Translate this page into:
Unilateral angiokeratoma of fordyce
Correspondence Address:
Sushil Y Pande
Department of Dermatology, Seth GS Medical College and KEM Hospital, Parel, Mumbai - 400012
India
| How to cite this article: Pande SY, Kharkar V D, Mahajan S. Unilateral angiokeratoma of fordyce. Indian J Dermatol Venereol Leprol 2004;70:377-379 |
 |
|
 |
|
Sir,
Angiokeratoma of Fordyce is a localized form of angiokeratoma affecting the scrotum and is probably the commonest of the angiokeratomas. We report a rare case of angiokeratoma of Fordyce with unilateral occurrence without any underlying disorder. Such a case has been reported only once in the literature recently, in association with a unilateral varicocele.[1]
A 32 year old male rickshaw driver presented with multiple asymptomatic reddish purple colored raised lesions on the left side of the scrotum since 2 years with progressive increase in number. There was no history of bleeding from the site or history of swelling on the left side of the scrotum.
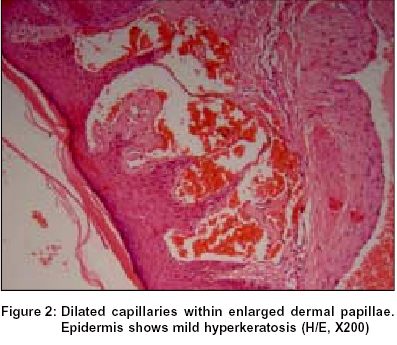
On examination, he had multiple, discrete, soft, smooth surfaced purplish red papules present unilaterally on anterolateral aspect of left side of the scrotum [Figure - 1]. Palpation ruled out varicocele, epididymal mass or inguinal hernia. Skin biopsy from a purplish papule showed mild hyperkeratosis with large, numerous, dilated and congested capillaries in an expanded papillary dermis [Figure - 2]. USG abdomen, pelvis and scrotum were done to rule out any vascular anomaly. On the basis of clinical features and histopathology, the patient was diagnosed as angiokeratoma of Fordyce with unilateral presentation as an unusual finding. We treated this patient with radiofrequency cauterization.
Scrotal angiokeratomas were first described by John Addison Fordyce in 1896.[2] Angiokeratomas are typically asymptomatic, 2 to 5 mm, blue-to-red papules with slightly keratotic surface. Commonest site is the scrotum with occasional affection of the shaft and glans of penis, and rarely leg, crural area and bulbar conjunctiva.[3],[5] Histopathologically the lesions show one or more dilated subepidermal blood vessels within a widened dermal papilla. The epidermal changes in all forms of angiokeratoma are secondary to friction. The principle morbidity comes from bleeding, anxiety, and sometimes over-treatment due to misdiagnosis. Usually, they do not require treatment. If treatment is needed, laser, electrocoagulation, excision, or cryotherapy may be used.
Exact pathophysiology of angiokeratomas remains unknown, although it has been proposed that increased venous pressure may contribute to their formation.[4] There are many reports of angiokeratomas occurring in the presence of a varicocele or other conditions of increased venous pressure (e.g. hernias, epididymal tumors, urinary tract tumors).[5] On the other hand, in the majority of cases, no cause for increased venous pressure was found.[6] However, it is possible that in these cases, the increase in venous pressure may be so mild as to be undetectable by the ordinary methods leading only to capillary dilatation at a site that has probably the lowest tissue pressure.
In our case, examination and investigations ruled out any overt cause for increased venous pressure on the affected side. However, a small or microscopic vascular malformation may have led to unilateral but subclinical increase in venous pressure, thereby resulting in the ectasia.
| 1. |
Bechara FG, Altmeyer P, Jansen T. Unilateral angiokeratoma scroti: A rare manifestation of a vascular tumor. J Dermatol 2004;31:39-41.
[Google Scholar]
|
| 2. |
Fitzpatrick JE, Gentry RH. Nonvenereal diseases of the male genitals. In: Moschella SL, Hurley HJ, editors. Dermatology. 3rd Ed. Philadelphia: WB Saunders; 1992. p. 1008-15.
[Google Scholar]
|
| 3. |
Sutton RL. A clinical and histopathological study of angiokeratoma of the scrotum. JAMA 1911;57:189-92.
[Google Scholar]
|
| 4. |
Bisceglia M, Carosi I, Castelvetere M, Murgo R. Multiple Fordyce-type angiokeratomas of the scrotum. An iatrogenic case. Pathologica 1998;90:46-50.
[Google Scholar]
|
| 5. |
Robinson SS, Tasker S. Angioma of the scrotum. Arch Dermatol 1946;54:667-74.
[Google Scholar]
|
| 6. |
Orvieto R, Alcalay J, Leibovitz I, Nehama H. Lack of association between varicocele and angiokeratoma of the scrotum (Fordyce). Mil Med 1994;159:523-4.
[Google Scholar]
|
Fulltext Views
2,998
PDF downloads
1,587





![[Figure - 1]](#fig_ijdvl_2004_70_6_377_13487_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2004_70_6_377_13487_2.jpg){kind=link}