
Translate this page into:
Slowly progressive nodular growth of the nail bed in a young adult
Corresponding author: Dr. Neetu Bhari, Department of Dermatology and Venereology, All India Institute of Medical Sciences, New Delhi, India. drntbhari@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Pangti R, Mehta N, Gupta S, Das P, Bhari N. Slowly progressive nodular growth of the nail bed in a young adult. Indian J Dermatol Venereol Leprol 2022;88:372-5.
A 34-year-old man, a known case of chronic myeloid leukemia on imatinib since four years, presented with a single, mildly painful, slowly progressive, pinkish swelling of the right thumb nail since one and a half years. There was no history of preceding local trauma.
Cutaneous examination revealed a pinkish, nodular, mildly tender swelling arising from the underlying nail bed, covering approximately the medial one-third of the right thumb nail [Figure 1].

- A pinkish nodular swelling covering approximately medial one-third of the right thumb
Dermoscopy showed a pinkish-white homogenous patch with well-defined margins along with peripheral radiating whitish streaks. Curved and branching vessels were seen in the center and in between the white streaks [Figure 2]. Ultrasonography of the nail revealed a hypo-echoic lesion of size 12.7 mm × 11.4 mm, not extending beyond the nail fold. After avulsion of the medial half of the nail plate, a flesh-colored nodule of size 1.3 cm × 1 cm with a smooth surface and gelatinous-to-firm consistency, was excised [Figure 3].
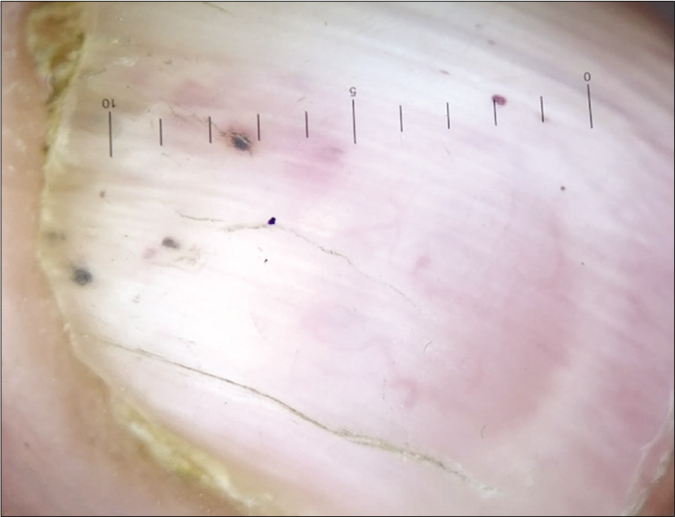
- Dermoscopy of the lesions showing a pinkish white homogenous patch with defined margins in the center along with peripheral radiating whitish streaks; the curved and branching vessels are seen in the center as well as between the radiating white streaks. (DermLite DL4, polarizing, 10×)
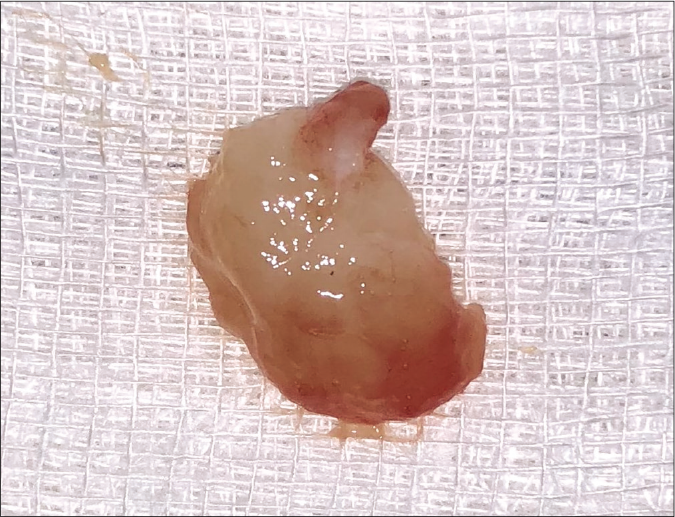
- An excised flesh colored to yellowish nodule of size 1.3 cm × 1 cm with smooth surface
Histopathology showed a relatively circumscribed, moderately cellular, spindle cell tumor with haphazardly arranged tumor cells and interspersed collagen fibers in a myxoid background [Figures 4 and 5]. Many thin-walled blood vessels were identified. Atypical mitoses or pleomorphic changes were not seen.The tumoral cells showed patchy, moderately intense immunostaining for CD 34, while negative for smooth muscle actin [Figure 6].
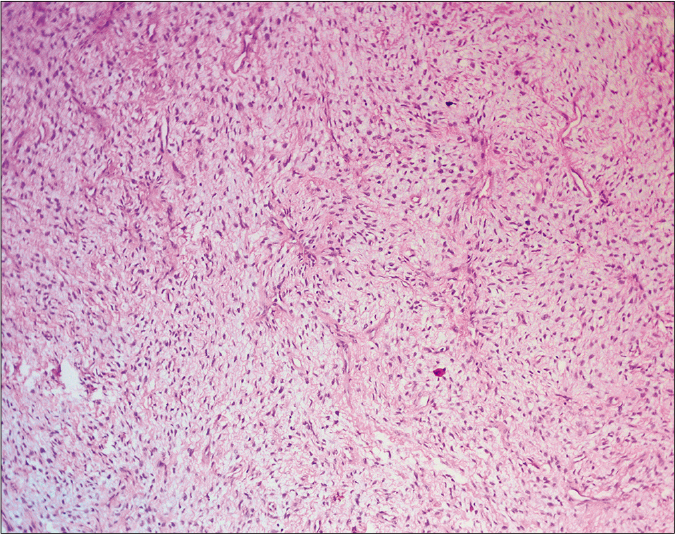
- A moderately cellular spindle cell tumor with myxoid stroma (H and E, 40×)
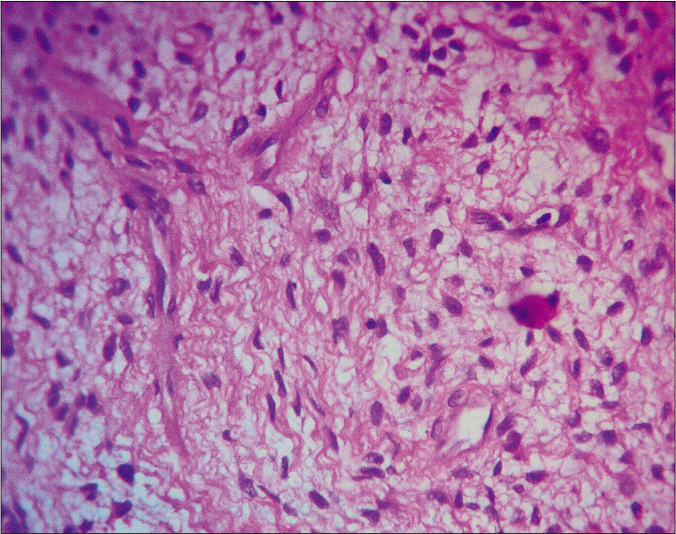
- Higher magnification showing spindle cells in myxoid stroma (H and E, ×400)
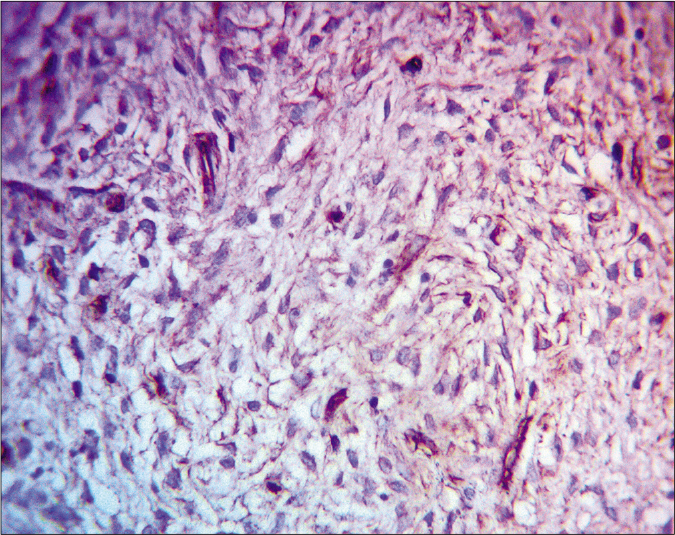
- Tumor cells positive for CD34 (IHC, ×400)
Question
What is your diagnosis?
Answer
Superficial acral fibromyxoma
Superficial acral fibromyxoma, also known as digital fibromyxoma, is a relatively uncommon tumor. It was first described in 2001.1 It has a distinct predilection for periungual or subungual and acral areas. It is more common in middle-aged males and affects hands and feet almost equally, mostly digits, near the nails. It presents as a slow-growing lesion. Bone involvement, in the form of erosions or lytic lesions, is rarely seen. Pain has previously been reported in 41% of the cases.2
On dermoscopic examination, an acral fibromyxoma over the palm/sole shows either a yellowish hyperkeratotic area with or without finger-like projections or a white scar-like patch with shiny white streaks/striae.The vascular pattern has been variably described as small arborizing vessels with an in-focus central telengiectasia, small blood vessels perpendicular to the surface or grouped polymorphous (fine curved and dotted) vessels at the periphery of the finger-like projections.3 A single case describing dermoscopy of a subungual fibromyxoma showed yellow-brown discoloration and partial nail plate destruction, characteristic of a fungal infection, while the nodular nail bed lesion showed structureless homogeneous red areas, a non-specific feature which can be seen in vascular lesions, amelanotic melanoma or squamous lesions of the nail. No discernible vascular pattern was apparent on dermoscopy.4 Dermoscopic analysis in our case showed a central well-defined whitish patch similar to that reported earlier in the palm/sole acral fibromyxoma, in addition to the prominent vascular findings. On ultrasonography, subungual tumors present as hypoechoic, homogenous, or heterogenous masses.4 Imaging studies can aid in evaluating bone involvement and the accurate tumor size of subungual acral fibromyxoma which is difficult to ascertain clinically.
On histological examination, the tumor comprises of spindle cells arranged in random, loose storiform or fascicular pattern. The stroma is either predominantly myxoid, myxo-collagenous or predominantly collagenous. Mitoses and atypia are rarely seen. Increased vascularity is seen in most cases. Tumor is strongly immunoreactive for CD34, CD99 and nestin, while variable positivity is seen for smooth muscle actin, CD10 and epithelial membrane antigen. Tumor is negative for Factor XIIIa, MUC4 and S-100.1,5,6 Differential diagnoses for superficial acral fibromyxoma include a long list of various benign and malignant lesions, based on the location of the lesion, similar histology of myxoid stroma and immunohistochemistry showing CD34 positivity.2,7-14 Benign tumors such as digital fibrokeratoma (acquired digital fibrokeratoma and periungual/ subungual fibroma), myxoid neurofibroma, superficial angiomyxoma, spindle cell lipoma, benign nerve sheath tumors including sclerosing perineuroma and nerve sheath myxoma, myxoid dermatofibroma, cellular myxoma of soft tissue, glomus tumor, tendon sheath fibroma, tenosynovial giant cell tumor and malignant tumors such as low-grade fibromyxoid sarcoma, myxoid dermatofibrosarcoma protuberans, myxofibrosarcoma, acral myxoinflammatory fibroblastic sarcoma and minute synovial sarcoma of digits, among others are close differentials. These should be differentiated from SAF with the help of histopathology and immunohistochemistry. Although the list is broad, a few of the most relevant differential considerations requiring distinction are discussed in Table 1. Molecular studies have shown Rb1 gene deletions, variably associated with loss of the corresponding 13q12 signal (monosomy at the 13q region).15
| Disease | Clinical features | Histopathology | Immuno-histochemistry |
|---|---|---|---|
| Superficial acral fibromyxoma | Solitary, slow growing lesion, mostly on periungual/subungual and acral areas | Myxoid, myxo-collagenous or predominantly collagenous stroma with spindle cells arranged in random, loose storiform or fascicular pattern | CD34+, CD99+nestin+, SMA+/-, CD10+/-, EMA+/-, Factor XIIIa-ve, MUC4-ve, S100-ve |
| Acquired digital fibrokeratoma7 | Solitary skin-colored papule with a characteristic hyperkeratotic collarette, commonly over fingers/toes, often in middle-aged adults | Marked hyperkeratotic and acanthotic epidermis with thick bundles of collagen which are vertically oriented, in dermis | Factor XIIIA+, CD34-ve |
| Glomus tumor8 | Solitary blue-red nodules associated with paroxysmal pain elicited by changes in temperature (usually cold) or pressure, involving fingers and toes in middle-aged adults. Subungual glomus tumors have been associated with neurofibromatosis type I | Well circumscribed tumor composed of sheets of uniform cells with pale or eosinophilic cytoplasm, well-defined cell margins and round or ovoid punched-out central nuclei and small blood vessels uniformly distributed | SMA+, CD34-ve |
| Superficial angiomyxoma9 | Solitary or as multiple papules, nodules or polypoid lesions associated with Carney complex, more common in men with a predilection for head, neck and trunk | Multilobulated, poorly circumscribed, myxoid stroma with scattered bland stellate and spindled cells in dermis and subcutis. Many blood vessels, frequent neutrophils | CD34+, S100 -ve, SMA-ve, pan keratin -ve |
| Myxoid neurofibroma10 | Solitary, nontender nodule in young adults commonly over face, shoulders, arms, feet, periungual regions | Well-circumscribed, characterized by spindle-shaped cells with wavy nuclei and abundant myxoid stroma | S100+, CD34 -ve |
| Low-grade fibromxyoid sarcoma11 | Slow-growing mass in deep soft tissue in young adults commonly over thighs, shoulders, inguinal area and chest wall | Bland spindled cells in a whorled growth pattern with alternating myxoid and fibrous stroma | MUC4+, vimentin+, CD34 -ve, cytokeratin -ve, smooth muscle actin -ve, S-100 -ve, neuron specific enolase -ve |
| Myxofibrosarcoma12 | Slow-growing, painless nodule or mass, commonly over extremities in the elderly | Multinodular tumor comprising of pleomorphic spindle cells in myxoid matrix. Curvilinear vessels with surrounding condensed cells characteristic | CD34+, vimentin+, actin+/-, EMA-ve, CD68 -ve, factor XIIIa -ve |
| Myxoid dermatofibrosarcoma protruberans2,13 | Pink or flesh-colored plaque that slowly enlarges to a nodule, predominantly on the trunk and proximal extremities of young to middle-aged adults | Prominent myxoid stromal changes and a multinodular growth pattern of spindled and stellated tumor cells containing slightly enlarged nuclei and numerous blood vessels | CD34+, EMA+/-, factor XIIIa -ve, CD99–ve, CD31 –ve, S100 –ve |
| Acral myxoinflammatory fibroblastic sarcoma14 | Slow growing, painless mass in the distal extremities of middle-aged patients | Multinodular with alternating densely cellular and myxoid hypocellular areas, mixed inflammatory infiltrate and bizarre giant and lipoblast-like cells | Vimentin+, CD34+/–, CD68+/–, SMA+/–, cytokeratin +/–, epithelial membrane antigen –ve, S100 –ve, desmin –ve, CD15 –ve, HMB45 –ve, CD45–ve |
Treatment of superficial acral fibromyxoma is complete surgical excision. However, recurrence is seen in 20%–25% of the cases.1 Complete excision is essential to prevent recurrence. Malignant transformation has not yet been reported.1,2 Although dermoscopy and imaging are helpful tools in the assessment of subungual superficial acral fibromyxoma, specific features are lacking. The diagnosis of and its distinction from other subungual tumors rely on histopathology and immunohistochemistry.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Digital fibromyxoma (superficial acral fibromyxoma): A detailed characterization of 124 cases. Am J Surg Pathol. 2012;36:789-98.
- [CrossRef] [PubMed] [Google Scholar]
- Superficial acral fibromyxoma. Int J Dermatol. 2015;54:499-508.
- [CrossRef] [PubMed] [Google Scholar]
- Superficial acral fibromyxoma in the heel with new vascular features on dermoscopy. J Cutan Pathol. 2018;45:416-8.
- [CrossRef] [PubMed] [Google Scholar]
- Clinico-pathologic, dermoscopic and ultrasound examination of a rare acral tumour involving the nail-case report and review of the literature. Clujul Med. 2016;89:160-4.
- [CrossRef] [PubMed] [Google Scholar]
- Superficial acral fibromyxoma: A clinicopathologic and immunohistochemical analysis of 37 cases of a distinctive soft tissue tumor with a predilection for the fingers and toes. Hum Pathol. 2001;32:704-14.
- [CrossRef] [PubMed] [Google Scholar]
- Superficial acral fibromyxoma: Report of 13 cases with new immunohistochemical findings. Am J Dermatopathol. 2017;39:14-22.
- [CrossRef] [PubMed] [Google Scholar]
- Acquired digital fibrokeratoma In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2019. Available from: https://www.ncbi.nlm.nih.gov/books/NBK545146/ [Last accessed on 2020 May 27]
- [Google Scholar]
- Vascular tumors: Tumors and tumor-like conditions of blood vessels and lymphatics In: Elder DE, ed. Lever's Histopathology of the Skin (10th ed). Philadelphia: Wolters Kluwer/Lippincott Williams & Williams; 2010. p. :1005-56.
- [Google Scholar]
- Superficial angiomyxoma: clinicopathologic analysis of a series of distinctive but poorly recognized cutaneous tumors with tendency for recurrence. Am J Surg Pathol. 1999;23:910-7.
- [CrossRef] [PubMed] [Google Scholar]
- Myxoid neurofibroma: an unusual presentation. Indian J Dermatol. 2008;53:35-6.
- [CrossRef] [PubMed] [Google Scholar]
- Low grade fibromyxoid sarcoma in thigh. Clin Orthop Surg. 2009;1:240-3.
- [CrossRef] [PubMed] [Google Scholar]
- Myxofibrosarcoma: A diagnostic pitfall. Rare Tumors. 2013;5:60-1.
- [CrossRef] [PubMed] [Google Scholar]
- Myxoid dermatofibrosarcoma protuberans: Clinicopathologic, immunohistochemical, and molecular analysis of eight cases. Am J Dermatopathol. 2007;29:443-8.
- [CrossRef] [PubMed] [Google Scholar]
- Acral myxoinflammatory fibroblastic sarcoma. Orthop Traumatol Surg Res. 2010;96:597-9.
- [CrossRef] [PubMed] [Google Scholar]
- Superficial acral fibromyxoma: Clinicopathological, immunohistochemical, and molecular study of 11 cases highlighting frequent Rb1 loss/deletions. Hum Pathol. 2017;60:192-8.
- [CrossRef] [PubMed] [Google Scholar]




