Translate this page into:
Primary cutaneous plasmablastic lymphoma presenting as perineal ulcero-proliferative growth in a human immunodeficiency virus-seropositive patient
2 Department of Pathology, Venereology and Leprology, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India
Correspondence Address:
Rashmi Kumari
Department of Dermatology, Venereology and Leprology, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry - 605 006
India
| How to cite this article: Behera B, Kumari R, Chandrashekar L, Thappa DM, Kar R, Rajesh NG. Primary cutaneous plasmablastic lymphoma presenting as perineal ulcero-proliferative growth in a human immunodeficiency virus-seropositive patient. Indian J Dermatol Venereol Leprol 2017;83:83-86 |
Sir,
A 33-year-old man, seropositive for human immunodeficiency virus, presented with a 4-month history of a rapidly growing, painful, ulcerated growth on the perineum associated with a foul smelling discharge. He was on antiretroviral therapy consisting of zidovudine, lamivudine and nevirapine for the past 2 months. On examination, he was emaciated and had generalized lymphadenopathy. Cutaneous examination revealed a 8 cm × 6 cm × 7 cm ulcero-proliferative growth in the perineal region. The overlying ulcer was indurated with a firm-to-hard base, rolled out border and yellowish slough in the ulcer floor [Figure - 1]. Some smaller erythematous nodules were present around the ulcerated lesion [Figure - 1], arrow]. The oral cavity and the rest of the cutaneous and systemic examination were within normal limits. A differential diagnosis of squamous cell carcinoma, orificial tuberculosis, deep fungal infection, Kaposi's sarcoma and lymphoma was considered. Laboratory evaluation revealed a leukocyte count of 5.2 × 10[9] cells/L, lactate dehydrogenase of 225 IU/L and CD4+ count of 323/mm [3]. Other investigations were within normal limits. Skin biopsy revealed diffuse dermal infiltration by large immunoblast-like cells with moderate amounts of cytoplasm, large nuclei, vesicular chromatin and a single prominent nucleolus. Features suggestive of a high-grade lymphoma such as “starry-sky” pattern, necrotic areas and apoptotic figures were evident throughout the lesion [Figure - 2]. Immunohistochemistry showed negative staining for CD19, CD20, CD2, CD3, CD5, CD30 and positive staining for CD138, CD38 and multiple myeloma oncogene-1 [Figure - 3]a,[Figure - 3]b,[Figure - 3]c. The immunohistochemistry for immunoglobulin light chain showed lambda light chain restriction [Figure - 4]a and was negative for kappa light chain [Figure - 4]b. Immunohistochemistry for Epstein–Barr virus-latent membrane protein was negative [Figure - 5]. The proliferative index marker Ki-67 was positive in more than 75% of the cells [Figure - 3]d. The lymph node biopsy showed a reactive pattern and bone marrow biopsy did not show any evidence of infiltration. A diagnosis of human immunodeficiency virus-associated primary cutaneous plasmablastic lymphoma was made. We planned to undertake magnetic resonance imaging of the lesion followed by excision and chemotherapy while continuing antiretroviral therapy. However, the patient refused further investigation and treatment.
 |
| Figure 1: Ulcero-proliferative growth in the perineal region with small nodules in the surrounding area (arrow) |
 |
| Figure 2a: Diffuse proliferation of lymphoid cells and presence of phagocytizing histiocytes imparting a “starry-sky pattern”; a feature typical of high grade neoplasm (H and E, ×100) |
 |
| Figure 2b: The proliferating lymphoid cells are of medium to large size, having moderate cytoplasm, large irregular nuclei and vesicular chromatin. Apoptotic cells and phagocytizing histiocytes are evident throughout the lesion (H and E, ×400) |
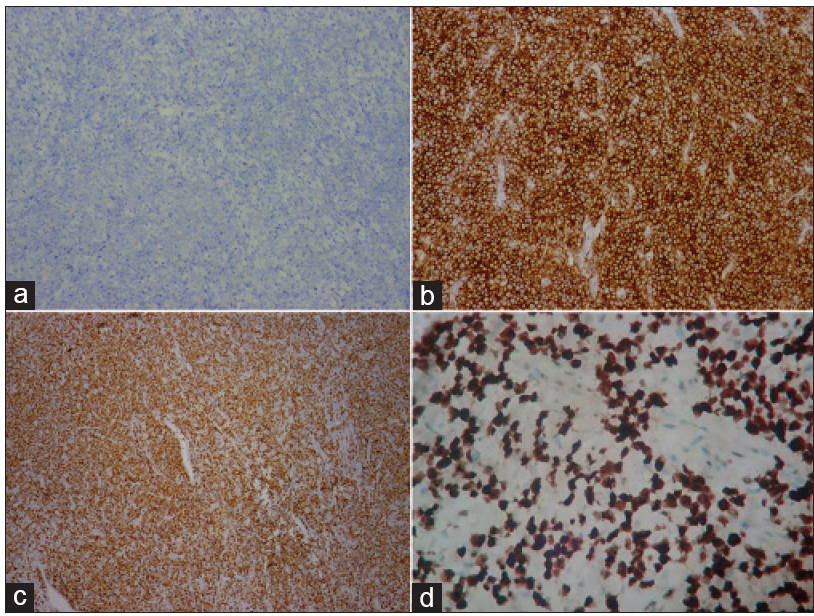 |
| Figure 3: Immunohistochemistry (IHC) of tumor cells demonstrating (a) negative CD20, (b) positive CD38, (c) positive multiple myeloma oncogene-1, (d) Ki67: marker of cell proliferation index is more than 75% (IHC, ×100) |
 |
| Figure 4: Immunohistochemistry (IHC) of tumor cells demonstrating lambda light chain restriction, (a) positive reactivity for lambda light chain and (b) negative reactivity for kappa light chain (IHC, ×100) |
 |
| Figure 5: Immunohistochemistry (IHC) of tumor cells demonstrating negative reactivity to Epstein–Barr virus-latent membrane protein (IHC, ×100) |
Plasmablastic lymphoma is a distinct subtype of diffuse large B-cell lymphoma characterized by a diffuse proliferation of large neoplastic cells that mostly have the morphology of B-cell immunoblasts but have a plasma cell immune phenotype.[1] It is strongly associated with human immunodeficiency virus infection, constitutes around 2% of all human immunodeficiency virus-related lymphomas and is considered one of the acquired immune deficiency syndrome (AIDS)-defining illnesses.[2]
The exact pathogenesis of human immunodeficiency virus-associated plasmablastic lymphoma is poorly understood. It comprises a complex interaction between genetic abnormalities, chronic immune stimulation, human immunodeficiency virus-related immunodeficiency and co-infecting oncogenic viruses (Epstein–Barr virus and probably human herpes virus-8).[3],[4], The association of Epstein–Barr virus with plasmablastic lymphoma is best demonstrated by the expression of Epstein–Barr virus encoded ribonucleic acid rather than latent membrane protein as the latter is usually negative, as in our case. The association with Epstein-Barr virus is more commonly seen in human immunodeficiency virus-positive plasmablastic lymphoma (75%) and post-transplant plasmablastic lymphoma (67%) than in immunocompetent patients (50%). The actual prevalence of human herpes virus 8 infection in plasmablastic lymphoma is controversial.[5]
In their review, Castillo et al. categorized patients of plasmablastic lymphoma into four groups, human immunodeficiency virus-positive plasmablastic lymphoma, human immunodeficiency virus-negative plasmablastic lymphoma, post-transplant plasmablastic lymphoma and transformed plasmablastic lymphoma, depending on their immunological status.[2] Out of 590 cases of plasmablastic lymphoma, 369 were human immunodeficiency virus-seropositive, 164 were human immunodeficiency virus-negative, 37 patients were post-transplant and 20 were in the transformed group. In all groups, males were commonly affected than females but in human immunodeficiency virus-negative plasmablastic lymphoma, females were relatively more affected than in other groups. In comparison to the human immunodeficiency virus-positive plasmablastic lymphoma, relatively older patients were affected in the human immunodeficiency virus-negative group (mean age of presentation was 55 years). The mean age of presentation in both post-transplant and transformed plasmablastic lymphoma groups were 62 years.[2] In contrast to human immunodeficiency virus-positive plasmablastic lymphoma, extranodal involvement was most common (95% of patients) with 48% having oral cavity/jaw involvement, 12% having gastrointestinal tract disease and 6% having skin involvement. In 7% of the patients, plasmablastic lymphoma was the initial presentation of human immunodeficiency virus infection. More than half (65%) of the patients had advanced disease (stage III or IV) at presentation, and 40% had bone marrow involvement and B symptoms.[2] Plasmablastic lymphoma affects the oral cavity with fast local invasion and dissemination. Other less commonly involved sites were the central nervous system, paranasal sinuses, mediastinum, liver, lungs and testes.[1] Our patient presented with a rapidly enlarging ulcero-proliferative growth in the perineum without involvement of the gastrointestinal tract. In human immunodeficiency virus-negative plasmablastic lymphoma, although the oral cavity is commonly involved, involvement of extra-nodal sites is more heterogeneous. In addition, in human immunodeficiency virus-positive plasmablastic lymphoma, bone marrow involvement, B symptoms and advanced clinical stage at presentation are more common than in the human immunodeficiency virus-negative plasmablastic lymphoma.[2] Around 41 cases of plasmablastic lymphoma that involved the skin have been reported, of which 22 cases were seropositive for human immunodeficiency virus. Cutaneous involvement is relatively more common in the case of post-transplant plasmablastic lymphoma (8 cases, 22%) than in human immunodeficiency virus-positive plasmablastic lymphoma (22 cases, 6%), human immunodeficiency virus-negative plasmablastic lymphoma (10 cases, 7%) and transformed plasmablastic lymphoma (1 case, 5%).[2] Plasmablastic lymphoma with cutaneous involvement has a male preponderance and is commonly associated with Epstein–Barr virus infection. It has a rare association with human herpes virus 8.[6],[7], Reddish-purple nodules involving the lower limb was the common presenting feature of cutaneous plasmablastic lymphoma. We were unable to find any previous reports of plasmablastic lymphoma presenting as a perineal ulcero-proliferative growth; however, there have been reports of plasmablastic lymphoma involving the testis and penis.[8],[9],
Differential diagnosis of an ulcero-proliferative growth in the perineal region includes epidermoid carcinoma, lymphoma, adenocarcinoma, basaloid carcinoma, melanoma and metastasis.[4] The histology of plasmablastic lymphoma is characterized by monomorphic cellular proliferation of large immunoblasts or large plasma cells, as seen in our case. Apoptotic bodies and mitotic figures are frequent. The neoplastic cells express plasma cell markers (VS38c, CD38, multiple myeloma oncogene-1, BLIMP1, XBP-1, cytoplasmic immunoglobulin and CD138), stain variably for CD79a, CD56, CD45, CD10, CD30, Epstein–Barr virus-encoded small ribonucleic acids and stain negative for B-cell markers (CD20 and PAX5).[5],[10], The various morphologic and immunophenotypic differentials of plasmablastic lymphoma are primary cutaneous diffuse large B-cell lymphoma-leg type, primary cutaneous diffuse large B-cell lymphoma-not otherwise specified, plasmablastic and anaplastic variants of plasma cell myeloma and plasmacytoma, myeloid sarcoma and metastatic melanoma.[2],[5],[6] Primary cutaneous diffuse large B-cell lymphoma (both leg type and not otherwise specified) can be excluded by the characteristics of CD20 and leukocyte common antigen positivity and negativity for plasma cell markers such as CD138. The presence of significant bone involvement, a monoclonal serum paraprotein, lower proliferation index, positive staining for CD56 and negative staining for Epstein–Barr virus favor a diagnosis of plasma cell myeloma. Negative staining for myeloperoxidase and S-100 rules out myeloid sarcoma and metastatic melanoma, respectively.[2],[5],[6]
Patients having plasmablastic lymphoma have a poor prognosis. Prognosis largely depends on the advanced stage and human immunodeficiency virus status does not appear to affect the outcome.[2] Standard cyclophosphamide, hydroxydaunorubicin (doxorubicin), vincristin and prednisone (CHOP) therapy is considered inadequate for the treatment of plasmablastic lymphoma and recent guidelines recommend more intensive regimens. These include cyclophosphamide, vincristine, doxorubicin, methotrexate alternating with ifosfamide, etoposide and cytarabine, hyperfractionated cyclophosphamide, vincristine, doxorubicin and dexamethasone alternating with methotrexate and cytarabine or dose-adjusted etoposide, prednisone, doxorubicin, cyclophosphamide and vincristine.[2]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Castillo JJ, Reagan JL. Plasmablastic lymphoma: A systematic review. ScientificWorldJournal 2011;11:687-96.
[Google Scholar]
|
| 2. |
Castillo JJ, Bibas M, Miranda RN. The biology and treatment of plasmablastic lymphoma. Blood 2015;125:2323-30.
[Google Scholar]
|
| 3. |
Loghavi S, Alayed K, Aladily TN, Zuo Z, Ng SB, Tang G, et al. Stage, age, and EBV status impact outcomes of plasmablastic lymphoma patients: A clinicopathologic analysis of 61 patients. J Hematol Oncol 2015;8:65.
[Google Scholar]
|
| 4. |
Chagas LA, Camilo GB, Machado DC, Vidal DR, de Oliveira CE, Toledo GC, et al. Plasmablastic lymphoma of the anal canal in an HIV-infected patient. Am J Case Rep 2014;15:543-9.
[Google Scholar]
|
| 5. |
Elyamany G, Al Mussaed E, Alzahrani AM. Plasmablastic lymphoma: A review of current knowledge and future directions. Adv Hematol 2015;2015:315289.
[Google Scholar]
|
| 6. |
Tiong IS, Strauss M, Lau MB, Chiruka S. Cutaneous plasmablastic lymphoma in an immunocompetent patient with long-term pyrimethamine use for essential thrombocythemia: A case report and literature review. Case Rep Hematol 2013;2013:541783.
[Google Scholar]
|
| 7. |
Black CL, Foster-Smith E, Lewis ID, Faull RJ, Sidhu SK. Post-transplant plasmablastic lymphoma of the skin. Australas J Dermatol 2013;54:277-82.
[Google Scholar]
|
| 8. |
Sugimoto K, Koike H, Esa A. Plasmablastic lymphoma of the right testis. Int J Urol 2011;18:85-6.
[Google Scholar]
|
| 9. |
Sun J, Medeiros LJ, Lin P, Lu G, Bueso-Ramos CE, You MJ. Plasmablastic lymphoma involving the penis: A previously unreported location of a case with aberrant CD3 expression. Pathology 2011;43:54-7.
[Google Scholar]
|
| 10. |
Hsi ED, Lorsbach RB, Fend F, Dogan A. Plasmablastic lymphoma and related disorders. Am J Clin Pathol 2011;136:183-94.
[Google Scholar]
|
Fulltext Views
2,117
PDF downloads
1,302





![[Figure - 1]](#fig_ijdvl_2017_83_1_83_192953_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2017_83_1_83_192953_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2017_83_1_83_192953_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2017_83_1_83_192953_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2017_83_1_83_192953_f5.jpg){kind=link}