Translate this page into:
EEC syndrome sans clefting: Variable clinical presentations in a family
Correspondence Address:
Sejal Thakkar
C-82, Smruti Society, Refinery Road, Gorwa, Vadodara - 390 016
India
| How to cite this article: Thakkar S, Marfatia Y. EEC syndrome sans clefting: Variable clinical presentations in a family. Indian J Dermatol Venereol Leprol 2007;73:46-48 |
Abstract
Ectrodactyly, ectodermal dysplasia and cleft palate/lip syndrome (EEC) is a rare autosomal dominant syndrome with varied presentation and is actually a multiple congenital anomaly syndrome leading to intra- and interfamilial differences in severity because of its variable expression and reduced penetrance. The cardinal features include ectrodactyly, sparse, wiry, hypopigmented hair, peg-shaped teeth with defective enamel and cleft palate/lip. A family comprising father, daughter and son presented to us with split hand-split foot deformity (ectrodactyly), epiphora, hair changes and deafness with variable involvement in each family member.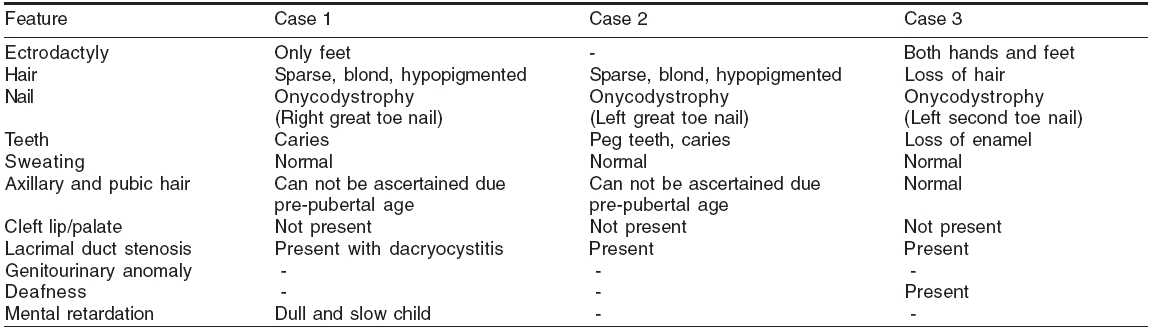
 |
| All family members showing feet involvement |
|
| All family members showing feet involvement |
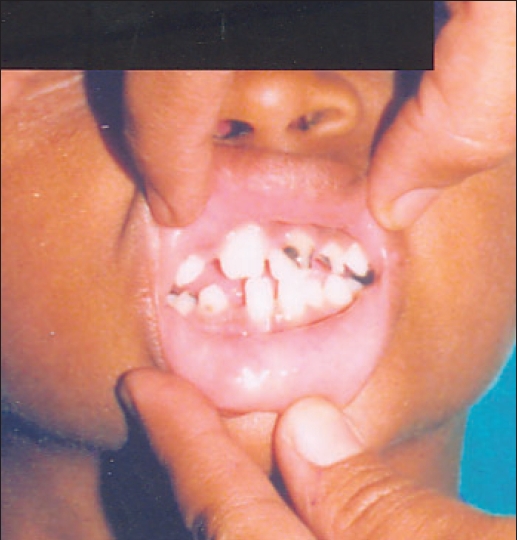 |
| Deciduous, peg teeth (Case 2) |
|
| Deciduous, peg teeth (Case 2) |
 |
| Sparse, blond, hypopigmented hair (Case 1) |
|
| Sparse, blond, hypopigmented hair (Case 1) |
 |
| Split feet deformity with normal hands (Case 1) |
|
| Split feet deformity with normal hands (Case 1) |
Introduction
The EEC syndrome, a rare form of multiple congenital anomaly syndrome,, was first described in 1936 by Cockayne[1] and later designated by Rudiger and colleagues as EEC syndrome.[2] The main clinical features are: ectrodactyly, sparse, wiry, hypopigmented hair, peg-shaped teeth with defective enamel and cleft palate/ lip. Besides these cardinal features, lacrimal duct abnormalities, urogenital anomalies, mental retardation and conductive deafness may be present. Paucity of reports of familial cases of EEC syndrome, especially in the Indian literature, prompted us to report these cases here.[3],[4] This report suggests autosomal dominant transmission in a family and highlights the intrafamilial variations indicating variable penetrance.
Case reports
Case 1
A 10-year-old girl, born of a nonconsanguineous marriage, with complaint of epiphora was referred by an ophthalmologist to the Department of Dermatology for hair changes. On enquiry she reported feet deformities. Her parents gave history of poor scholastic performance. There was no history of fused eyelid margin, scalp erosions, denudation of the skin or cleft lip /palate. Her brother (Case 2) and her father (Case 3) had a similar eye problem. Her father also had hand and feet deformities.
Physical examination revealed ectrodactyly of both the feet along with syndactyly i.e., split feet deformity with normal hands [Figure - 1]. She had sparse, hypopigmented, blond hair [Figure - 2] and onychodystrophy of the great toe nail. Axillary/ pubic hair involvement can not be confirmed as child was in prepubertal age, no ear deformities/ supernumerary nipples and had normal sweating. She did not have cleft lip/palate. On dental examination, no abnormalities except a few carious teeth were detected. Ophthalmic examination revealed lacrimal duct stenosis with dacryocystitis for which she was treated with antibiotics followed by dilatation of the duct.
On investigations, X-ray hands and feet confirmed the clinical findings. Her USG abdomen and pelvis were normal. Skin biopsy showed normal appendages. In view of these findings, the possibility of EEC syndrome was considered and other family members were evaluated.
Case 2
An eight-year-old male child, brother of the first case, was assessed in reference to Case 1. He had complaint of epiphora off and on. He had sparse, blond, hypopigmented hair and onycodystrophy in the great toe nail. He also had normal sweating.
He had no deformities of hands/feet or cleft lip/palate. On ophthalmological examination, he had lacrimal duct stenosis and dental check-up showed peg teeth with carious deciduous teeth [Figure - 3].
Case 3
A 39-year-old male, the father of the two previous cases, was assessed and found to have ectrodactyly of both the hands and feet since birth. He had history of hair loss since the age of 10 years. He also had complaints of epiphora and deafness. He did not have any sweating abnormality.
On examination, he had tetramelic ectrodactyly, hair loss and onychodystrophy of toe nail. He was found to have conduction deafness and lacrimal duct stenosis. Rinne test was negative and Weber test was centralized. He was advised audiometry but was not willing to go for the same. Dental examination showed peg teeth and enamel loss on incisor teeth. No findings suggestive of clefting of lip/palate were present [Table - 1].
Discussion
The EEC syndrome [OMIM: 129900] is a rare autosomal dominant disorder attributed to mutations in gene encoding for p63, a tumor suppressor protein, involving both the ectodermal and mesodermal tissues. The syndrome includes ectrodactyly (split hand/foot deformity), cleft lip/palate, hypotrichosis, hypodontia, dystrophic nails, eye duct anomalies and sometimes hypohidrosis.[5] Ectrodactyly is a major feature in which there is abnormal development of median rays of the hands and/or feet. Cleft palate with variable lip involvement occurs in 70-100% of cases.[6] Epiphora and recurrent infections with keratitis are commonly induced by nasolacrimal duct obstruction. Almost half of the patients have some degree of conduction deafness. Mental retardation is seen in 5-10% of cases. Genitourinary abnormalities are also common. According to Buss et al , the diagnosis of EEC syndrome should include ectodermal dysplasia of any variety and two of the following additional features: ectrodactyly, cleft lip/palate and lacrimal duct abnormalities.[7]
All the three cases reported here had findings of ectodermal dysplasia in the form of hair, nail and teeth involvement along with lacrimal duct abnormality. Two of them had ectrodactyly in which the father had tetramelic ectrodactyly while the daughter had only feet involvement [Figure - 4]. The index case had mild mental retardation and the father had conduction deafness. Surprisingly, none of them had findings of cleft lip/palate.
Similar to our case, a family was reported by Wallis et al . with ectrodactyly and ectodermal dysplasia (hypotrichosis and abnormal dentition) without cleft lip/palate. The existence of a separate syndrome of ectrodactyly, ectodermal dysplasia without clefting had not been described previously although Wallis has suggested that it represents a distinct clinical entity.[8]
This phenotypic variation in a family illustrates the variable penetrance of the gene. The complexity of this genotype-phenotype correlation in p63 syndromes is in part attributed to the complex biochemical structure of p63 because of its six isomers.[9] Genetic study to pinpoint the exact nature of the defect in our cases could not be done due to lack of facilities.
Early recognition of the EEC syndrome may lead to more effective interventions. Such patients often have ocular and auricular defects that progressively become more severe. The patient′s dental status requires frequent evaluation in order to prevent further damage. It is important to address the physical defect and functional problem as well as the psychological issues that may accompany this disorder.
| 1. |
Cockayne EA. Cleft palate-lip, hare lip, dacryocystitis and cleft hand and foot. Biometrika 1936;28:60-3
[Google Scholar]
|
| 2. |
Rudiger RA, Haase W, Passarge E. Association of ectrodactyly, ectodermal dysplasia and cleft lip-palate- the EEC syndrome. Am J Dis Child 1970;120:160-3.
[Google Scholar]
|
| 3. |
Kalla G, Anush G. Ectrodactyly. Indian J Dermatol Venereol Leprol 2002;68:152-3
[Google Scholar]
|
| 4. |
Cyriac MJ, Lashpa E. Lobster claw hand: A manifestation of EEC syndrome. Indian J Dermatol Venereol Leprol 2006;72:54-6
[Google Scholar]
|
| 5. |
Zlotogora J, Ogur G. Syndactyly, ectodermal dysplasia, and cleft lip and palate. J Med Genet 1988;25:503.
[Google Scholar]
|
| 6. |
Roelfsema NM, Cobben JM. The EEC Syndrome: A literature study. Clin Dysmorphol 1996;5:115-27.
[Google Scholar]
|
| 7. |
Buss PW, Hughes HE, Clarke A. Twenty four cases of the EEC syndrome: Clinical presentation and management. J Med Genet 1995;32:716-23.
[Google Scholar]
|
| 8. |
Wallis CE. Ectrodactyly (split hand/split foot) and ectodermal dysplasia with normal lip and palate in four generation kindred. Clin Genet 1988;34:252-7.
[Google Scholar]
|
| 9. |
Payne AS, Yan AC, Ilyas E, Li W, Seykora JT, Young TL, et al . Two novel TP63 mutations associated with the ankyloblepharon, ectodermal defects and cleft lip and palate syndrome: A skin fragility phenotype. Arch Dermatol 2005;141:1567-73.
[Google Scholar]
|
Fulltext Views
3,479
PDF downloads
1,960





![[Figure - 1]](#fig_ijdvl_2007_73_1_46_30653_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2007_73_1_46_30653_2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2007_73_1_46_30653_3.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2007_73_1_46_30653_5.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2007_73_1_46_30653_4.jpg){kind=link}