
Translate this page into:
Dermoscopic features of basal cell carcinoma in skin of color: A retrospective cross-sectional study from Puducherry, South India
Corresponding author: Dr. Rashmi Kumari, Department of Dermatology, Venereology and Leprology, JIPMER, Puducherry - 605 006, India. rashmi.sreerag@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Behera B, Kumari R, Thappa DM, Gochhait D, Srinivas BH, Ayyanar P. Dermoscopic features of basal cell carcinoma in dark skin phototype: A retrospective cross-sectional study from South India. Indian J Dermatol Venereol Leprol 2023;89:254-60.
Abstract
Background:
Dermoscopy is useful in the diagnosis of basal cell carcinoma (BCC). However, most descriptions of the dermoscopic features of BCCs are in Caucasians (skin types I-III) and there is a paucity of data in dark-skinned Indian patients.
Aims:
The aim of this study was to describe the various dermoscopic features of BCC in dark-skinned patients from South India and correlate these with the histopathologic subtypes.
Methods:
A retrospective observational study of biopsy-proven cases of BCC was conducted at a tertiary care center in South India using nonpolarized contact dermoscopy.
Results:
Sixty BCCs in 35 patients predominantly of skin phototypes IV or V were studied. These included 32 nodular, 27 superficial and 1 infiltrative type of BCC. The most common dermoscopic features noted were maple leaf-like areas (61.7%), blue-white veils (53.4%), ulceration (48.4%) and short fine telangiectases (46.7%). Ulceration, blue-white veils and arborizing vessels were significantly associated with nodular BCCs, while maple leaf-like areas, red-white structureless areas, multiple small erosions and spoke wheel areas were noted with superficial BCCs.
Limitations:
The limitations of this study include its retrospective nature, the use of only nonpolarized light for examination, the lack of other histopathological variants of BCC as well as the lack of a comparison group.
Conclusion:
We report a dermoscopic study of BCC in dark-skinned patients from Puducherry, South India. The blue-white veil was observed in half of the patients and was significantly associated with nodular BCCs. The addition of the blue-white veil to the diagnostic criteria for pigmented BCC could improve the diagnostic accuracy of dermoscopy in Indian patients.
Keywords
Basal cell carcinoma
blue-white veil
dark skin
dermoscopy

Introduction
BCCs are slow-growing, locally infiltrative epithelial tumors that rarely metastasize. The incidence of BCCs in the Indian population is low.1 Of the various morphological subtypes of BCC, the pigmented variety is most commonly seen in Indians.1,2 There is a paucity of dermoscopic studies of BCCs in the Indian skin. We thus aimed to delineate the various dermoscopic features of BCCs and to correlate these with the histopathologic subtypes of BCCs.
Methods
This retrospective observational study was conducted from January 2014 to December 2017 at the Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, a tertiary care hospital in South India. The study was approved by the institutional ethics committee.
All biopsy-proven cases of BCC of both genders and all age groups were included in the study. The patients were predominantly of skin phototypes IV and V. Patients with equivocal histopathological reports, xeroderma pigmentosum with multiple cutaneous tumors and collision tumors with BCC were excluded from the study. All images were taken in the nonpolarized contact mode (HEINE DELTA20® Dermatoscope, ×10) using liquid paraffin as immersion fluid. The gender, age, duration, size, location and diameter of the lesions were recorded in all patients.
Clinical photographs were used to classify the lesions as pigmented or nonpigmented. The BCCs were categorized as nodular, superficial, morpheaform or infiltrative based on the histologic features. In each lesion, classic and non-classic BCC-associated dermoscopic features were analyzed. The classic BCC-associated dermoscopic features included ulceration, maple leaf-like areas, blue-gray ovoid nests, blue-gray globules, arborizing vessels and spoke wheel areas, while the nonclassic features noted were short fine telangiectases, multiple small erosions, concentric structure, red-white homogenous areas and in-focus dots.3-5 Nonspecific dermoscopic features and other vascular structures were also recorded. For each dermoscopic feature, a histopathological analysis was performed for dermoscopic/dermatopathologic correlation.
Statistical Analysis
Dermoscopic features distributed between nodular and superficial BCCs were expressed as proportions. A Chi-square test was used to study the association of dermoscopic features between nodular and superficial BCCs. Fisher’s exact test was used when the variable’s expected value was less than 5. A P-value of <0.05 was considered significant. The data were analyzed using SPSS 20 software (IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.).
Results
Sixty BCCs in 35 patients satisfied the inclusion and exclusion criteria. The patients were from 24 to 80 years of age, and included 19 females and 16 males. The majority (57/60) of BCCs were pigmented and only three were non-pigmented. Nodular and superficial BCC constituted 32 and 27 lesions respectively and there was a single infiltrative BCC.
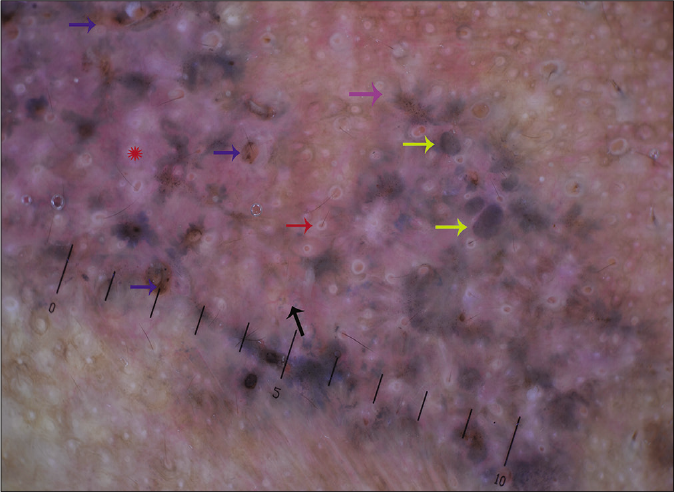
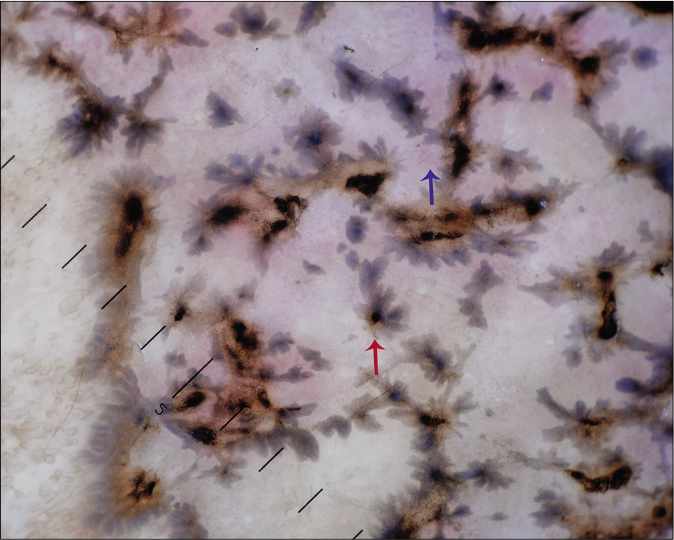
The most common dermoscopic features noted were maple leaf-like areas [61.7%, Figure 1], blue-white veils [53.4%, Figure 2], ulcerations (48.4%) and short fine telangiectases (46.7%). The color of the maple leaf-like areas, large ovoid nests [Figures 3 and 4], aggregates [Figure 5] and globules varied from brown, brown-gray to blue-gray.6 The dermoscopic features are detailed in Table 1. The association of various dermoscopic features with nodular and superficial BCC is shown in Table 2.
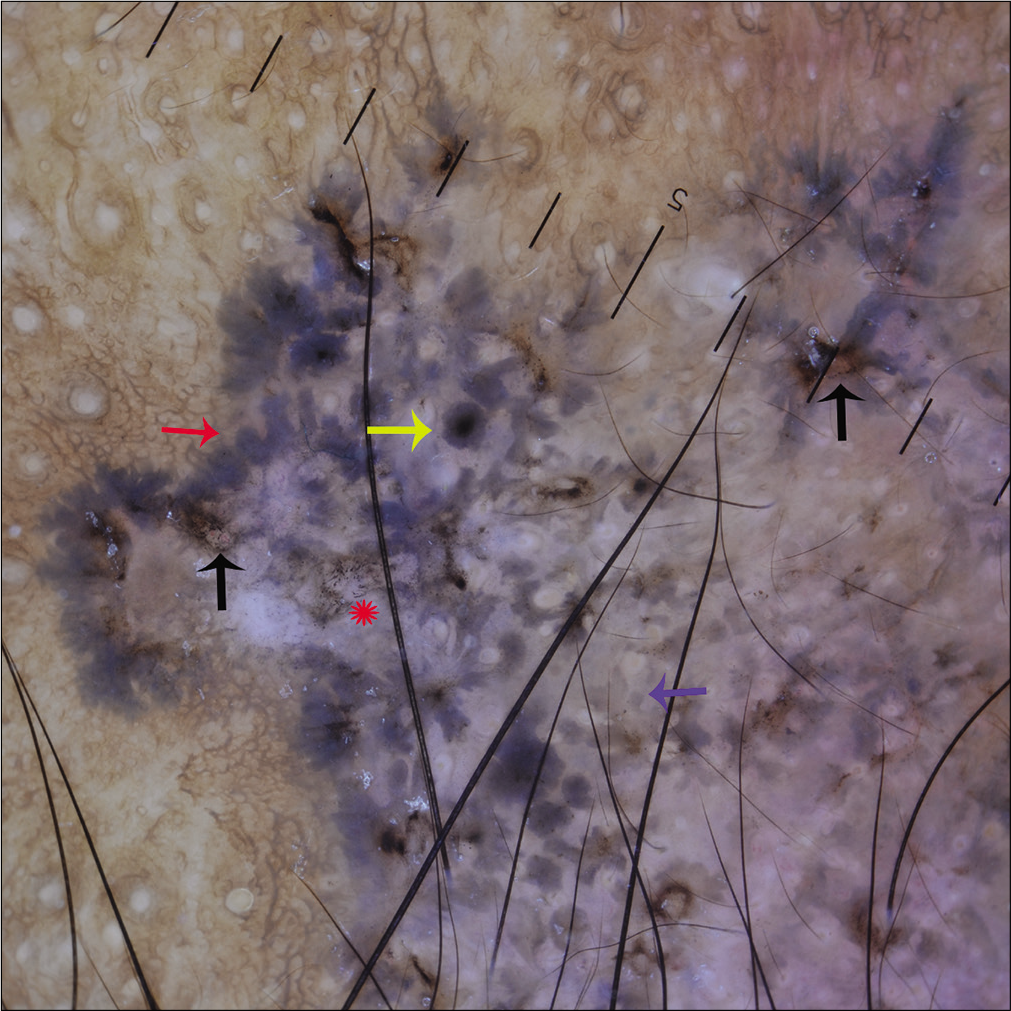
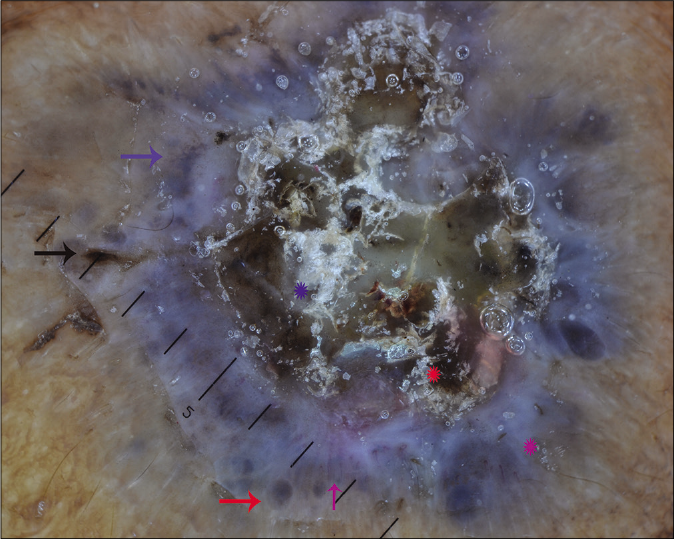
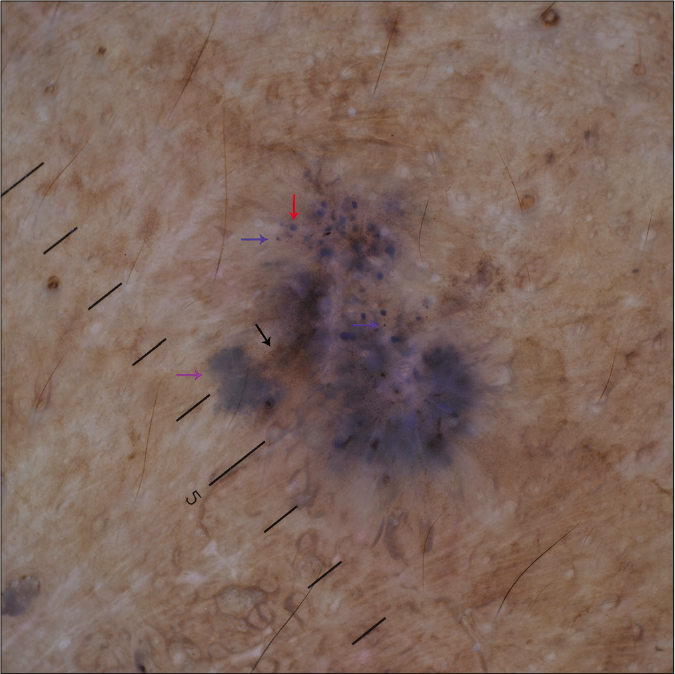
- Dermoscopic examination under nonpolarized contact dermoscopy (HEINE DELTA20® Dermatoscope, ×10) showing brown-gray (blue arrow) to blue-gray (red arrow) maple leaf-like areas, multiple erosions (black arrows), concentric structure (yellow arrow) and multiple blue-gray peppering (Asterix)
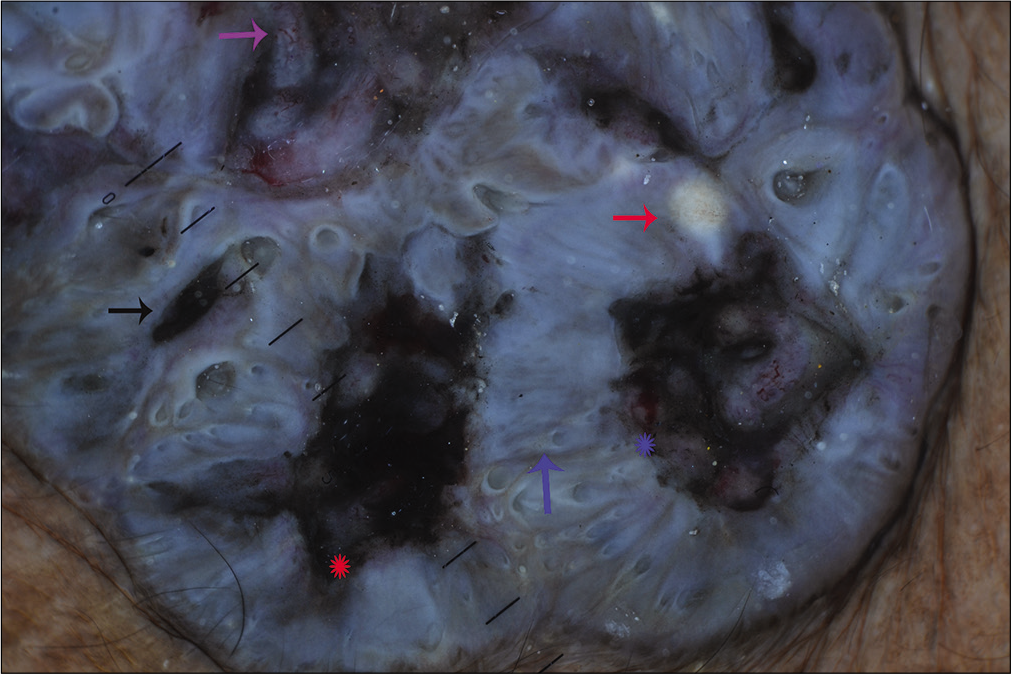
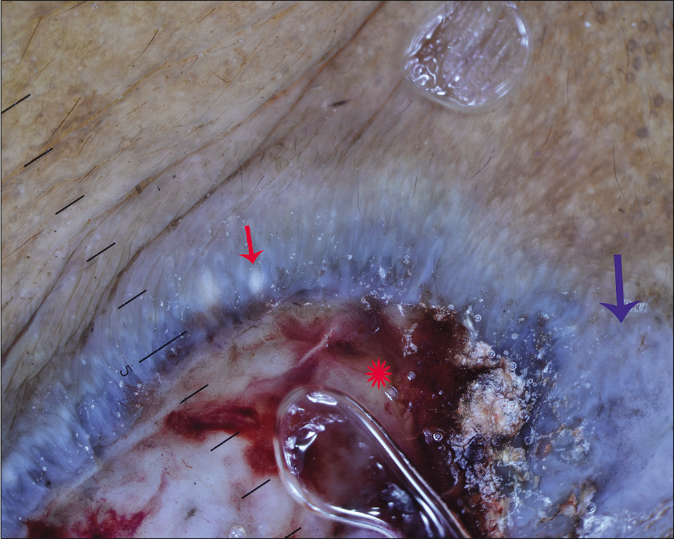
- Dermoscopic examination under nonpolarized contact dermoscopy (HEINE DELTA20® Dermatoscope, ×10) showing blue-white veil (blue arrow), ulceration (red Asterix), micro-ulceration (black arrow), milia-like cyst (red arrow), linear vessels (purple arrow) and hemorrhage (blue Asterix)
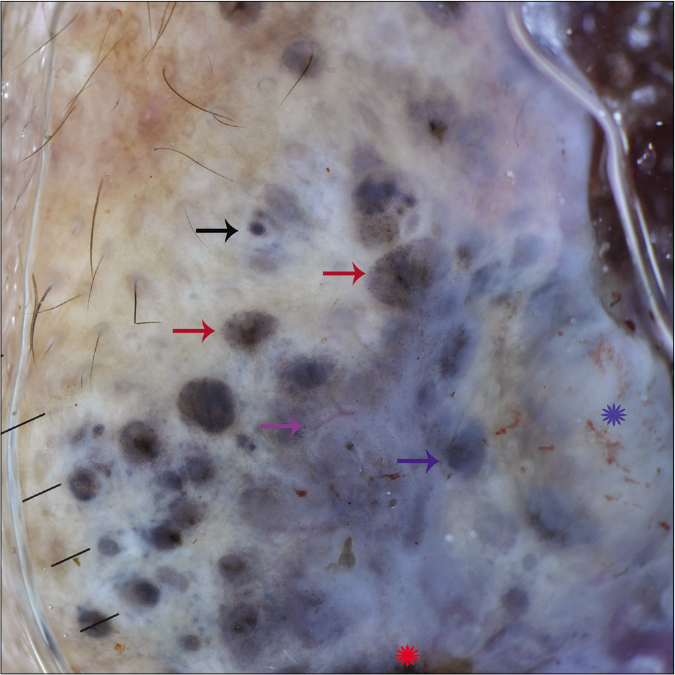
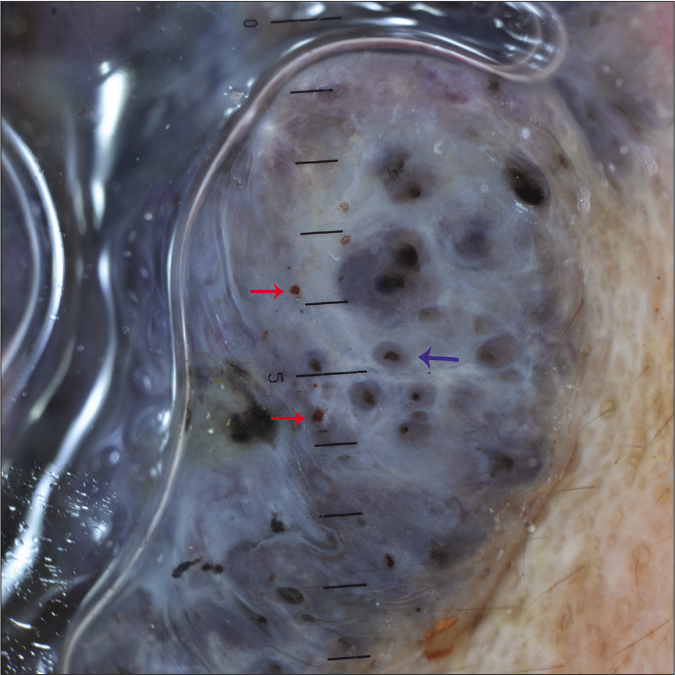
- Dermoscopic examination under nonpolarized contact dermoscopy (HEINE DELTA20® Dermatoscope, ×10) showing gray ovoid nest with brown peppering (red arrows), blue-gray (blue arrow) ovoid nest, blue-gray globules (black arrow), blue-white veil (red Asterix), branching vessels (purple arrow) and hemorrhage (blue Asterix)
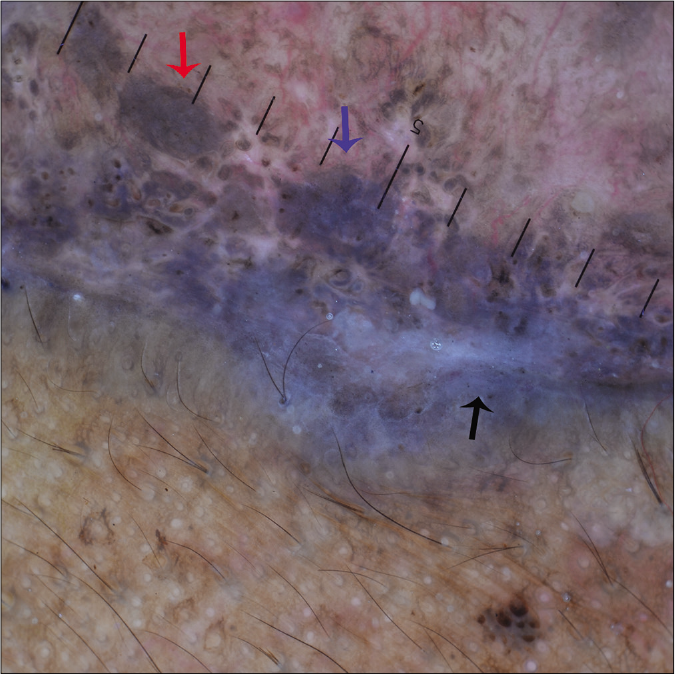
- Dermoscopic examination under nonpolarized contact dermoscopy (HEINE DELTA20® Dermatoscope, ×10) showing large brown-gray (red arrow), blue-gray (blue arrow) ovoid nests and blue-white veil (black arrow)
- Dermoscopic examination under nonpolarized contact dermoscopy (HEINE DELTA20® Dermatoscope, ×10) showing blue-gray aggregate (blue arrow), gray-brown ovoid nests (red arrow), blue-white veil (purple Asterix), brown blotch (red Asterix), keratotic scales (blue Asterix) and hairpin vessels (purple arrow)
| Dermoscopic features | n (%) | |
|---|---|---|
| Classic BCC-associated dermoscopic feature | Ulceration | 29 (48.4) |
| Maple leaf-like area | 37 (61.7) | |
| Brown to blue-gray ovoid nest | 20 (33.4) | |
| Brown to blue-gray globule | 11 (18.4) | |
| Arborizing vessels | 12 (20) | |
| Spoke wheel area | 16 (26.7) | |
| Nonclassic BCC-associated features | Multiple small erosions | 19 (31.7) |
| Short fine telangiectasia | 28 (46.7) | |
| Concentric structure | 8 (13.3) | |
| In-focus dot | 2 (3.3) | |
| Red-white homogenous area | 24 (40) | |
| Nonspecific dermoscopic features | Blue-white veil | 32 (53.4) |
| Brown to blue-gray aggregate/coarse peppering | 26 (43.4) | |
| Brown to blue-gray fine peppering | 41 (68.4) | |
| Brown to black blotch | 12 (20) | |
| Milia-like cyst | 19 (31.7) | |
| Comedo-like opening | 12 (20) | |
| Scale | 14 (23.3) | |
| Peripheral striations | 6 (10) | |
| Follicular plugging | 2 (3.3) | |
| Peri-follicular white ring | 9 (15) | |
| Keratin | 10 (16.7) | |
| Other vascular structures | Hemorrhage | 35 (58.3) |
| Hairpin vessels | 3 (5) | |
| Linear irregular vessels | 2 (3.3) | |
BCC=basal cell carcinoma
| Dermoscopic feature | In nodular BCC, n (%) | In superficial BCC, n (%) | P |
|---|---|---|---|
| Ulceration | 27 (84.3) | 2 (7.4) | <0.001 |
| Maple leaf-like area | 12 (37.5) | 25 (92.5) | <0.001 |
| Brown to blue-gray ovoid nest | 13 (40.6) | 7 (25.9) | 0.2786 |
| Brown to blue-gray globule | 6 (18.7) | 5 (18.5) | 1.000 |
| Arborizing vessels | 12 (37.5) | 0 (0) | <0.001 |
| Spoke wheel area | 1 (3.1) | 15 (55.5) | <0.001 |
| Multiple small erosions | 3 (9.3) | 16 (59.2) | <0.001 |
| Short fine telangiectasia | 12 (37.5) | 16 (59.2) | 0.1206 |
| Concentric structure* | 4 (12.5) | 4 (14.8) | 1.000 |
| Blue-white veil | 26 (81.2) | 6 (22.2) | <0.001 |
| Red-white homogenous area | 6 (18.7) | 18 (66.6) | <0.001 |
| Brown to blue to blue-gray aggregate | 12 (37.5) | 11 (40.7) | 1.00 |
| Milia-like cyst | 12 (37.5) | 7 (25.9) | 0.4093 |
| Comedo-like opening | 10 (31.2) | 2 (7.4) | 0.0277 |
| In-focus dot* | 1 (3.1) | 1 (3.7) | 1.000 |
Discussion
Melanin plays a central role in orchestrating the various dermoscopic features of BCC, especially in the pigmented subtype. Besides the increased epidermal pigmentation, the BCC-associated pigmented structures correlate with the presence of melanin both within (colonized pigmented melanocytes in the tumor lobules) and outside the tumor lobules (free melanin and melanophages).7
The prevalence of pigmented BCC in Caucasians is low (around 10%). However, in our study 95% (57/60 lesions) of BCCs were pigmented.8 All but one case (a patient with oculo-cutaneous albinism) had at least one pigmented structure(s) on dermoscopy. On histopathology and immunohistochemistry (performed in a few cases), pigmented melanocytes staining positive for Melan-A were seen in the tumor lobules [Figures 6-8].
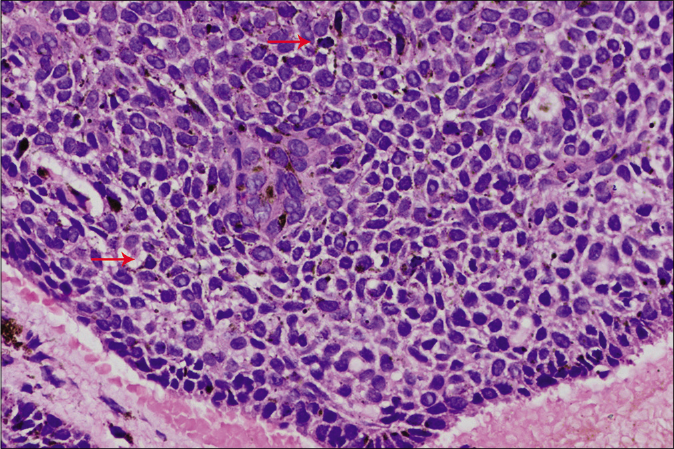
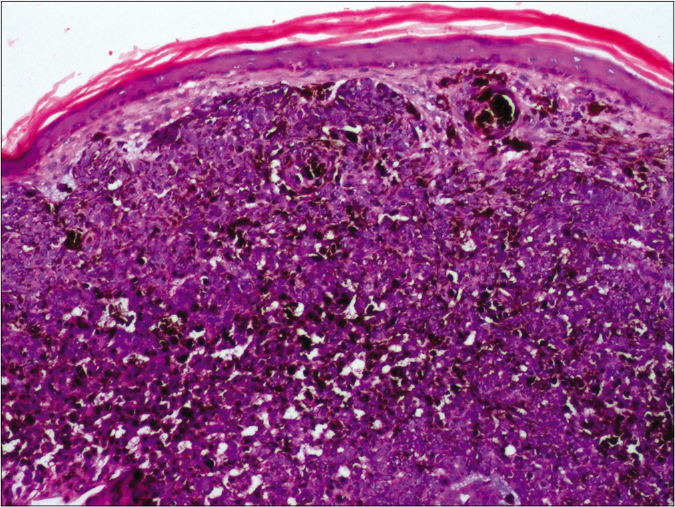
- Basaloid lobule showing colonization by dendritic melanocytes (arrows, H and E, ×400)

- Melan-A demonstrating melanocyte colonization inside basaloid lobules (immunohistochemistry, ×100)
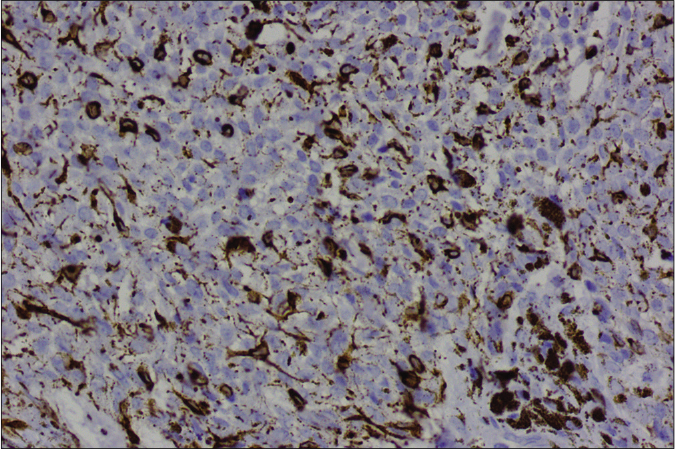
- Melan-A demonstrating dendritic melanocytes (immunohistochemistry, ×400)
The majority of BCCs (57/60, 95%) lacked a pigment network and had at least one of Menzies’ classic BCC-associated dermoscopic features.3 In a recent systematic review, arborizing vessels (59%), shiny white structures (49%) and large blue-grey ovoid nests (34%) were the most common dermoscopic features associated with BCC.9 However, we observed maple leaf-like areas, blue-white veils, ulcerations and short fine telangiectases more frequently and this may be due to the dark skin phototype of our patients. Further, ulceration, blue-white veil and arborizing vessels were significantly associated with nodular BCCs, while superficial BCCs were more often associated with maple leaf-like area, red-white structureless areas, erosion and spoke wheel areas [Figures 9-11]. Similar findings have been reported by others earlier.10,11 The large blue-gray ovoid nests histopathologically correspond to the large pigmented dermal tumor nests invading the dermis [Figure 12], while leaf-like areas to the interconnected basaloid nests attached at the dermo-epidermal junction [Figure 13].
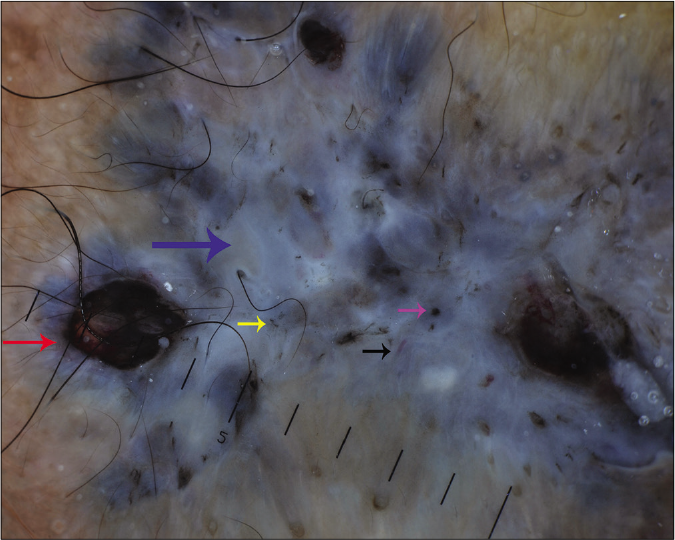
- Dermoscopic examination under nonpolarized contact dermoscopy (HEINE DELTA20® Dermatoscope, ×10) of a nodular basal cell carcinoma dominated by a blue-white veil (blue arrow) and ulceration (red arrow). Other features noted are brown globule (purple arrow), brown peppering (yellow arrow), milia-like cyst and linear vessel (black arrow)
- Dermoscopic examination under nonpolarized contact dermoscopy (HEINE DELTA20® Dermatoscope, ×10) of a superficial basal cell carcinoma showing multiple small erosions (blue arrows), maple leaf-like area (purple arrow), red-white homogenous area (Asterix), grayish-brown ovoid nests (yellow arrows) and short-fine telangiectasia (black arrow). Multiple perifollicular white rings (red arrow)
- Dermoscopic examination under nonpolarized contact dermoscopy (HEINE DELTA20® Dermatoscope, ×10) showing short fine telangiectasia (blue arrow) and spoke wheel pattern (red arrow)
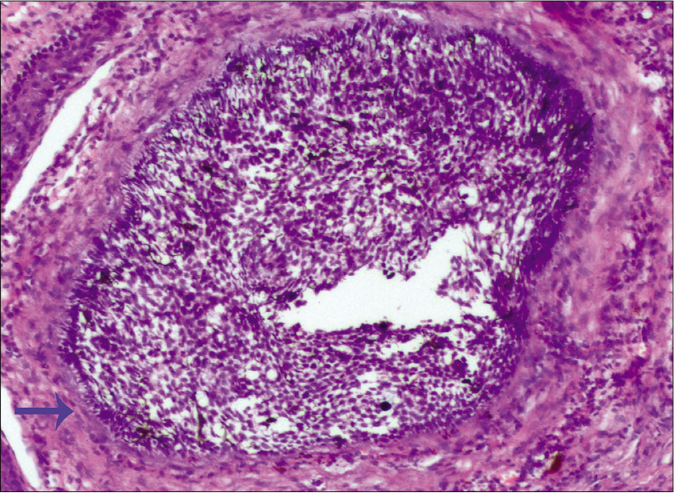
- Large basaloid lobule (arrow) corresponding to the blue-gray ovoid nest (H and E, ×100)
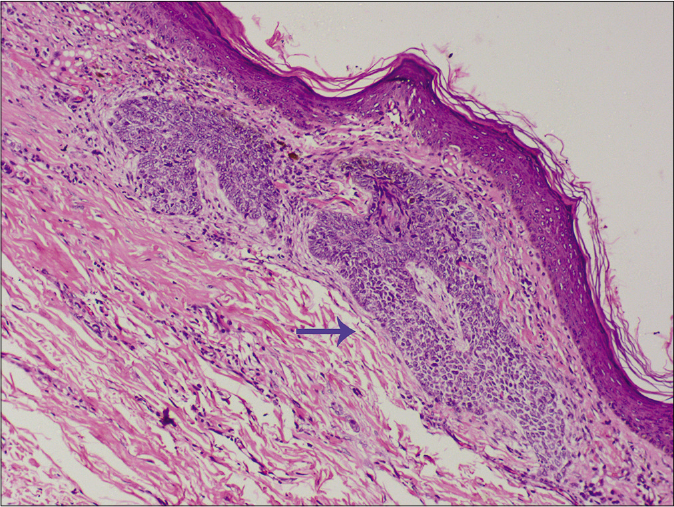
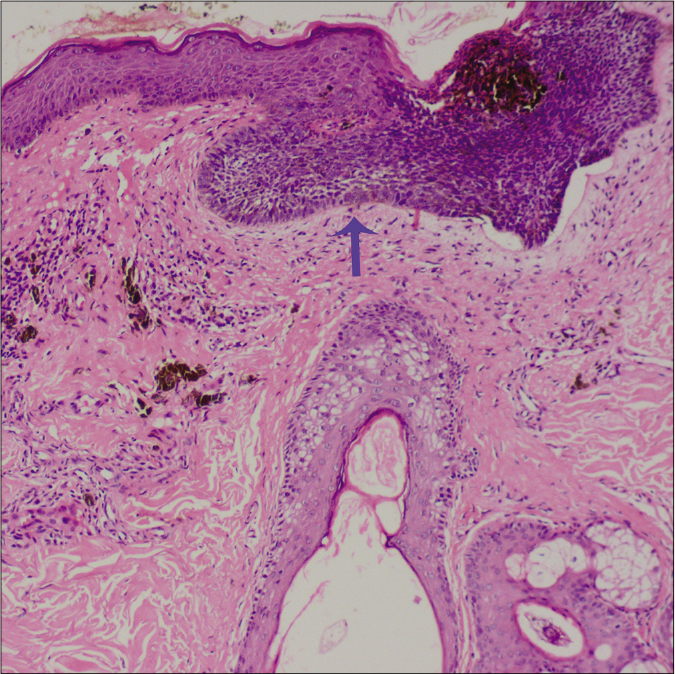
- Basaloid lobules near the dermo-epidermal junction corresponding to the maple-leaf like area (arrow, H and E, ×100)
The blue-white veil was found in almost half of our cases [Figures 12-14] and it was significantly associated with nodular rather than superficial BCCs (P<0.001). The frequent finding of the blue-white veil in BCCs has been noted by others,5,12,13 and the association of this pattern with nodular BCCs has been reported earlier by Suppa and his coworkers.4 The combination of blue-white veil and ulceration was observed in 19 cases of nodular BCCs but none of the superficial BCCs. In 7 of the nodular BCCs with ulceration, the blue-white veil was the only pigmented structure [Figure 14]. The frequent occurrence of the blue-white veil in nodular BCCs may have been responsible for the lower incidence of other pigmented structures in our series. Histopathologically, the blue-white veil corresponds to the heavily pigmented dermal melanocytes and/or melanophages or melanin combined with compact orthokeratosis [Figure 15].13
- Dermoscopic examination under nonpolarized contact dermoscopy (HEINE DELTA20® Dermatoscope, ×10) of a nodular basal cell carcinoma dominated by a blue-white veil (arrow), ulceration (Asterix) and milia-like cyst (red arrow)
- Densely pigmented basaloid cells with overlying compact orthokeratosis corresponding to the blue-white veil (H and E, ×100)
Concentric structures, thought to be precursors of the spoke wheel area, were noted in 13% of the BCCs in our study [Figure 16].4,12,14 They correspond to small tumor nests with darkly pigmented centers arising from (and connected to) the epidermis [Figure 17].
- Dermoscopic examination under nonpolarized contact dermoscopy (HEINE DELTA20® Dermatoscope, ×10) showing concentric structure (blue arrow) and red globules (red arrows)
- Basaloid lobule attached to the epidermis with a densely pigmented central area corresponding to the concentric structure (arrow, H and E, ×100)
In-focus dots are pigmented structures [Figure 18] that are different from the non-focused pepper-like blue-gray dots. They are thought to be the early phase of blue-gray globules and correlate to the free pigment/melanophages/small aggregates of pigmented neoplastic tumor cells.5
- Dermoscopic examination under nonpolarized contact dermoscopy (HEINE DELTA20® Dermatoscope, ×10) showing in-focus dots (blue arrows), blue-gray globules (red arrow), maple leaf-like area (purple arrow) and fine brown peppering (black arrow)
BCC-associated pigment structures (due to the microscopic melanization by colonized melanocytes)15 were seen in 30% of macroscopically nonpigmented BCCs.16 Of the 3 nonpigmented BCCs in our study, only one showed a blue-gray ovoid nest.5
We observed vascular structures in 53.4% of BCCs. These were mostly short fine telangiectasia (28 cases) or arborizing vessels (12 cases), but a few cases showed hairpin and linear irregular vessels. Short fine telangiectasias were seen in 28 BCCs and were in-focus in 8 and out of focus in the rest. Similarly, the arborizing vessels were present in 12 BCCs and were in-focus in 5 of these. Short fine telangiectasias [Figures 10 and 11] were more frequently associated with superficial BCCs, but the differences were not significant.4 The lower incidence of vascular structures in our study could be due to the contact pressure of the dermoscope, the use of nonpolarized dermoscopy (deeper structures are better visualized under polarized mode)17 and the presence of heavily pigmented structures. Suppa et al.4 have reported an inverse relationship between the degree of pigmentation of the BCC and the presence of vascular structures of any type.
The colors observed are sharper and less distorted in the nonpolarized mode when compared to the polarized mode. In the polarized mode colors are darker and render different shades of brown and blue for melanin distributed in the skin.17 Braun et al. using a nonpolarized dermoscope reported findings similar to our study.18 However, they observed a lower frequency of maple-leaf, spoke wheel and concentric structures, which may have been due to the fairer skin color of their patients.18
Limitations
The retrospective nature of the study, the use of only nonpolarized light for examination, the lack of other histopathological variants of BCC and the absence a comparative group were the limitations of the study.
Conclusion
We report the dermoscopic features of BCC from India in patients with skin phototypes IV and V. The majority of the BCCs were pigmented and BCC-associated pigmented structures dominated the dermoscopic features. Dermoscopic features, leaf-like area, red-white homogenous area, erosion and spoke wheel-like area were significantly associated with superficial BCC and blue-white veil, ulceration and arborizing vessel with nodular BCC. A less recognized dermoscopic feature, the blue-white veil, was observed in half of our patients and was significantly associated with nodular BCC. The addition of the blue-white veil as a diagnostic criterion in pigmented BCCs could improve the diagnostic accuracy of dermoscopy in dark skin.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- A study of Basal cell carcinoma in South Asians for risk factor and clinicopathological characterization: A hospital based study. J Skin Cancer. 2014;2014:173582.
- [CrossRef] [PubMed] [Google Scholar]
- The dermatoscopic universe of basal cell carcinoma. Dermatol Pract Concept. 2014;4:11-24.
- [CrossRef] [PubMed] [Google Scholar]
- Surface microscopy of pigmented basal cell carcinoma. Arch Dermatol. 2000;136:1012-6.
- [CrossRef] [PubMed] [Google Scholar]
- Dermoscopic variability of basal cell carcinoma according to clinical type and anatomic location. J Eur Acad Dermatol Venereol. 2015;29:1732-41.
- [CrossRef] [PubMed] [Google Scholar]
- Dermatoscopy of basal cell carcinoma: Morphologic variability of global and local features and accuracy of diagnosis. J Am Acad Dermatol. 2010;62:67-75.
- [CrossRef] [PubMed] [Google Scholar]
- Dermoscopy and dermatopathology correlates of cutaneous neoplasms. J Am Acad Dermatol. 2019;80:341-63.
- [CrossRef] [PubMed] [Google Scholar]
- Basal cell carcinomas are populated by melanocytes and Langerhans [correction of Langerhan's] cells. Am J Dermatopathol. 2001;23:24-8.
- [CrossRef] [PubMed] [Google Scholar]
- Pigmentation, Melanocyte Colonization, and p53 Status in Basal Cell Carcinoma. J Skin Cancer. 2011;2011:349726.
- [CrossRef] [PubMed] [Google Scholar]
- Dermoscopic features of basal cell carcinoma and its subtypes: A systematic review. J Am Acad Dermatol. 2019;7:S0190-9622.
- [CrossRef] [Google Scholar]
- Basosquamous cell carcinoma: A survey of 76 patients and a comparative analysis of basal cell carcinomas and squamous cell carcinomas. Eur J Dermatol. 2013;23:83-6.
- [CrossRef] [PubMed] [Google Scholar]
- Accuracy of dermoscopic criteria for the differentiation between superficial basal cell carcinoma and Bowen's disease. J Eur Acad Dermatol Venereol. 2018;32:1914-19.
- [CrossRef] [PubMed] [Google Scholar]
- Usefulness of Dermatoscopy for the Preoperative Assessment of the Histopathologic Aggressiveness of Basal Cell Carcinoma. Ann Dermatol. 2015;27:682-7.
- [CrossRef] [PubMed] [Google Scholar]
- Correlation between the dermatoscopic and histopathological features of pigmented basal cell carcinoma. J Eur Acad Dermatol Venereol. 2010;24:1317-25.
- [CrossRef] [PubMed] [Google Scholar]
- High magnification digital dermoscopy of basal cell carcinoma: A single-centre study on 400 cases. Acta Derm Venereol. 2014;94:677-82.
- [CrossRef] [PubMed] [Google Scholar]
- Melanization in basal cellcarcinomas: Microscopic characterization of clinically pigmented and non-pigmented tumours. Australas J Dermatol. 2008;49:202-6.
- [CrossRef] [PubMed] [Google Scholar]
- Dermoscopy uncovers clinically undetectable pigmentation in basal cell carcinoma. Br J Dermatol. 2014;170:192-5.
- [CrossRef] [PubMed] [Google Scholar]
- Differences between polarized light dermoscopy and immersion contact dermoscopy for the evaluation of skin lesions. Arch Dermatol. 2007;143:329-38.
- [CrossRef] [PubMed] [Google Scholar]
- Dermoscopy of pigmented skin lesions. J Am Acad Dermatol. 2005;52:109-21.
- [CrossRef] [PubMed] [Google Scholar]




