Translate this page into:
Coexistence of onychomycosis in psoriatic nails: A descriptive study
2 Department of Dermatology and STD, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Puducherry - 605 006, India
3 Department of Pathology, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Puducherry - 605 006, India
Correspondence Address:
Devinder Mohan Thappa
Department of Dermatology and STD, JIPMER, Puducherry - 605 006
India
| How to cite this article: Natarajan V, Nath AK, Thappa DM, Singh R, Verma SK. Coexistence of onychomycosis in psoriatic nails: A descriptive study. Indian J Dermatol Venereol Leprol 2010;76:723 |
Abstract
Background: Psoriatic nail changes predispose to onychomycosis because it becomes easier for fungi to penetrate an already compromised nail plate. Moreover, some of the psoriatic nail changes closely resemble onychomycosis. Aim: To investigate cases of nail psoriasis for any evidence of onychomycosis. Methods: Seventy-two patients with psoriasis were included in the study. The patients were selected from the psoriasis clinic and dermatology in-patient ward. Direct microscopic examination with 20% KOH and culture were carried out in all patients showing psoriatic nail changes. Histopathological examination with Periodic Acid-Schiff (PAS) stain was done in cases negative by KOH examination and culture. Results: Nail changes were seen in 66.66% (48/72) of psoriasis patients. The most common fingernail changes observed were pitting, onycholysis and subungual hyperkeratosis, and the most common toenail changes were onycholysis and subungual hyperkeratosis. Nail changes were significantly more common in males. The duration of skin lesions of psoriasis and Psoriasis Area Severity Index scores were significantly higher in patients with nail changes. Out of 48 patients with psoriatic nail change, 23 (47.91%) had investigative evidence of onychomycosis. The fungal isolates on culture were non-dermatophytic molds in nine patients (18.75%) and yeast like fungi also in nine patients (18.75%). Conclusion: Coexistent onychomycosis in psoriatic nails does occur.Introduction
Psoriasis is associated with nail changes in significant proportion of cases, and the frequency is much higher in the presence of psoriatic arthropathy. [1],[2] While most of the nail changes occurring in psoriasis are due to the psoriatic process involving the nail unit, other factors may play a considerable role in the induction or worsening of psoriatic nail disease. Onychomycosis, an infection of the nail unit by dermatophytic as well as non-dermatophytic fungi, has been found to be associated with psoriatic nail changes in several studies. [3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14] Psoriatic nail disease may be a predisposing condition for secondary invasion by the fungi. Many psoriatic patients have nail changes which morphologically resemble onychomycosis, and in such patients further differential diagnostic procedures are essential to exclude the presence of coexisting fungal infection. Onychomycosis playing a role in the initiation or the worsening of nail changes in psoriasis patients is also possible but it is more difficult to substantiate. The present study was carried out to study the presence of investigative evidence of onychomycosis in psoriatic nail.
Methods
Seventy-two patients with psoriasis were included in the study over a period of 4 months (June 2009-September 2009). The patients were selected from the psoriasis clinic and dermatology in-patient ward. Those patients who were on systemic antifungal treatment for any indication and/or on topical antifungal treatment for onychomycosis within the period of last 4 weeks were excluded from the study.
After obtaining informed consent, detailed history was obtained in all cases and detailed clinical examination of the nails was done. Severity of nail disease was scored by Nail Psoriasis Area Severity Index (NAPSI), as proposed by Rich and Scher. [15] The severity of skin disease was scored according to the Psoriasis Area Severity Index (PASI).
Only those patients with any psoriatic nail change were evaluated further for onychomycosis. A maximum of two finger nails and two toenails with the suspicion of onychomycosis were selected for evaluation. Samples were collected with a sterile nail clipper after disinfecting the nail with 70% alcohol. The nail samples collected were transported in a sterile pouch made out of paper to microbiology lab and in 10% formalin solution to pathology lab. All specimens were subjected to direct microscopy in 20% KOH [Figure - 1] to determine the presence of fungal elements. The specimens were cultured in two tubes containing Sabouraud′s Dextrose Agar (SDA), with and without cycloheximide, respectively. The culture tubes were incubated at 25°C and examined daily for 4 weeks. Growth of non-dermatophytic molds in culture was considered significant only if "simple association" evaluation criterion was met, i.e., non-dermatophytic fungal outgrowth was considered etiologic whenever direct microscopy was positive for fungal elements and no dermatophyte could be cultured from the initial specimen. [16] Confirmation of Candida species required positive culture and observation of pseudomycelium under light microscopy with 20% KOH. If onychomycosis was strongly suspected on clinical grounds but microscopy and culture were negative, histological examination of the affected nail material was carried out by Periodic Acid-Schiff (PAS) staining [Figure - 2].
 |
| Figure 1 :Direct microscopy with 20% KOH showing budding yeast cells |
 |
| Figure 2 :Nail clipping histopathology with PAS stain showing fungal hyphae (×400) |
Diagnosis of onychomycosis was made if both direct microscopy with 20% KOH and culture were positive, or histological examination with PAS demonstrated fungal elements in cases negative by direct microscopy and culture.
Results
Mean age of the patients in our study was 48.4 years (with a range of 5.5-75 years). Male to female ratio was 3.8:1 (57 males and 15 females). Majority of the patients were farmers (35/72, 48.6%), followed by housewives (8/72, 11.1%), retired clerks (6/72, 8.3%), businessmen (5/72, 6.9%), and miscellaneous (carpenter, clerk, driver, weaver, barber, electrician, mechanic, student, rice mill worker, shop owner, street play actor, tailor and waiter).
The most common type of psoriasis found was psoriasis vulgaris (61/72, 84.7%) followed by psoriatic erythroderma (5/72, 6.9%), scalp psoriasis (two cases), inverse psoriasis (two cases), palmoplantar psoriasis (one case), and generalized pustular psoriasis (one case). Six patients (8.3%) also had psoriatic arthritis. The mean duration of skin changes was found to be 9.63 years (range of 1 month-49 years).
Forty-eight (66.66%) out of 72 patients had nail involvement. Five out of 6 patients with psoriatic arthritis had nail changes. The mean duration of nail changes was 6.10 years (range of 10 days-49 years). Eighteen patients (18/48, 37.5%) developed skin lesions and nail changes simultaneously. In the remaining 30 patients (62.5%), nails changes developed after the onset of skin lesions, the mean time interval between onset of skin and nail changes being 8.234 years. Onycholysis (44.79%), subungual hyperkeratosis (32.91%) and pitting (29.06%) were the most common nail (toe and finger nails included) changes. The most common fingernail change observed was pitting (54.3%), followed by onycholysis (51.25%) and subungual hyperkeratosis (35%) [Figure - 3] and [Figure - 4]. On the contrary, most common toenail changes observed were onycholysis (38.3%) and subungual hyperkeratosis (30.83%). Pitting, onycholysis, splinter hemorrhage and salmon patch were significantly more common (P < 0.0001 for all four type of nail changes) in fingernails as compared to toenails. Beau′s line was significantly more common in fingernails (P value= 0.0030).
 |
| Figure 3 :Pitting, onycholysis and salmon patch |
 |
| Figure 4 :Subungual hyperkeratosis involving the fingernails |
The mean PASI score of 72 patients was 9.98 (range of 0.3-62.4). The mean of total NAPSI score (finger and toenails) of 48 patients with nail changes was 32.77 (range of 7-69). Mean NAPSI scores for fingernails and toenails were 21.5 and 11.58, respectively. There was no correlation between PASI and their respective total NAPSI scores. However, the mean PASI of patients with nail changes was found to be significantly higher (P < 0.0001). It was found that nail changes were significantly more common in males than in females (P value 0.0006). Duration of psoriatic skin lesions was significantly longer in patients with nail changes (mean duration 11.42 years) than in those without nail changes (mean duration 6.05 years) (P value 0.002). No significant difference was found in the mean NAPSI score between males and females, patients with and without psoriatic arthritis, and between patients selected from in-patient and out-patient departments.
Out of 72 patients, 19 (26.4%) gave a history of trauma to nails. Twenty-nine out of 48 patients (60.4%) reported that their nail changes improved with the systemic medications used for skin lesions. Diabetes mellitus and hypertension were found to be the most commonly associated systemic illnesses (8/72 cases each), whereas eczema, contact dermatitis and pitted keratolysis were commonly seen associated dermatoses (2/72 cases each).
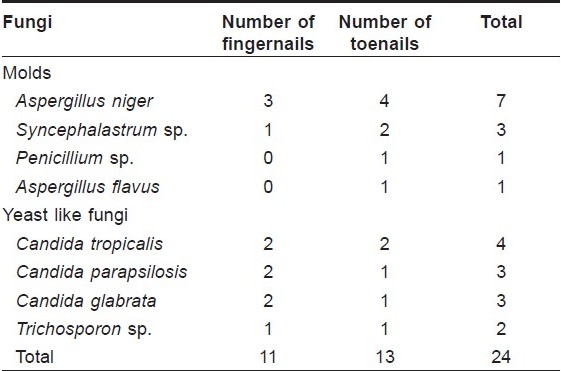
Out of 48 patients with psoriatic nail change, evidence of onychomycosis as per the diagnostic criteria was found in 23 patients (47.91%) [Table - 1]. Fungal culture grew only non-dermatophytic molds and yeast like fungi (9/48, 18.75% each) [Table - 2]. No statistical correlations were found between the presence of onychomycosis and duration of nail changes, NAPSI scores, age, presence of onycholysis, presence of subungual hyperkeratosis or trauma to nail.

Discussion
The presence of fungal nail infection in psoriatic nails and its significance is a matter of controversy. Previous studies reported a prevalence rate of onychomycosis to be 4.6-30% in patients with psoriatic nail disease. [3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14] In the present survey, we found nail fungal infection in 47.91% of psoriatic patients with nail psoriasis. This figure is slightly higher than that reported in many other studies, and this could be because of the features of study population (majority of the patients were farmers, housewives and in other occupations involving manual work which may independently increase the risk of onychomycosis). The prevalence of onychomycosis in the general population of India as such is 0.5-45%. [17]
Kacar et al.[3] found that nail changes were more severe in patients with onychomycosis, suggesting that the presence of fungal infection may intensify nail psoriasis through koebner effect. We could not find any significant difference in the NAPSI scores (signifying the severity of nail disease) between these two groups in our study; hence, we suggest that the severity of nail infection cannot be used as a marker for onychomycosis, a finding which was also reported by Larsen et al.[4]
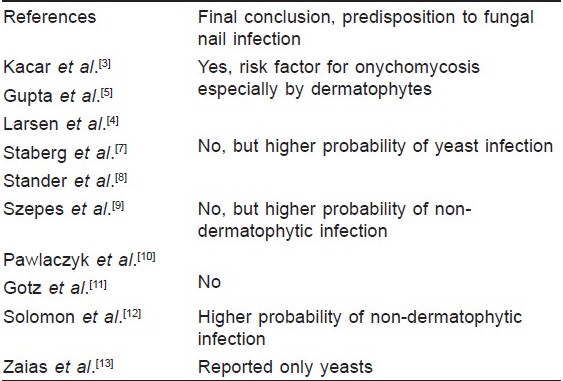
There is a considerable amount of difference in the reports of various studies on the role of onychomycosis in psoriasis nails and vice versa [Table - 3]. Gupta et al,[5] and Kacar et al,[3] concluded that nail psoriasis constituted a risk factor for onychomycosis specifically by dermatophytes. In our study, however, no dermatophytes were cultured. Other case control studies by Larsen et al,[4] Staberg et al,[7] and Stander et al,[8] reported a higher probability of yeast infection, while Szepes [9] reported a higher probability of non-dermatophytic infection in psoriatic nails, but they all also concluded that the frequency of onychomycosis in psoriatic patients did not differ from the occurrence of onychomycosis in non-psoriatics. Pawlaczyk et al,[10] and Gotz et al,[11] reported that there was no altered susceptibility to onychomycosis in patients with psoriatic nail changes. Some descriptive studies like that of Solomon et al,[12] concluded that there was a higher probability of non-dermatophytic infection in psoriatic patients and Zaias et al,[13] reported no dermatophytes and some yeasts. In our study, we found only non-dermatophytic molds and yeast like fungi (18.75% each).
There could be several reasons for the preferential invasion of psoriatic nails by non-dermatophytes and yeasts. It is known that serum-like glycoprotein has an inhibitory effect on dermatophytes, but with no effect on yeasts. [12] An in vitro study showed that dermatophytes do not grow readily on nail material collected from psoriatic nails as compared with non-psoriatic nail. [18] It is also believed that the fast turnover of the nails in psoriasis patients theoretically may constitute an effective defence against dermatophytes. It is also suggested that altered subungual tissue and onycholysis may facilitate yeast invasion. But we did not find any significant difference in the occurrence of onychomycosis in patients with or without onycholysis or subungual hyperkeratosis. An immunosupressed state caused by of the intake of methotrexate may also play a role in the occurrence of onychomycosis.
Ours was a descriptive type of study and could have been strengthened if done comparatively with a larger sample size. "Simple association criteria" [16] were used to make the final diagnosis of onychomycosis with a sensitivity of 53.6% and a specificity of 70.3% for non-dermatophytic fungal (the only species isolated in our study) infections, which is predictive enough. Repeated culture was beyond the scope of the study or else the diagnostic criteria could be strengthened by using the "Classic evaluation Criterion". [16] From this study, it is difficult to conclude whether nail psoriasis is a risk factor for onychomycosis but psoriatic nails do have an increased susceptibility for secondary invasion by non-dermatophytic and yeast like fungi.
Based on our findings and other reports, it is important to consider coexistent fungal infection in psoriatic nails and treat if clinically appropriate, considering the fact that both have negative synergistic effect on the nail architecture. Further, a study to analyze whether psoriatic nails with coexistent onychomycosis show any morphological improvement when put on antifungal treatment will help elaborate the therapeutic importance of this finding. However, it seems that the therapy must be prescribed with caution as some systemic antifungal agents such as terbinafine may exacerbate psoriasis. [19]
Acknowledgment
This project was carried out under Indian council of Medical Research (ICMR), Short Term Studentship (STS), 2009.
| 1. |
Scher RK. Psoriasis of the nail. Dermatol Clin 1985;3:387-94.
[Google Scholar]
|
| 2. |
Lavaroni G, Kokelj F, Pauluzzi P, Trevisan G. The nail in psoriatic arthritis. Acta Derm Venereol Suppl 1994;186:113.
[Google Scholar]
|
| 3. |
Szepietowski JC, Solomon J. Do fungi play a role in psoriatic nails? Mycoses 2007;50:437-42.
[Google Scholar]
|
| 4. |
Kacar N, Ergin S, Ergin C, Erdogan BS, Kaleli I. The prevalence, aetiological agents and therapy of onychomycosis in patients with psoriasis: A prospective controlled trial. Clin Exp Dermatol 2007;32:1-5.
[Google Scholar]
|
| 5. |
Larsen GK, Haedersdal M, Svejgaard EL. The prevalence of onychomycosis in patients with psoriasis and other skin diseases. Acta Derm Venereol 2003;83:206-9.
[Google Scholar]
|
| 6. |
Gupta AK, Lynde CW, Jain HC, Sibbald RG, Elewski BE, Daniel CR 3 rd , et al. A higher prevalence of onychomycosis in psoriatics compared with non-psoriatics: Multicentre study. Br J Dermatol 1997;136:786-9.
[Google Scholar]
|
| 7. |
Staberg B, Gammeltoft M, Onsberg P. Onychomycosis in patients with psoriasis. Acta Derm Venereol 1983;63:436-8.
[Google Scholar]
|
| 8. |
Stδnder H, Stδnder M, Nolting S. Incidence of fungal involvement in nail psoriasis. Hautarzt 2001;52:418-22.
[Google Scholar]
|
| 9. |
Szepes E. Mycotic infections of psoriatic nails. Mykosen 1986;29:82-4.
[Google Scholar]
|
| 10. |
Pawlaczyk M, Rokowska A, Chmielewska I, Janicka D, Gutowska-Ryters A. Does onychomycosis more frequently affect patients suffering from psoriasis? Mikol Lek 2006;13:82.
[Google Scholar]
|
| 11. |
Gφtz H, Patiri C, Hantschke D. The growth of Deramatophyten on normal and psoriatiatischem nail keratin. Mykosen 1974;17:373-7.
[Google Scholar]
|
| 12. |
Salomon J, Szepietowski JC, Proniewicz A. Psoriatic nails: A prospective clinical study. J Cutan Med Surg 2003;7:317-21.
[Google Scholar]
|
| 13. |
Zaias N. Psoriasis of the nail: A clinical-pathological study. Arch Dermatol 1969;99:567-79.
[Google Scholar]
|
| 14. |
Sαnchez-Regaρa ML, Videla S, Villoria J, Domingo H, Macaya A, Ortiz E, et al. Prevalence of fungal involvement in a series of patients with nail psoriasis. Clin Exp Dermatol 2008;33:194-5.
[Google Scholar]
|
| 15. |
Rich P, Scher RK. Nail Psoriasis Severity Index: A useful tool for evaluation of nail psoriasis. J Am Acad Dermatol 2003;49:206-12.
[Google Scholar]
|
| 16. |
Summerbell RC, Cooper E, Bunn U, Jamieson F, Gupta AK. Onychomycosis: A critical study of techniques and criteria for confirming the etiologic significance of nondermatophytes. Med Mycol 2005;43:39-59.
[Google Scholar]
|
| 17. |
Kaur R, Kashyap B, Bhalla P. Onychomycosis- epidemiology, diagnosis and management. Indian J Med Microbiol 2008;26:108-16.
[Google Scholar]
|
| 18. |
Hamnerius N, Berglund J, Faergemann J. Pedal dermatophyte infection in psoriasis. Br J Dermatol 2004;150:1125-8.
[Google Scholar]
|
| 19. |
Szepietowski J. Terbinafine exacerbates psoriasis: Case report with a literature review. Acta Dermatovenerol Croat 2003;11:17-21.
[Google Scholar]
|
Fulltext Views
4,462
PDF downloads
2,111





![[Figure - 1]](#fig_ijdvl_2010_76_6_723_72468_f4.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2010_76_6_723_72468_f5.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2010_76_6_723_72468_f6.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2010_76_6_723_72468_f7.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2010_76_6_723_72468_t1.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2010_76_6_723_72468_t2.jpg){kind=link}
![[Table - 3]](#tbl_ijdvl_2010_76_6_723_72468_t3.jpg){kind=link}