Translate this page into:
Iontophoresis with topical 0.05% tretinoin for the management of recalcitrant palmar psoriasis: A report of two cases
Correspondence Address:
Aditya Kumar Bubna
Department of Dermatology, Sri Ramachandra University, Porur, Chennai - 600 116, Tamil Nadu
India
| How to cite this article: Bubna AK. Iontophoresis with topical 0.05% tretinoin for the management of recalcitrant palmar psoriasis: A report of two cases. Indian J Dermatol Venereol Leprol 2017;83:119-121 |
Sir,
Psoriasis is a chronic inflammatory disorder of the skin with variable presentation, and requires long-term treatment. The drugs utilized to clear psoriasis differ in their chemistry, route of administration, mode of action and adverse effect profile. In localized forms of psoriasis such as palmoplantar psoriasis, the treating clinician has to weigh the risks and benefits before initiating systemic therapy. The skin is semi-permeable and passive diffusion of topical drugs is poor on the palms and soles due to the stratum lucidum. Due to this, there could be a substantial deficit in therapeutic outcome. Combining topical therapy with physical modalities such as iontophoresis facilitates percutaneous absorption of drugs thereby enhancing drug penetration and causing quicker disease remission.
A 45-year-old man presented with scaly plaques on the palms for two years. They gradually progressed to the present condition [Figure 1a] and [Figure 1b]. He was treated with topical steroids and vitamin D3 analogues. The lesions recurred after an initial period of remission and were no longer responding to any topical medications. A lesional skin biopsy was consistent with psoriasis. He was counselled about iontophoresis treatment and the need for weekly adherence for two months, to which he agreed. A thin uniform layer of 0.05% tretinoin cream was applied over the right palm, and direct current from the iontophoresis unit [Figure - 2] was delivered using an ionto-roller probe. The indifferent electrode was clasped by the patient in his left hand to complete the circuit. The strength of the current was gradually increased until the patient experienced a mild tingling electrical sensation without any discomfort. In this study, the strength of the current was 7 milliamperes (mA) for the first session following which the strength was gradually increased by 0.5 mA per se ssion with the maximum current being 10.5 mA for the last session. As the ionto-roller was moved across the palm several times with gentle forward and backward strokes, tretinoin 0.05% cream gradually got absorbed with no trace of any visible drug on the surface. This was considered to be the end point. The same process was then repeated on the left palm. The duration of the entire procedure in both palms ranged from 15 to 20 minutes. Visible changes were noticed after about four sessions of this procedure. A total of eight once-weekly treatments were given over a period of two months. Between treatments, the patient was asked to apply white soft paraffin in the morning, and tretinoin 0.05% cream at bed time. The lesions had completely resolved after eight weeks [Figure 1c]. After this, the patient was advised to apply a urea-based cream in the morning, and to continue tretinoin 0.05% cream on alternate nights. The patient has completed one year of follow-up with no recurrence.
 |
| Figure 1a: Right palm of patient 1, prior tretinoin iontophoresis |
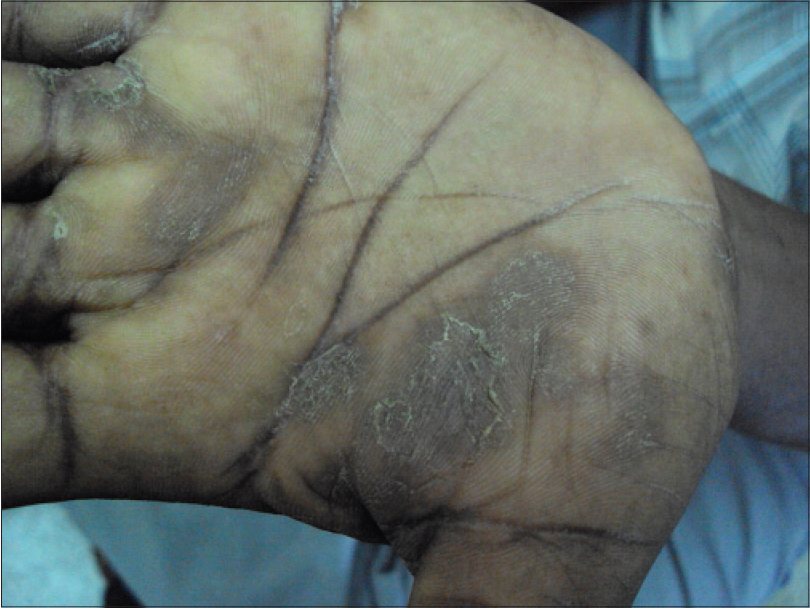 |
| Figure 1b: Left palm of patient 1, prior tretinoin iontophoresis |
 |
| Figure 1c: Both palms of patient 1, 8 weeks after tretinoin iontophoresis |
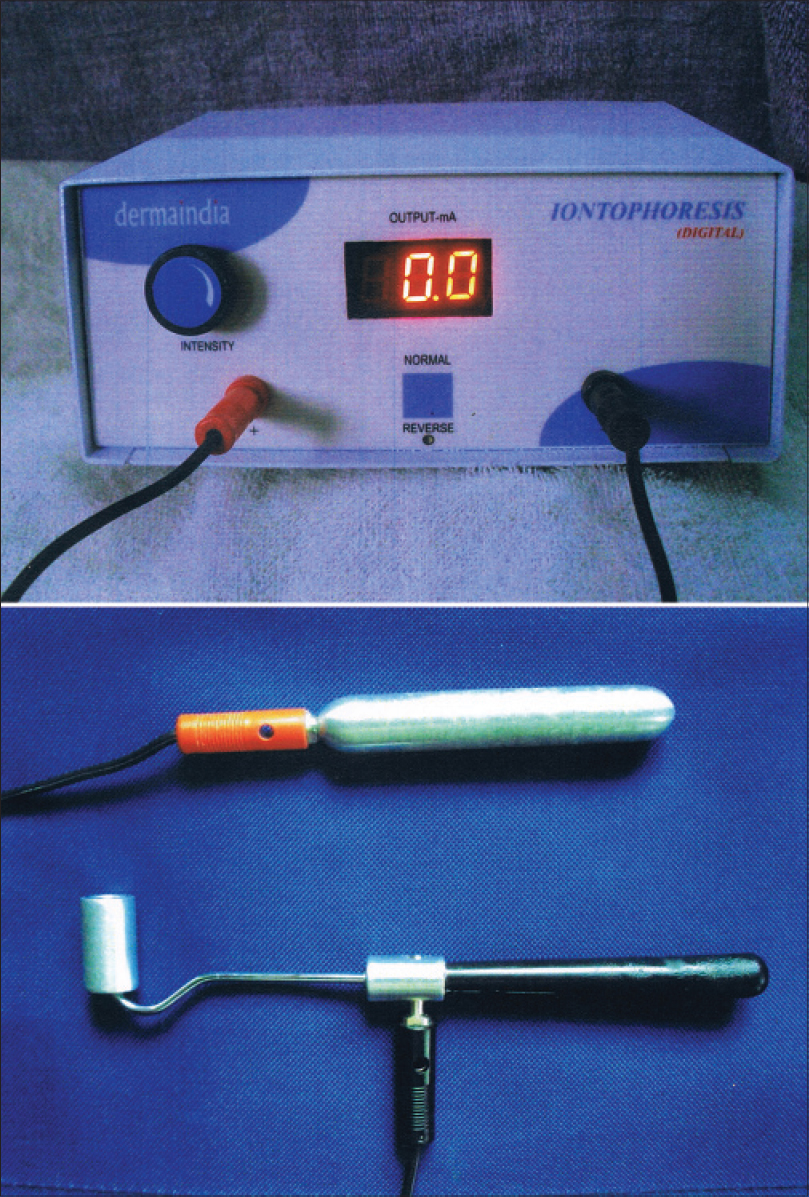 |
| Figure 2: Iontophoresis equipment used by the author for treating his patients |
The second patient was a 35-year-old woman with pruritic scaly lesions on both palms for one year [Figure 3a]. She had applied topical medications, like the previous patient, with an initial remission followed by a recurrence. The skin biopsy was suggestive of psoriasis. She was also treated with tretinoin iontophoresis. Her lesions demonstrated excellent resolution within eight weeks of treatment [Figure 3b]. The patient is still in remission after a year of follow-up.
 |
| Figure 3a: Both palms of patient 2, prior tretinoin iontophoresis |
 |
| Figure 3b: Both palms of patient 2, 8 weeks after tretinoin iontophoresis |
Cutaneous iontophoresis refers to the delivery of therapeutic drugs into the skin by applying a direct current to increase local concentrations of the drug. Tretinoin is a topical retinoid used for management of acne. It has been used with iontophoresis to treat atrophic scars of acne.[1] Although not marketed as a drug for the treatment of psoriasis, tretinoin has been found to demonstrate beneficial immunologic, anti-inflammatory and anti-keratinizing properties that could be utilized to facilitate regression of psoriatic lesions.[2]
A single case of psoriasis was reported to have responded very well to topical tretinoin 0.05% cream within six weeks of starting treatment with no relapse even after 3 months of follow up. PUVAsol, topical glucocorticoids and systemic methotrexate were previously tried in that patient with no improvement.[3] Iontophoresis utilizing methotrexate and cyclosporine A has been assessed in animal models and experimental studies but there have been only two reports that utilized iontophoresis with therapeutic drugs to manage psoriasis.[4],[5], The first was a case report where palmar psoriasis was successfully managed utilizing methotrexate iontophoresis and the second was a retrospective study of 31 patients where dexamethasone iontophoresis was used for treating nail psoriasis.[6],[7], Although there was a satisfactory improvement in psoriatic lesions, none of these reports mention the duration of remission.
A drawback of this therapeutic modality is the regular weekly follow-up required during the initial stages. Other limitations of this report are the small sample size of just two patients. A longer follow-up is required to check for recurrence. A need for further comparative randomized controlled trials with other penetration enhancers is required to demonstrate the effectiveness of this treatment modality. Given the toxicity profile of most antipsoriatic drugs, it would be worthwhile to explore this treatment modality in localized forms of psoriasis. Systemic therapy should be considered only if the therapeutic outcome is unsatisfactory. To conclude, this modality of treatment could help patients with localized psoriasis. It is a simple procedure that can be done in outpatient settings.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Schmidt JB, Donath P, Hannes J, Perl S, Neumayer R, Reiner A. Tretinoin-iontophoresis in atrophic acne scars. Int J Dermatol 1999;38:149-53.
[Google Scholar]
|
| 2. |
Koo J, Nguyen Q, Gambla C. Advances in psoriasis therapy. Adv Dermatol 1997;12:47-72.
[Google Scholar]
|
| 3. |
Raizada AK, Khurana VK, Sharma V, Gupta RK. Recalcitrant psoriasis treated with tretinoin 0.05% cream. Indian J Dermatol Venereol Leprol 1996;62:338.
[Google Scholar]
|
| 4. |
Wong TW, Zhao YL, Sen A, Hui SW. Pilot study of topical delivery of methotrexate by electroporation. Br J Dermatol 2005;152:524-30.
[Google Scholar]
|
| 5. |
Wang S, Kara M, Krishnan TR. Transdermal delivery of cyclosporine – A using electroporation. J Control Release 1998;50:61-70.
[Google Scholar]
|
| 6. |
Tiwari SB, Kumar BC, Udupa N, Balachandran C. Topical methotrexate delivered by iontophoresis in the treatment of recalcitrant psoriais – A case report. Int J Dermatol 2003;42:157-9.
[Google Scholar]
|
| 7. |
Le QV, Howard A. Dexamethasone iontophoresis for the treatment of nail psoriasis. Australas J Dermatol 2013;54:115-9.
[Google Scholar]
|
Fulltext Views
2,688
PDF downloads
1,489





![[Figure - 2]](#fig_ijdvl_2017_83_1_119_193614_f2.jpg){kind=link}