Translate this page into:
Multiple elastomas in a 6-month-old child
2 Department of Pathology, Lady Hardinge Medical College, New Delhi, India
Correspondence Address:
Ram Chander
Department of Dermatology and STD, Lady Hardinge Medical College and Assoc. Hospitals, New Delhi - 110 001
India
| How to cite this article: Garg T, Chander R, Jain A, Nangia A, Mal J. Multiple elastomas in a 6-month-old child. Indian J Dermatol Venereol Leprol 2010;76:578-579 |
Sir,
Connective tissue nevi can either occur as isolated lesions or form a part of inherited syndromes like Buschke-Ollendorff syndrome (BOS). We report a case of multiple juvenile elastomas in a 6-month-old child, which could be a forme fruste of BOS, for its peculiar and rare presentation.
A 6-month-old girl, product of a non-consanguineous marriage, presented with multiple asymptomatic, raised skin lesions all over the body, since birth. The skin lesions did not increase in number; however, they increased in size, proportionate to the body growth. The cutaneous examination showed multiple skin colored to yellowish, round to oval, soft to firm, discrete papules and plaques, scattered all over, with relatively more involvement of the face and trunk [Figure - 1]. The ophthalmological examination was normal. The histopathology of the plaque did not reveal any abnormality on routine hematoxlin and eosin staining. However, special staining with Verhoeff van-Gieson stain showed thick interlacing bundles of elastic fibers running between the normal collagen bundles [Figure - 2]. The skeletal survey did not show areas of increased opacities or any other abnormality. The hemogram, serum biochemistry and calcium levels were normal. Other members in the family, including the parents and two siblings, did not have any skin lesions, but they could not be screened radiologically.
 |
| Figure 1 : Multiple skin colored to yellowish, discrete papules and plaques |
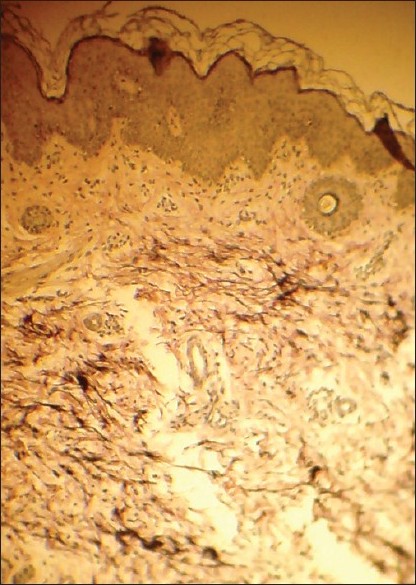 |
| Figure 2 : Verhoeff van-Gieson stain section showing thick interlacing bundles of elastic fibers |
BOS is a rare autosomal-dominant disorder, characterized by connective tissue nevi (elastomas) and osteopoikilosis. It has been shown that patients with BOS can have skin lesions alone or only bone involvement without any skin lesions. [1] BOS is caused due to loss of function mutation in the LEMD3 gene on chromosome 12q14.
BOS can either present as symmetrical, small, asymptomatic lichenoid papules resembling pseudoxanthoma elasticum known as "dermatofibrosis lenticularis disseminative" [2] or as large asymmetrical, yellowish plaques or nodules. The lesions are usually present on the trunk, proximal extremities and skin folds. They may be present since birth. Histopathologically, it may present as increased, broad and interlacing elastic fibers, diminished and fragmented fibers or, at times, normal elastin. Collagen bundles can be thickened or normal. [3] Giro et al. [4] showed that levels of tropoelastin and elastin mRNA were increased in the fibroblasts. On the other hand, Ohnishi et al. [5] found normal elastin mRNA levels in the elastic nevi without osteopoikilosis and proposed that elastic nevi without skeletal involvement might be etiologically different from that of BOS.
Osteopoikilosis is seen as well-circumscribed areas of increased opacities affecting mainly the carpals, tarsals, phalanges, epiphyses and metaphyses of long bones and pelvis. These changes manifest during late childhood or puberty. [1],[2],[3],[4],[5]
Our patient had multiple elastomas manifesting as skin colored to yellowish plaques and few papules scattered all over the body. There were no nodular lesions. The involvement was very extensive. At the initial presentation, the possibilities of cutaneous mucinosis of infancy, mastocytosis, histiocytosis and juvenile elastomas were suspected. It was only after a completely normal histopathology and positive staining with Verhoeff van-Gieson stain that the other possibilities were ruled out.
To the best of our knowledge, this kind of clinical presentation, with such extensive distribution and presence of both papules and plaques, has not been described previously. The girl had no osteopoikilosis at presentation. We assume that either she had multiple juvenile elastomas occurring independently or was a forme fruste of BOS, as the radiological defect in this condition appears late. Therefore, a postpubertal radiological examination should be carried out in all patients having multiple juvenile elastomas. The importance of diagnosing this entity lies in the fact that, radiologically, opacities seen in BOS, which appear late in life, may mimic secondary metastasis in the bones; however, the skeletal involvement in this condition is purely benign in nature.
There is little evidence of any increased morbidity or mortality in the case of BOS. [1],[2],[3],[4],[5] Diagnosis is made by a complete clinical history, examination and skeletal survey of the patient and their family. As the skeletal changes manifest late in childhood, all the newborns presenting with localized or generalized elastomas should be thought of as a possible case of BOS and the family should be screened clinically and radiologically. The child should also be under regular follow-ups. As the lesions are asymptomatic, no specific treatment is required.
Our case highlights the rare presentation of a rare entity.
| 1. |
Woodrow SL, Pope FM, Handfield-Jones SE. The Buschke-Olendorff syndrome presenting as familial elastic naevi. Br J Dermatol 2001;122:890-3.
[Google Scholar]
|
| 2. |
Ramme K, Kolde G, Stadler R. [Dermatofibrosis lenticularis disseminata with osteopoikilosis. Buschke-Olldendorff syndrome] Hautarzt 1993;44:312-4.
[Google Scholar]
|
| 3. |
Kawamura A, Ochiai T, Tan-Kinoshita M, Suzuki H. Buschke-Ollendroff syndrome: Three generations in a Japanese family. Pediatr Dermatol 2005;22:133-7.
[Google Scholar]
|
| 4. |
Giro MG, Duvic M, Smith LT, Kennedy R, Rapini R, Arnett FC, et al. Buschke-Ollendorff syndrome associated with elevated elastin production by affected skin fibroblasts in culture. J Invest Dermatol 1992;99:129-37.
[Google Scholar]
|
| 5. |
Ohnishi Y, Akiyama M, Tajima S, Ishibashi A, Seyama Y. Elastic nevus with normal expression of elastin and elastin related proteins mRNAs. Dermatology 1999;198:307-9.
[Google Scholar]
|
Fulltext Views
1,840
PDF downloads
1,233





![[Figure - 1]](#fig_ijdvl_2010_76_5_578_69077_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2010_76_5_578_69077_f2.jpg){kind=link}