
Translate this page into:
Concomitant occurrence of frontal fibrosing alopecia and trichotemnomania: The importance of trichoscopy
Corresponding author: Dr. María Librada Porriño-Bustamante, Hospital Universitario La Zarzuela, Calle de Pleyades, 25, 28023, Madrid, Spain. mporrinobustamante@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Porriño-Bustamante ML, Arias-Santiago S, Buendía-Eisman A. Concomitant occurrence of frontal fibrosing alopecia and trichotemnomania: The importance of trichoscopy. Indian J Dermatol Venereol Leprol 2021;87:112-115.
Sir,
Frontal fibrosing alopecia (FFA) is a scarring alopecia characterized by the recession of the frontal and/or temporal hairline. The absence of vellus hair in the hairline is a common finding. Some patients retain hairs along the frontotemporal rim, which is named the pseudo “fringe sign.”1 FFA has been reported occurring concurrently with other types of alopecia, especially androgenetic alopecia (AGA), lichen planopilaris, discoid lupus erythematosus and alopecia areata.2
Trichotemnomania is an obsessive-compulsive habit of cutting or shaving one’s own hair with scissors or a razor. Literature search shows that concurrent occurrence of FFA and trichotemnomania has not been reported so far.
A 46-year-old woman presented with alopecia for 7 years, which had worsened in the last few months. Her medical history included anxiety disorder. Physical examination showed frontal and fronto-temporal hairline recession with isolated hairs in the original temporal hairline, and pseudo-fringe sign in the frontal area. Clusters of short hairs with similar length were seen behind the hairline. [Figures 1a and b]. A completely alopecic cicatricial band was noted preceding this area. Eyebrow alopecia was observed.

- Right (a) and frontal (b) views, showing frontal and fronto-temporal hairline recession with isolated hairs in the original temporal hairline. Pseudo- fringe-sign was noted in the frontal area, along with hairs shorter than the normal ones

- Right (a) and frontal (b) views, showing frontal and fronto-temporal hairline recession with isolated hairs in the original temporal hairline. Pseudo-fringe-sign was noted in the frontal area, along with hairs shorter than the normal ones
Dermoscopy of the frontal area revealed black dots and short hairs with different length and sharply cut ends, in addition to loss of follicular openings, follicles with one hair shaft, follicular hyperkeratosis and white areas [Figure 2a]. Latter signs were also noted in the temporal area. Biopsy was performed in an area which suggested trichotemnomania to confirm this diagnosis [Figure 2b]. The diagnosis of FFA was made on the base of clinical findings. Treatment with oral finasteride along with topical minoxidil, and clobetasol was prescribed.
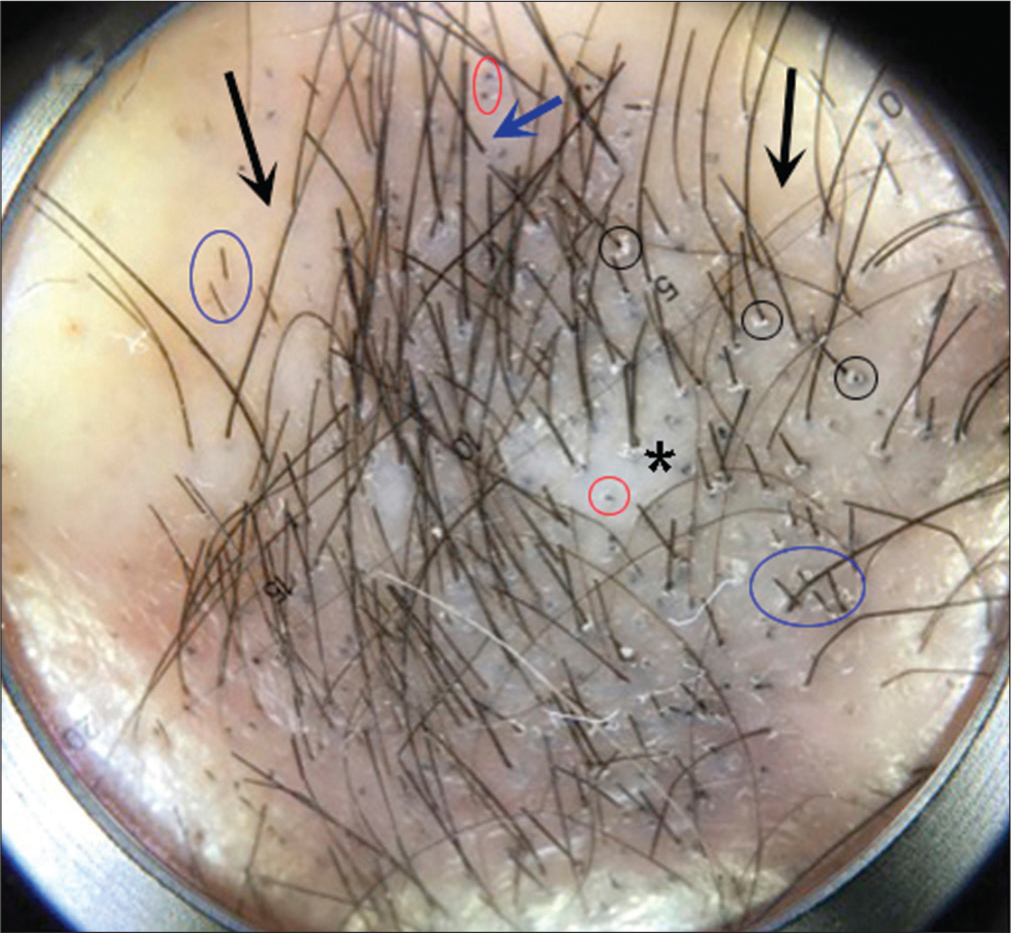
- Dermoscopy showed black dots (red circles) and short black hairs with sharp ends (blue circles), in addition to loss of follicular openings (black arrows), follicles with one hair shaft (blue arrow), follicular hyperkeratosis (black circles) and white areas (asterisk) (Photofinder, polarized light, ×100)
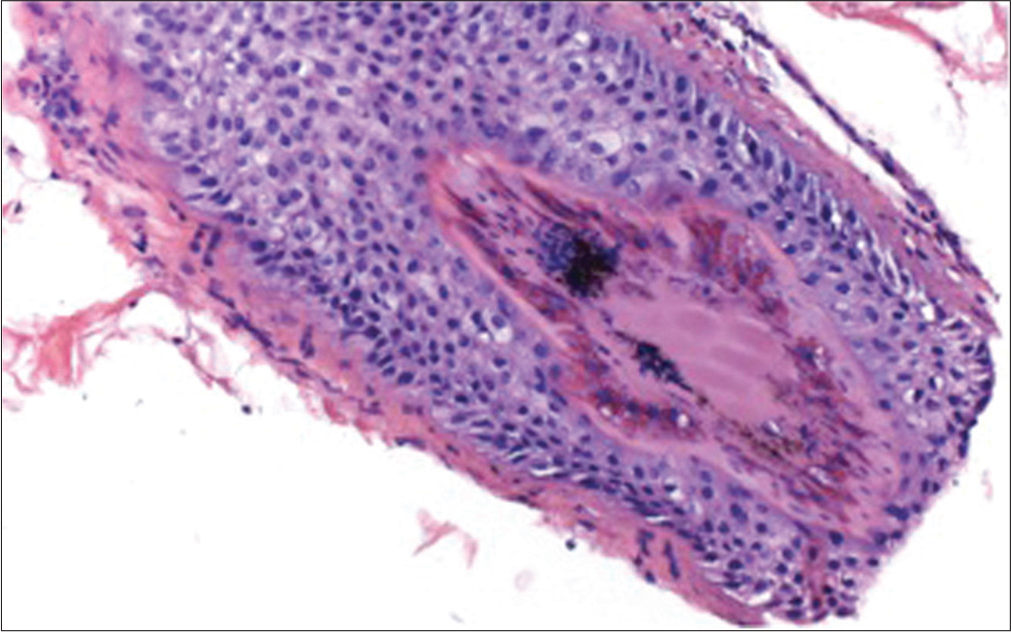
- Histopathological image (H and E, ×200) showing pigmented hair casts and absence of inflammatory infiltrate
Six months later, the hair in the frontal area had regrown [Figure 3a], but an oval area of decreased hair density was noted around the vertex [Figure 3b]. Dermoscopy demonstrated thin hairs with diversity in hair diameter, but again short black hairs with sharply cut ends were also seen[Figure 3c]. Early AGA aggravated by trichotemnomania was suspected. Oral N-acetyl-cysteine was added to the treatment.

- Recovering of the factious alopecia in the frontal area at 6 months. Note the persistence of the frontal recession because of the coexistence with frontal fibrosing alopecia
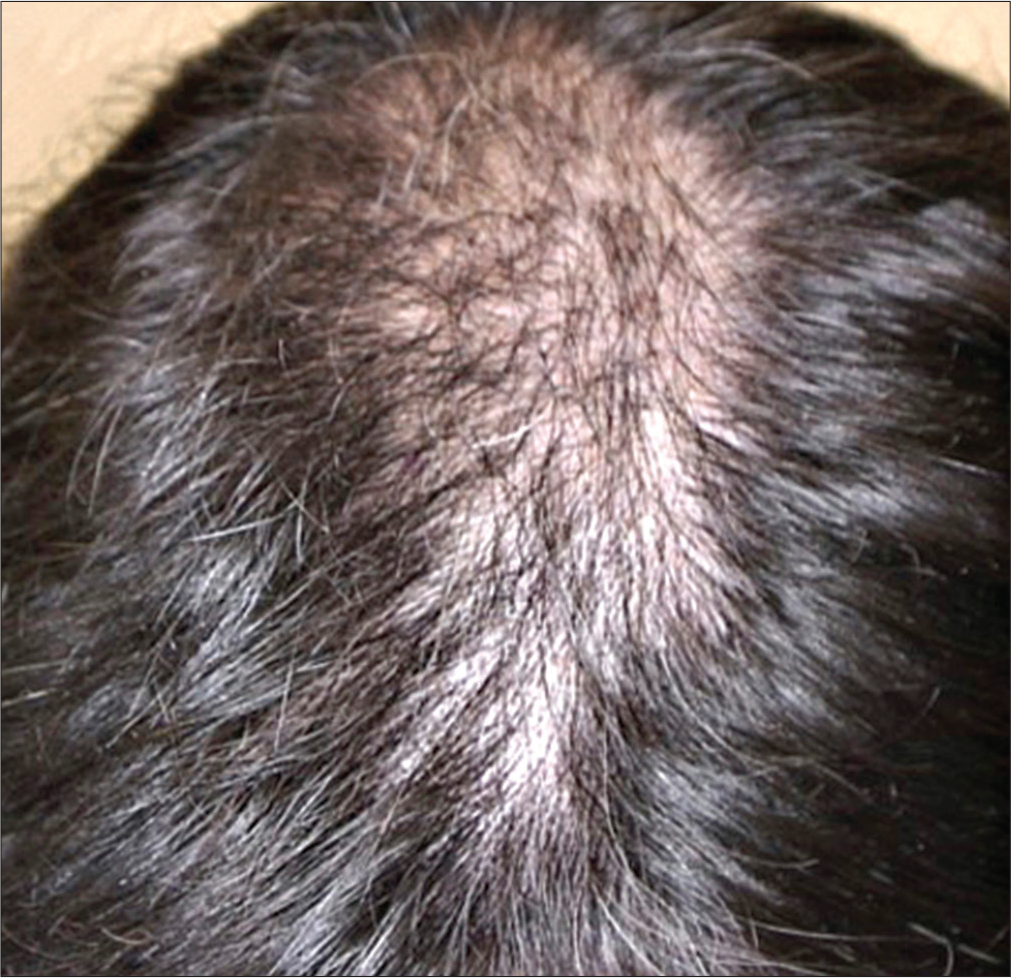
- Decreased hair density in the parieto-occipital region
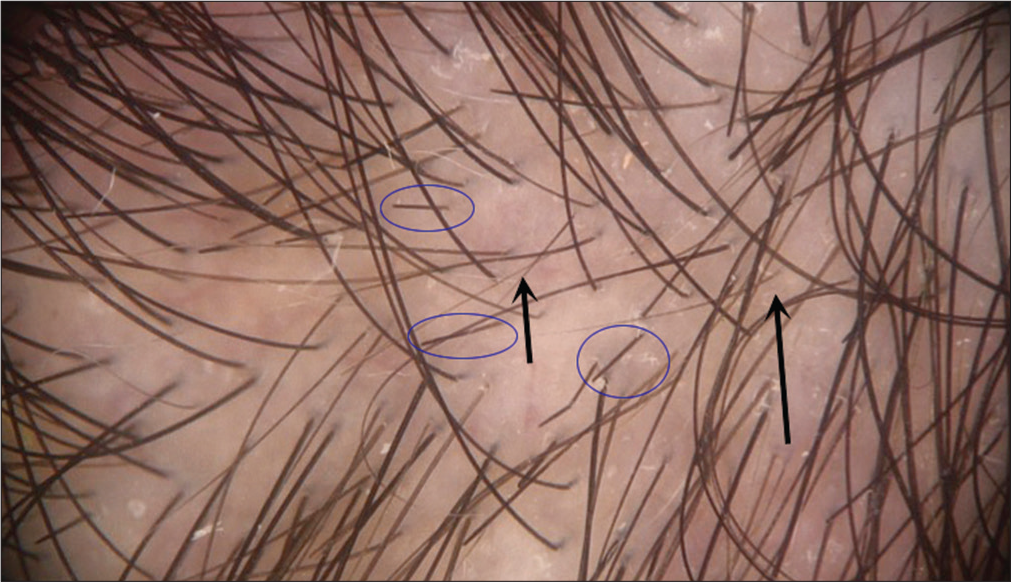
- Dermoscopy in parieto-occipital region showed thin hairs (arrows) with hair diameter diversity, but again short black hairs with sharply cut ends (blue circles) (Photofinder, polarized light, ×100)
Trichotemnomania is a self-induced alopecia, which belongs to the obsessive-compulsive disorders. The hair loss is due to self-cutting or shaving.3 It is not purely voluntary, but it is performed to relieve stress, although patients normally do not admit the habit.3 Trichotemnomania commonly involves scalp, although it may also affect eyebrows, eyelashes, and pubic and axillary hair. Clinically it is characterized by the presence of short hairs with the same length and sharply cut ends.3
Trichotillomania is the commonest factitious hair disorder, which consists of a compulsive habit of plucking hair. The term “trichoteiromania” is reserved for those with the habit of repeated rubbing causing hair loss. Finally, trichodaganomania is the compulsive habit of biting one’s own hair.
FFA has been reported occurring concurrently with several types of alopecia, but not yet with any of the self-induced alopecias. AGA has been noted in 30% of women with FFA.2
Trichoscopy is a fast, non-invasive technique, helpful in the diagnosis of hair diseases. FFA is characterized by loss of follicular openings, perifollicular erythema, and minor follicular hyperkeratosis, scarring white patches, and the presence of lonely hairs. Black dots and short black hairs with sharply cut ends were the key for the associated diagnosis in our patient. Black hairs are observed mainly in alopecia areata, dissecting cellulitis, tinea capitis, chemotherapy-induced alopecia and trichotillomania.4 Trichotillomania can sometimes be difficult to distinguish from alopecia areata at dermatoscopy, because it also shows broken hairs, black dots and yellow dots. However, the presence of exclamation mark hairs suggests alopecia areata; while coiled hairs point to trichotillomania. Trichoptilosis (“split ends”), irregular coiled hairs, flame hairs, V-sign, tulip hairs, hair powder, and upright re-growing hairs are also observed in trichotillomania.5
AGA is characterized by an increased proportion of vellus hair, diversity in hair shaft diameter, brownish perifollicular halo, follicular units with one hair shaft, and the presence of variable number of yellow dots. These findings are more pronounced in the frontal area compared to the occipital one.4 Unlike FFA, eyebrows are not involved in AGA; however, compulsive trichoses may affect them.
In our patient, trichoscopy was very helpful in making the diagnosis of FFA, trichotemnomania and emerging AGA. The presence of sharply cut short hairs pointed to the diagnosis of trichotemnomania rather than trichotillomania. Biopsy confirmed the diagnosis.
N-acetylcysteine has been used in dermatology in several conditions, including trichotillomania. The mechanism of action is thought to be the reduction of glutamate levels in the nucleus accumbens.
In conclusion, we herein report a a case with concomitant FFA, trichotemnomania and AGA. Trichoscopy may be a really useful tool in cases with atypical clinical presentation.
Acknowledgement
To Dr. Aneiros-Fernández for providing the histological image.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal the identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- It's not all traction: The pseudo 'fringe sign' in frontal fibrosing alopecia. Br J Dermatol. 2015;173:1336-8.
- [CrossRef] [PubMed] [Google Scholar]
- A Cross-sectional Study of Rosacea and Risk Factors in Women with Frontal Fibrosing Alopecia. Acta Derm Venereol. 2019;99:1099-104.
- [CrossRef] [PubMed] [Google Scholar]
- Trichotemnomania: Hair loss mediated by a compulsive habit not admitted by patients. Acta Derm Venereol. 2012;92:183-4.
- [CrossRef] [PubMed] [Google Scholar]
- New trichoscopy findings in trichotillomania: Flame hairs, V-sign, hook hairs, hair powder, tulip hairs. Acta Derm Venereol. 2014;94:303-6.
- [CrossRef] [PubMed] [Google Scholar]




