Translate this page into:
Disseminated cutaneous rhinosporidiomas in an immunocompetent male
Correspondence Address:
Sunil N Tolat
Aakar Bhavan, Above House of Laptops, Opposite IMA Hall, Hirabaug Chowk, Tilak Road, Shukrawar Peth, Pune - 411 002, Maharashatra
India
| How to cite this article: Tolat SN, Gokhale NR, Belgaumkar VA, Pradhan SN, Birud NR. Disseminated cutaneous rhinosporidiomas in an immunocompetent male. Indian J Dermatol Venereol Leprol 2007;73:343-345 |
Abstract
Rhinosporidiosis is a chronic recurrent infective granulomatous disease of man and animals. It is endemic in India and Sri Lanka. Rhinosporidiosis is a chronic disease commonly involving the nose and nasopharynx. Cutaneous lesions, although rare, can occur due to autoinoculation or due to hematogenous spread. However, disseminated cutaneous lesions presenting as tumor-like swellings are rare. We report here a 48-year-old immunocompetent patient who had disseminated painless cutaneous tumor-like swellings over both the upper limbs, abdomen, left buttock and calf since 10 months, gradually increasing in size. On inquiring, the patient gave history of excisions and electrocauterization of subglottic and nasal polyps. Histopathological examination of these lesions was suggestive of rhinosporidiosis. The general and systemic examinations of the patient did not reveal any abnormality.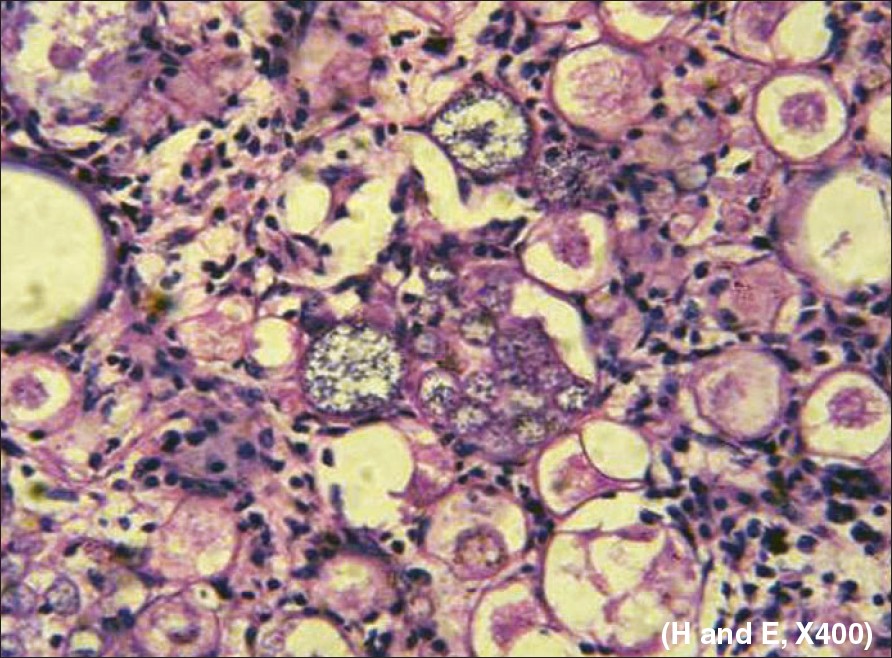 |
| Figure 4: Biopsy (low and high power) of the swelling over left lilac region revealed abundant rounded sporangia with a size of 50-200 � containing multiple endospores with a size of 6-10�. There were immature sporangia and mature ruptured sporangia with the release of endospores. |
|
| Figure 4: Biopsy (low and high power) of the swelling over left lilac region revealed abundant rounded sporangia with a size of 50-200 � containing multiple endospores with a size of 6-10�. There were immature sporangia and mature ruptured sporangia with the release of endospores. |
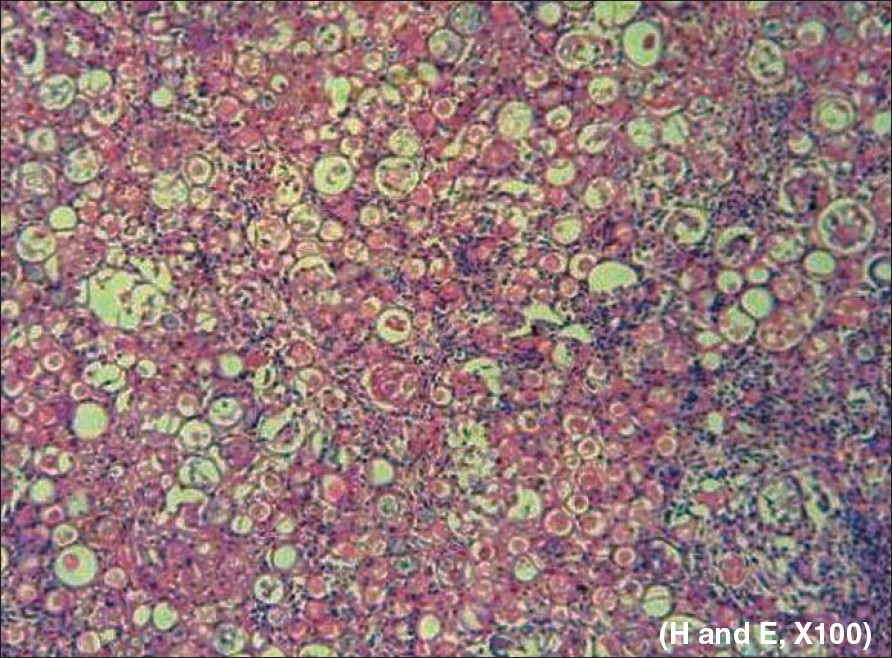 |
| Figure 3 : Biopsy (low and high power) of the swelling over left lilac region revealed abundant rounded sporangia with a size of 50-200 � containing multiple endospores with a size of 6-10�. There were immature sporangia and mature ruptured sporangia with the release of endospores. |
|
| Figure 3 : Biopsy (low and high power) of the swelling over left lilac region revealed abundant rounded sporangia with a size of 50-200 � containing multiple endospores with a size of 6-10�. There were immature sporangia and mature ruptured sporangia with the release of endospores. |
 |
| Figure 2: CT scan of left upper limb showed subcutaneous, benign, septate cystic masses that do not penetrate the underlying muscles or bones |
|
| Figure 2: CT scan of left upper limb showed subcutaneous, benign, septate cystic masses that do not penetrate the underlying muscles or bones |
 |
| Figure 1: Tense oblong swelling with dilated and engorged veins 15 x 8 cm over left elbow |
|
| Figure 1: Tense oblong swelling with dilated and engorged veins 15 x 8 cm over left elbow |
Introduction
Rhinosporidiosis is a chronic disease involving the nose and nasopharynx, clinically presenting as polyps. The involvement of skin adjacent to mucosal lesions is not uncommon. [1] However, disseminated cutaneous lesions presenting as tumor-like swellings is rare. We report here a case of disseminated cutaneous rhinosporidiosis in a 48-year-old immunocompetent patient.
Case Report
A 48-year-old male, laborer by occupation, presented with multiple swellings on both the upper limbs, abdomen, left buttock and calf since 10 months. Swellings were painless and gradually increasing in size. On inquiring, the patient gave history of repeated admissions in our hospital for the treatment of subglottic and nasal polyps with excisions and electrocauterization. Histopathological examination of these lesions was suggestive of rhinosporidiosis. The general and systemic examinations of the patient did not reveal any abnormality. Amongst various swellings, there was a 15cm x 8cm oblong swelling over the left elbow [Figure - 1]. The swelling was soft, cystic, nontender, noncompressible and tense with dilated and engorged veins visible over it. Similar swellings were also observed over the left calf, left infraclavicular region, left forearm and left iliac region. The differential diagnosis of angiolipomas and disseminated cutaneous rhinosporidiosis was considered. On investigation, hemogram was normal and enzyme-linked immunosorbent assay for human immunodeficiency virus was negative. Radiological investigations such as X-ray chest and ultrasonography abdomen were carried out; this did not reveal any abnormality. ENT examination showed subglottic masses on direct laryngoscopy. The CT scan of left upper limb showed subcutaneous, benign, septate cystic masses that did not penetrate the underlying muscle or bone [Figure - 2]. Smears were prepared of aspirated material from the swelling and stained by Papanicolaou and Giemsa stains; this showed numerous, large rounded structures and some of them contained endospores. An excisional biopsy of the swelling over the left lilac region revealed abundant, rounded sporangia of sizes of 50-200 µ containing multiple endospores of sizes of 6-10 µ. There were immature sporangia and mature ruptured sporangia with release of endospores. The stroma consisted of dense infiltration of polymorphs, lymphocytes, plasma cells and foreign body giant cells [Figure - 3],[Figure - 4]. Fungal culture was negative. Surgical excision of all the swellings was carried out. Bronchoscopic excision of subglottic masses was performed and dapsone was introduced in a dose of 100mg daily. After 2 months, swellings appeared over both upper limbs that gradually increased in size. We attempted to introduce intralesional amphotericin B in a dose of 25mg per swelling without success. Hence, both the swellings were excised and dapsone was continued in the same dose.
Discussion
Rhinosporidiosis is a chronic recurrent granulomatous disease of man and animals, caused by fungus Rhinosporidium Seeberi . It is endemic in India and Sri Lanka. The organism has not been cultured nor has it been successfully transmitted to experimental animals. Rhinosporidiosis was initially described by Seeber in 1900 and cutaneous Rhinosporidiosis was initially described by Forsyth. [1] Cutaneous lesions, although rare, can occur due to autoinoculation or due to hematogenous spread and are described to be of three types: [2] (1) Satellite lesions around the nasal polypoidal lesions. (2) Disseminated lesions with visceral involvement. (3) Primary cutaneous lesions without internal organ involvement.
Although primary cutaneous lesions appear to be uncommon, most authors have reported lesions that begin as tiny papules, which eventually developed into warty polypoidal growths. [3],[4] Poricha et al. , described a male patient of rhinosporidiosis with multiple, mobile, subcutaneous nodules that suppurated and burst with the drainage of mucopurulent content leading to ulceration. [5] Other authors have described similar presentations either in the presence [6] or absence of nasal involvement. [2] However, tumoral cutaneous rhinosporidiosis is extremely rare. Less than five such cases have been documented in the literature thus far. Date et al. , described large lesions on the right thigh in a patient from Orissa and subsequently proposed the term "rhinosporidioma". [7] A 44-year old male patient from Sri Lanka with large masses on thigh and anterior chest wall was described in the study by Angunwala et al. [8] In the abovementioned two patients, the clinical appearance had led to the diagnosis of chondrosarcoma and soft-tissue sarcoma with biopsy showing the typical picture of rhinosporidiosis. Our patient with multiple tumor-like swellings was a unique presentation of disseminated cutaneous rhinosporidiomas.
To the best of our knowledge, rhinosporidiosis remains a therapeutic challenge amenable only to surgical excision with a high risk of recurrence and occasional widespread and fatal complications. A number of previous studies using various drugs like dapsone, ketoconazole, ciprofloxacin and amphotericin B suggested encouraging results only with dapsone. Previous light and electron microscopic studies have confirmed maturation arrest of spores and accelerated granulomatous response with fibrosis following the dapsone therapy. [9] Surgical removal and electrodesiccation are the treatments of choice. [10] Our patient has undergone surgical excision of all the lesions and has been advised to take dapsone for one year. The present case is being reported to highlight this rare presentation of disseminated cutaneous rhinosporidiosis that can masquerade as soft-tissue tumors.
| 1. |
Padmavathy L, Rao IL, Sevam SS, Sahoo CG. Disseminated cutaneous rhinosporidiosis in a HIV seropositive patient. Indian J Dermatol Venerol Leprol 2001;67:332-3.
[Google Scholar]
|
| 2. |
Hadke NS, Ananthkrishnan N, Ratanakar C, Baruah MC. Primary cutaneous rhinosporidiosis. Indian J Dermatol Venerol Leprol 1990;56:61-3.
[Google Scholar]
|
| 3. |
Thappa DM, Venktesan S, Sirka CS, Jaisankar TJ, Gopalkrishnan, Ratnakar C. Disseminated cutaneous rhinosporidiosis. J Dermatol 1998;25:527-32.
[Google Scholar]
|
| 4. |
Ghorpade A, Ramanan C. Verrucoid cutaneous rhinosporidiosis. J Eur Acad Dermatol Venerol 1998;10:269-70.
[Google Scholar]
|
| 5. |
Porichha O, Pradhan SC, Agarwal MN. Cutaneous rhinosporidiosis in a patient of lepromatous leprosy: A case report. Indian J Lepr 1986;58:626-7.
[Google Scholar]
|
| 6. |
Mathur DR. Disseminated cutaneous rhinosporidiosis. Indian J Pathol Microbiol 1995;38:223.
[Google Scholar]
|
| 7. |
Date A, Ramkrishna B, Lee VN, Sundraraj GD. Tumoral rhinosporidiosis. Hiatopathology 1995;27:288-90.
[Google Scholar]
|
| 8. |
Anjunwala P, Teissera DA, Dissanaike AS. Rhinosporidiosis presenting with two soft tissue tumors followed by dissemination. Pathology 1999;31:57-8.
[Google Scholar]
|
| 9. |
Job A, Venkateswaran S, Mathan M, Krishnaswami H, Raman R. Medical therapy of rhinosporidiosis with dapsone. J Laryngol Otol 1993;107:809-12.
[Google Scholar]
|
| 10. |
Kumari R, Laxmisha C, Thappa DM. Disseminated cutaneous rhinosporidiosis. Dermatol Online J 2005;11:19.
[Google Scholar]
|
Fulltext Views
2,074
PDF downloads
2,742





![[Figure - 1]](#fig_ijdvl_2007_73_5_343_35738_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2007_73_5_343_35738_2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2007_73_5_343_35738_3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2007_73_5_343_35738_4.jpg){kind=link}