
Translate this page into:
Impact on quality of life of family members of vitiligo patients in North India: A cross-sectional study using family dermatology life quality index
Corresponding author: Dr. Soumya Agarwal, Department of Dermatology, Era’s Lucknow Medical College, Era University, Sarfarazganj, Lucknow, Uttar Pradesh, India. scorpsoumya@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Agarwal S, Jain C, Shaafie HI, Khalid A, Singh A. Impact on quality of life of family members of vitiligo patients in North India: A cross-sectional study using family dermatology life quality index. Indian J Dermatol Venereol Leprol 2021;87:869-72.
Sir,
Vitiligo is a common acquired depigmenting disorder caused due to progressive loss of melanocytes. The disease affects approximately one–two percentage of the global population, and the highest incidence has been recorded in the Indian subcontinent followed by Mexico and Japan.1,2 Visible disfigurement, especially in pigmented races, can lead to a detrimental impact on patient’s psychosocial status. Such patients are in a constant need of emotional support and motivation from family members/partners to address these issues. But dermatologic disorders like vitiligo have been shown to adversely affect the quality of life of a patient’s family members as well.3
We conducted a cross-sectional study on 158 vitiligo patients and their family members attending dermatology outpatients' department of Era’s Lucknow Medical College and Hospital in Lucknow from February 2019 to February 2020 with an aim to explore the level and specific domains in which quality of life of of family members of vitiligo patients are affected and any correlation of its impairment with the disease parameters. Our inclusion criteria were as follows: (i) all patients with clinically diagnosed vitiligo attending dermatology OPD without any other significant illness or disability, who give a written informed consent for the study and (ii) family members of age greater than 18 years, having a close relationship with the patient (parents/children/spouse/ siblings) and who are living in same household. Exclusion criteria were as follows: (i) an individual with dermatological disorders other than vitiligo and (ii) partners and relatives who report having any skin diseases or other significant illness (including psychiatric illness) that may impair their quality of life. Ethical clearance for the study was obtained from the Institutional Ethics Committee. Out of 158 patients, five patients suffered from other significant illnesses (type 2 diabetes mellitus – three, psoriasis – one and chronic heart disease – one) and three patients did not give consent. Thus, 150 patients and their relatives completed the study. The measurement of the effect of vitiligo on patient’s quality of life was done using dermatology life quality index(DLQI).4,5 and that on family member’s quality of life using family dermatology life quality index(FDLQI).4 Both scales have a scoring range from 0 to 30 with higher scores representing greater impairment in quality of life. A score of 0-1 on the FDLQI was interpreted as having no effect at all on quality of life. Patients and their family members were asked questions in the life quality indices and the investigator filled out the questionnaires. Data were analyzed using Statistical Package for the Social Sciences version 21 software. Appropriate statistical tests, i.e., ANOVA and Pearson coefficient, were used and P < 0.05 was considered as statistically significant.
The mean age of patients was 30.26 ± 14.86 years [Table 1] and the mean duration of disease was 5.67 ± 7.36 years. The mean body surface area involvement was 24.25±20.49 %. The disease was progressive in 124 (82.7%) patients (mean vitiligo disease activity (VIDA) score – 2.15 ± 1.37) [Figure 1]. Sociodemographic characteristics of family members are summarized in Table 2.
| Patient characteristics | Number (n=150) | % |
|---|---|---|
| Sex | ||
| Male | 72 | 48.0 |
| Female | 78 | 52.0 |
| Occupation of patient | ||
| Employed | 44 | 29.3 |
| Retired | 6 | 4.0 |
| Housewife | 35 | 23.3 |
| Student | 52 | 34.7 |
| Unemployed | 13 | 8.7 |
| Site of lesions | ||
| Exposed | 71 | 47.3 |
| Unexposed | 79 | 52.7 |
| Type of vitiligo | ||
| Focal | 70 | 46.7 |
| Universalis | 2 | 1.3 |
| Vulgaris | 78 | 52.0 |
| Relative characteristics | Number | % |
|---|---|---|
| Relation with patient | ||
| Parents | 78 | 52.0 |
| Spouses/partners | 59 | 39.3 |
| Son/daughter | 13 | 8.7 |
| Gender of family member | ||
| Male | 77 | 51.3 |
| Female | 73 | 48.7 |
| Occupation of family member | ||
| Employed | 83 | 55.3 |
| Retired | 2 | 1.3 |
| Housewife | 41 | 27.3 |
| Student | 8 | 5.3 |
| Unemployed | 16 | 10.7 |
| Marital status of family member | ||
| Married | 130 | 86.7 |
| Unmarried | 20 | 13.3 |

- Vitiligo disease activity score of patients
DLQI was affected in 146 (97.3%) out of 150 patients with a range of 0-28 (mean – 13.75 ± 6.69). According to Hongbo bands, 50% of our patients experienced a moderate effect on DLQI, followed by very large (20%), small (18%), mild (9.3%) and no effect (2.6%).6 FDLQI score >2 was recorded in 147 (98%) family members of the patients with a range of 0–28 (mean – 16.77 ± 6.74). Emotional distress was the worst affected domain (2.07 ± 0.84), followed by personal relationships (1.89±0.97), people’s reactions (1.89 ± 1.01), social life (1.77 ± 0.92), physical well-being (1.77 ± 1.03), recreation/leisure activities (1.71 ± 1.04), extra housework (1.63 ± 0.92), burden of care (1.61 ± 0.96), effect on job/ study (1.34 ± 0.99) and household expenditure (0.95 ± 0.90). We categorized the FDLQI scores into mild (scores —0-5), moderate (scores6-10) and severe (scores 11–30), and in our study we found that majority of the family members (81%) had a severe effect on FDLQI [Table 3]. When the responses, “a little,” “quite a lot” and “very much” were combined, emotional distress was the most commonly reported (98%) domain [Figure 2]. Physical well-being was more affected in females (P = 0.012). Female relatives were more adversely affected in the domains of emotional distress (P = 0.013), extra housework (P = 0.044) and effect on job/study (P = 0.029) as compared to male relatives and the difference was statistically significant. Social life restriction (r = –0.175, P = 0.032) and effect on job/study (r = –0.211, P = 0.009) correlated with patient’s age, that is, younger patients were more affected. The effect on job/study was statistically significant in case of parents (P = 0.005). Emotional distress (P = 0.032) and effect on job/study (P = 0.017) were more impaired in married relatives. FLDQI was more affected in relatives of patients with vitiligo vulgaris (18.51 ± 6.07) and vitiligo universalis (17.00 ± 12.73) as compared to focal vitiligo (14.81 ± 6.87) (P = 0.003). The body surface area (%) (r = 0.270, P = 0.001) and VIDA scores (r = 0.219, P = 0.007) showed a statistically significant correlation with FDLQI. We found a strong correlation between DLQI and FDLQI (r = 0.655, P < 0.001).
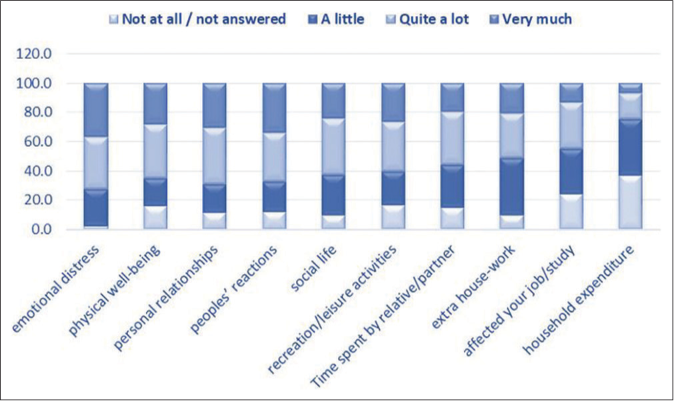
- Family dermatology life quality index items in family members of vitiligo
| Family dermatology life quality index score | Effect | n(%) |
|---|---|---|
| 0–5 | Mild | 9 (6) |
| 6–10 | Moderate | 19 (12.6) |
| 11–30 | Severe | 122 (81) |
Although the devastating impact of vitiligo on patient’s quality of life has been studied extensively, only a few studies that assessed the quality of life of family members of patients with vitiligo have been reported so far.4,7 FDLQI was affected in as high as 98% family members in our study, especially in domains of emotional distress, personal relationships, people’s reactions to the disease and social life. Basra et al. reported emotional impact and burden of care to be the most influenced domains.8 The significant difficulties faced by our subjects in people’s reactions to vitiligo and social functioning can be explained by social stigma attached to this disease in India, especially in parents of young girls as it becomes a major hindrance in their marriages. Among the relatives of patients with vitiligo, gender, relation with the patient and marital status had a significantly greater impact on different items of quality of life. The effect on job/study was more worrisome for parents as they shared a genuine concern about their children’s futurelife. Married relatives were significantly more emotionally perturbed and bothered about the patient’s job/study.
The cosmetic disfigurement perceived by family members of our patients suffering with extensive and active disease was considerably higher regardless of its duration and site. Quality of life of patients and close relatives were strongly related. The emotional disturbance and social inhibition experienced by the patient have a direct impact on psychosocial functioning of their caregivers.
Our analysis showed a much higher degree of deterioration of family members’ quality of life in comparison to the previous similar studies.4,7 It could be due to the social discrimination faced by Indian patients due to easy visibility of lesions and various myths prevalent about this condition, leading to greater perception of disability and thus having a profound bearing on entire family’s psychology.
The limitations of this study are inclusion of patients from a single tertiary care hospital, assessment of only single family member of each patient, lack of control group and the absence of a vitiligo-specific family quality of life scale. A vitiligo-specific family quality of life scale would have taken into account the contribution of sociocultural factors in the burden of vitiligo. Addressing the quality of life of caregivers is of utmost importance in vitiligo because its deterioration can lead to frustration, anger, irritation and anxiety often directed to patients, and this can seriously affect patient’s psychology. It is recommended that quality of life of family members of patients with severe and progressive disease, and impaired dermatology life quality index should be managed adequately through counseling or behavioral therapies.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Vitiligo: A comprehensive overview Part I. Introduction, epidemiology, quality of life, diagnosis, differential diagnosis, associations, histopathology, etiology, and work-up. J Am Acad Dermatol. 2011;65:473-91.
- [CrossRef] [PubMed] [Google Scholar]
- A review of the worldwide prevalence of vitiligo in children/adolescents and adults. Int J Dermatol. 2012;51:1206-12.
- [CrossRef] [PubMed] [Google Scholar]
- The family impact of childhood atopic dermatitis: The dermatitis family impact questionnaire. Br J Dermatol. 1998;138:107-13.
- [CrossRef] [PubMed] [Google Scholar]
- Quality of life in family members of vitiligo patients: A questionnaire study in Saudi Arabia. Amer J Clin Dermatol. 2013;14:489-95.
- [CrossRef] [PubMed] [Google Scholar]
- The psychosocial impact of vitiligo in Indian patients. Indian J Dermatol Venereol Leprol. 2013;79:679-85.
- [CrossRef] [PubMed] [Google Scholar]
- Translating the science of quality of life into practice: What do dermatology life quality index scores mean? J Invest Dermatol. 2005;125:659-64.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of occurrence of vitiligo in children over quality of life of their families: A hospital-based study using family dermatology life quality index. Indian J Paediatr Dermatol. 2018;19:21-5.
- [CrossRef] [Google Scholar]
- The family dermatology life quality index: Measuring the secondary impact of skin disease. Br J Dermatol. 2007;156:528-38.
- [CrossRef] [PubMed] [Google Scholar]




