Translate this page into:
Familial dyskeratotic comedones
Correspondence Address:
M Sendhil Kumaran
Department of Dermatology, St. Johns Medical College Hospital, Bangalore
India
| How to cite this article: Kumaran M S, Appachu D, Jayaseelan E. Familial dyskeratotic comedones. Indian J Dermatol Venereol Leprol 2008;74:142-144 |
Abstract
Familial dyskeratotic comedones (FDC) is a rare autosomal dominant inherited condition, characterized by widespread, symmetrically scattered, comedone-like, hyperkeratotic papules, which are cosmetically unappealing. These lesions appear around puberty and show a predilection to involve the trunk, arms and face. The lesions are asymptomatic and gradually worsen with time. Histology shows invagination of the epidermis with a lamellar keratinous plug and focal evidence of dyskeratosis. This condition is generally refractory to therapy. We report here two cases with this rare disorder who had a strong familial history of the same disorder.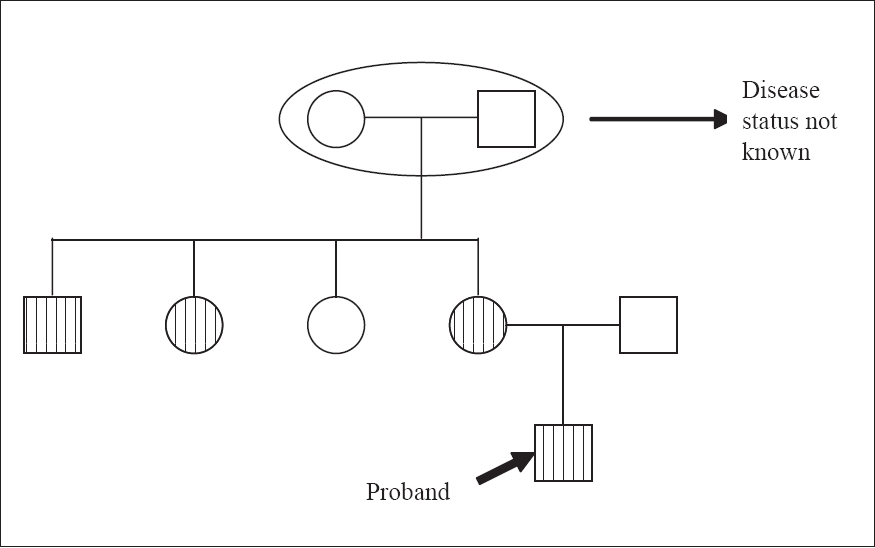 |
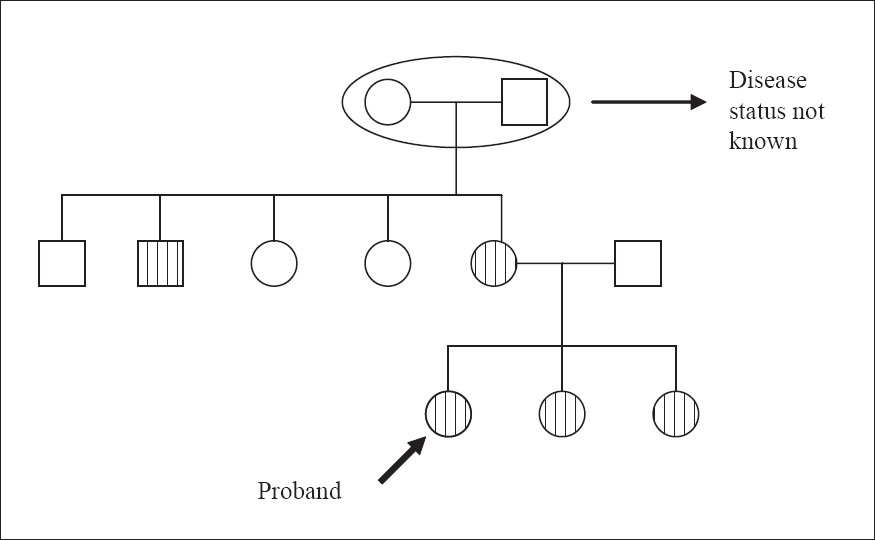
| Figure 5: Pedigree chart-Case 2 |
|
| Figure 5: Pedigree chart-Case 2 |
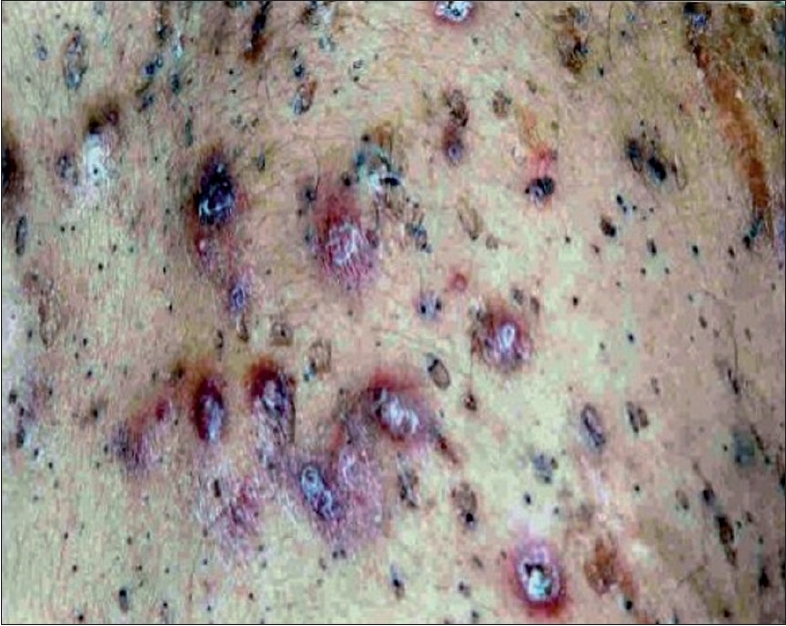 |
| Figure 4: Multiple inflamed nodules and comedones over back |
|
| Figure 4: Multiple inflamed nodules and comedones over back |
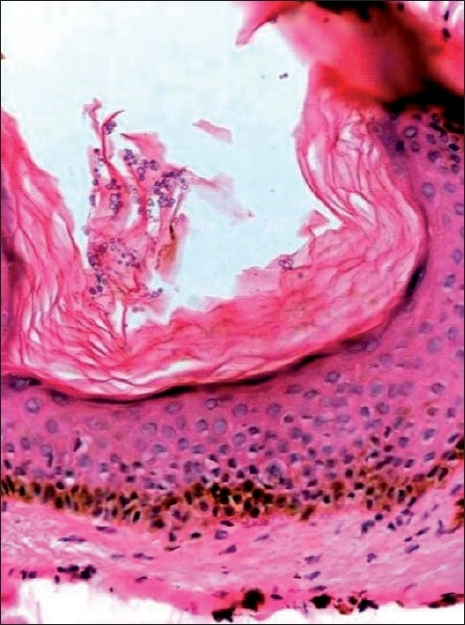 |
| Figure 3: Dilated follicular ostia filled with lamellar keratin with yeasts (H and E stain, 20�) |
|
| Figure 3: Dilated follicular ostia filled with lamellar keratin with yeasts (H and E stain, 20�) |
 |
| Figure 2: Pedigree chart-Case 1 |
|
| Figure 2: Pedigree chart-Case 1 |
 |
| Figure 1: Pock-like scars and comedones - case 1 |
|
| Figure 1: Pock-like scars and comedones - case 1 |
Introduction
Familial dyskeratotic comedones (FDC) is a rare asymptomatic autosomal dominant condition with distinctive clinical and histopathological features. Ever since its preliminary report by Rodin et al. [1] in 1967, only a few cases have been reported in literature around the world. It is clinically characterized by scattered, hyperkeratotic comedone-like papules. [2] Histopathology shows crater-like invaginations filled with keratinous material and evidence of dyskeratosis. [3] To the best of our knowledge, only 15 patients from seven families have been reported in literature [1],[2],[3],[4],[5],[6],[7],[8] and there is no case reported from India. We report here two families from India with this rare disorder.
Case Reports
Case 1
A 21 year-old female presented with an eight year-old history of multiple, asymptomatic widespread, hyperkeratotic papules. Her lesions initially appeared over the chest and subsequently spread to involve all areas of the body except the scalp, legs, mucosa, palms and soles. Apart from these skin lesions, multiple pock-like scars were seen over the face and the back. Removal of a keratinous plug from one of the papules revealed a minimal bleeding crater. There was no evidence of acne. The lesions started as pinpoint dark papules, which increased in number and extent of involvement as the patient grew older. When fully formed, the lesions measured around 0.5 to 1 cm in size [Figure - 1].
A few of the keratotic papules formed painful, inflamed swellings over the back. The patient had not received any treatment and was in good health and otherwise normal. A family history of similar lesions, that had started around the age of 12 years, was noted in her mother, two younger sisters and a maternal uncle [Figure - 2].
Skin biopsy from the hyperkeratotic lesions revealed a crater-like invagination filled with lamellar keratinous material [Figure - 3]. Foci of dyskeratosis were seen and a few of the dilated follicles showed colonization with budding yeast cells. Skin biopsies from the patient′s mother and sister revealed similar histopathological findings. The patient was treated with oral itraconazole 200 mg/day for one week resulting in a decrease in the number of keratotic papules and inflamed swellings.
Case 2
A 30 year-old male presented with hyperkeratotic papules (similar to case 1) over the trunk, upper limbs, face and thighs which initially appeared around 15 years of age over upper limbs and increased progressively since then. He also gave a history of tender swelling over the back [Figure - 4], which appeared when the keratotic papules increased in size. Case 2 had more lesions than did case 1. He also had large pock-like scars over his face. Physical examination aside from the skin lesions was normal. He had been treated with isotretinoin 20 mg daily for five months before he came to us with no improvement. Family history of similar lesions was seen in the mother, maternal uncle and aunt [Figure - 5]. Histopathology showed similar changes as those in case 1.
Discussion
Carneiro et al. [3] proposed the term FDC when he first described a family of four members affected with this rare entity, which was based on the following distinctive features:
- Lesions clinically resembling comedones
- Occurrence in some family members
- Presence of dyskeratotic changes on histological examination
McKusick [2] recently classified the disease as autosomal dominant (McK 120450). As the condition is asymptomatic, it may only be seen as an incidental finding. Complete family history (all family members) should be taken whenever possible.
The lesions usually appear around puberty and show a predilection for the trunk, arms, legs, face and shaft of the penis, sparing the glans, palms and soles. [2] Histologically, it is characterized by dyskeratosis and invaginations into the dermis, occasionally acantholysis may be seen. Dyskeratosis may not be seen in all patients. [9] Electron microscopy in FDC shows a decreased number of desmosomal attachments within the stratum malpighii. [5]
Both our index cases had clinical and histopathological features which correlated well with the diagnosis of FDC. However, there was one peculiar finding in both our patients; a few of the follicular ostia were filled with budding yeasts cells. It is not known how these yeasts were contributing to the pathogenesis of the disease. Culture or scrapping for the fungus was not attempted as it is well known that P. ovale colonizes in the pilosebaceous ducts. [10] Nearly half of the cases reported in literature had concomitant acne and only one was reported to have severe acne cysts. Both our patients gave history of multiple inflamed acne cysts over the back, most of which led to secondary scarring.
Kyrle′s disease, reactive perforating collagenosis, keratosis pilaris, perforating folliculitis, nevus comedonicus, acne vulgaris and Darier disease must be considered in the differential diagnosis. [1],[3],[6] Treatment has always been unrewarding. Various treatment modalities including topical retinoids and oral isotretinoin have proved to be ineffective. [7] The pathophysiological process in FDC could be different from that of normal comedones in acne, thus explaining its lack of response to retinoid treatment. However, frequent sun exposure [5] and carbon dioxide laser [5] have shown promising results. Our first patient has shown good results with itraconazole and has been on regular follow-up with us. We found that when the patient was put on itraconazole pulse therapy, a dramatic response in the form of healing of the inflamed lesions along with the absence of new lesions was noted. The exact mode of action of itraconazole remains unknown; it probably decreased the local yeast colonization.
FDC is usually asymptomatic, hence, it may go unseen. However, in patients where the face is also involved, it could lead to many social problems especially in the female population. Data regarding the long-term follow-up of these patients are lacking. The prognosis is generally better as the patients are otherwise healthy.
This report highlights both the efficacy of itraconazole and reports two cases of this rare genodermatosis, which to the best of our knowledge, is the first report from India.
| 1. |
Rodin HH, Blakenship ML, Bernstein G. Diffuse familial comedones. Arch Dermatol 1967;96:145-6.
[Google Scholar]
|
| 2. |
Van Geel NA, Kockaert M, Neumann HA. Familial dyskeratotic comedones. Br J Dermatol 1999;140:956-9.
[Google Scholar]
|
| 3. |
Carneiro SJ, Dickson JE, Knox JM. Familial dyskeratotic comedones. Arch Dermatol 1972;105:249-51.
[Google Scholar]
|
| 4. |
Cantu DJ, Gomez-Bustamente MO, Gonzalez-Mendoza A, Sαnchez-Corona J. Familial comedones. Arch Dermatol 1978; 114:1807-9.
[Google Scholar]
|
| 5. |
Hall JR, Holder W, Knox JM, Knox JM, Verani R. Familial dyskeratotic comedones. J Am Acad Derm 1987;17:808-14.
[Google Scholar]
|
| 6. |
Stander S, Rutten A, Metze D, Familial dyskeratotic comedones: A rare entity. Hautarzt 2001;52:533-6.
[Google Scholar]
|
| 7. |
Michot C, Guilhou JJ, Bessis D. Familial dyskeratotic comedones. Ann Dermatol Venerol 2004;131:811-3.
[Google Scholar]
|
| 8. |
Hallermann C, Bertsch HP. Two sisters with familial dyskeratotic comedones. Eur J Dermatol 2004;14:214-5.
[Google Scholar]
|
| 9. |
Griffiths WA, Judge MR, Leigh IM. Disorders of keratinization. In : Champion RH, Burton Jl. Burns DA, Breathnach SM, editors. Textbook of dermatology. Blackwell Science Publications: Chapter 34, 1998. p. 1483-8.
[Google Scholar]
|
| 10. |
Brasch J. In vitro susceptibility of pityrosporum ovale (Malassezia furfur) to human androgenic steroids. Mycopathologica 1993;123:99-104.
[Google Scholar]
|
Fulltext Views
7,006
PDF downloads
1,433





![[Figure - 1]](#fig_ijdvl_2008_74_2_142_39700_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2008_74_2_142_39700_2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2008_74_2_142_39700_3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2008_74_2_142_39700_4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2008_74_2_142_39700_5.jpg){kind=link}