
Translate this page into:
Vitiligo Impact Scale (VIS)-22: A measure of the psycho-social burden of vitiligo
Corresponding author: Dr. M Ramam, Department of Dermatology and venereology, Teaching Block, Fourth Floor, All India Institute of Medical Sciences, Ansari Nagar, New Delhi 110029, India. mramam@hotmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gupta V, Ramam M. Vitiligo Impact Scale (VIS)-22: A measure of the psycho-social burden of vitiligo. Indian J Dermatol Venereol Leprol 2022;88:691-695.
Introduction
Vitiligo has a significant impact on the psyche, particularly in communities where the contrast with normal brown skin is disfiguring and the condition is socially stigmatized. This impact is usually assessed informally by talking to the patient and/or family members. But in some situations, both in the clinic and in clinical research, it is helpful to have a valid and reliable scale to measure the impact of the disease.
General dermatology scales such as dermatology life quality index (DLQI) and Skindex have been used for this purpose but because they were designed to be applied to a wide variety of skin disorders, these scales contain some questions that are not relevant to vitiligo (e.g., pain or pruritus) and do not cover aspects particularly relevant to vitiligo (e.g., difficulty in marriage). Till recently, vitiligo-specific quality-of-life scales were not available. Vitiligo Impact Scale (VIS) was developed in India in 2013. Around the same time, two other such scales VitiQol,1 and Vitiligo Life Quality Index2 were developed in the United States of America and Turkey respectively.
Development of VIS and refinement to VIS-22
VIS3 was developed with the aim of addressing the concerns of patients with vitiligo. The questions in the VIS were primarily generated from the results of an earlier qualitative study on the psychosocial impact of vitiligo on 50 patients using semi-structured interviews which identified their concerns.4 Other sources included relevant questions from other quality-of-life scales and suggestions from departmental faculty. The final VIS consisted of 27 questions. Internal consistency was demonstrated by Cronbach’s alpha value of 0.83-0.85 for all items.3 The scale had 21 questions common to all patients, with five additional questions for married patients and one additional question for unmarried patients. This imbalance in the denominator required the scale score to be calculated and expressed differently for these two groups of patients. To overcome this problem, item reduction analysis was used to reduce the number of questions for married patients to one and thus, equalize the number of questions for married and unmarried patients.
The modified scale, VIS-22 has 22 questions that cover different domains viz., attitude (questions 1, 4, 17, 19), anxiety (2, 11), social interactions (3, 12, 13), self-confidence (5, 18), depression (6, 9, 10, 14), treatment (7, 15, 16), family (8), marriage (20), occupation (21) and school or college (22). Each question is scored from 0 to 3 (0: not at all, 1: a little, 2: a lot, 3: very much). The total score ranges from 0 to 66 with higher scores indicating a higher effect on life [Figure 1a and b]. Patients find the scale easy to understand and complete.5
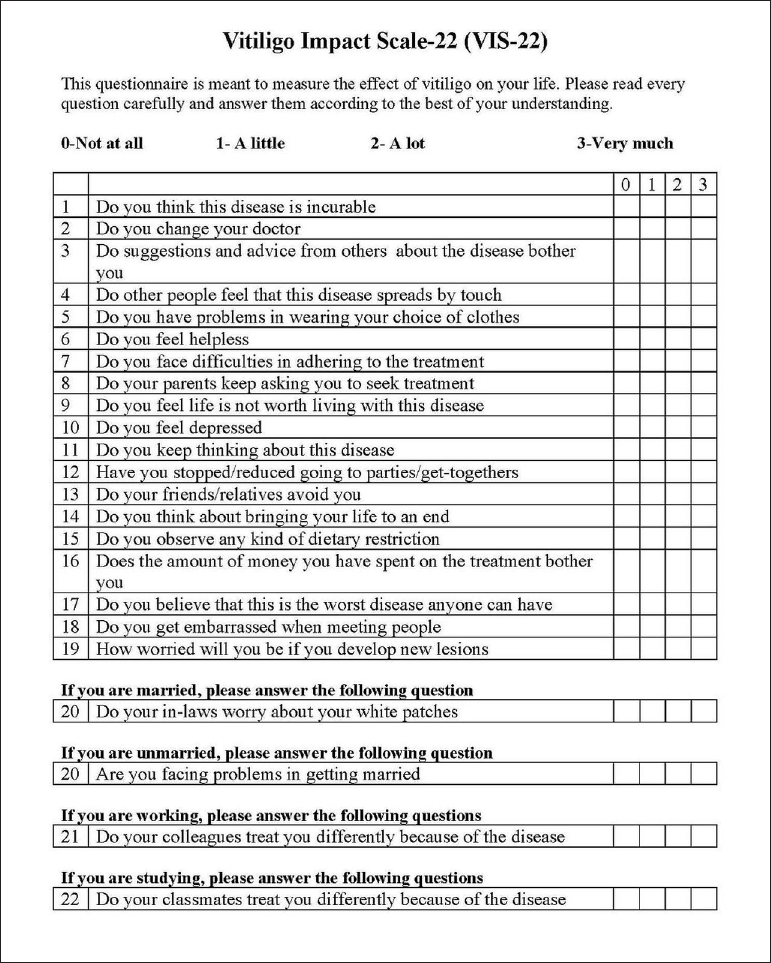
- English version of Vitiligo Impact Scale-22
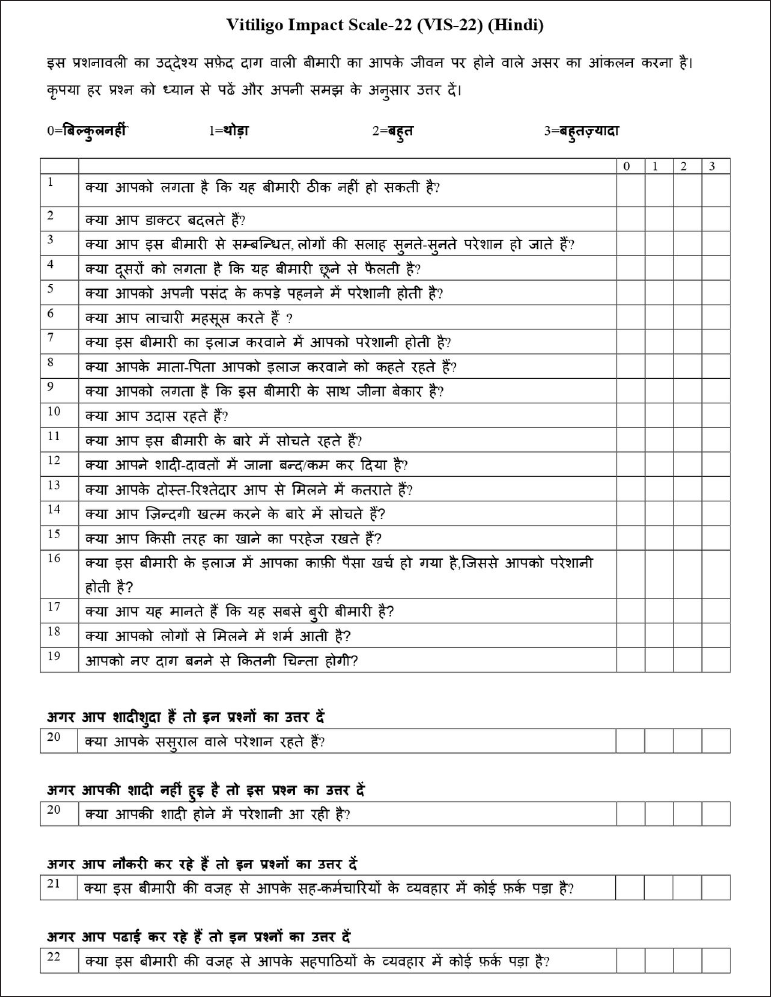
- Hindi version of Vitiligo Impact Scale-22
Validity of VIS-22
Validity refers to whether a scale measures what it intends to, and is one of the fundamental properties of a scale. Validity can be tested in different ways. Criterion validity refers to the correlation of the scale scores with another scale that is considered the gold standard. Convergent validity implies a positive correlation of the scale with other scales that measure the same variable. Known-groups validity assesses the scale’s ability to discriminate between patients known to have differing characteristics.
The criterion, convergent and known-group validity of VIS-22 were demonstrated on a sample of 161 patients (age ≥15 years) with vitiligo. VIS-22 was found to have good criterion validity (strong correlation with patient-perceived severity on visual analogue scale, r = 0.71, P < 0.001) and convergent validity (strong correlation with DLQI, r = 0.71-0.78, P < 0.001; skindex-16, r = 0.72-0.79, P < 0.001). Known-groups validity for VIS-22 scores was shown by higher scale scores for groups expected to have a higher level of distress related to vitiligo; women, patients with progressive disease and those with lower education.5
Test-retest reliability of VIS-22
If a patient’s disease is unchanged between two visits, the scale score should also remain unchanged; this is referred to as test-retest reliability. A two-week interval is chosen between visits so that enough time has elapsed for the person to forget their previous responses but not so much time that the disease has changed significantly.
VIS-22 was administered to 69 patients at an interval of two weeks and the scores at baseline (27.16 + 14.33) and at two weeks (27.26 + 15.62) showed a high correlation (r = 0.91, P = 0.049).5 This indicates that the scale is reliable.
Responsiveness of VIS-22
Scale scores should change when the quality-of-life changes: they should go up if the patient is feeling worse, and go down when they feel better. If the patient feels a lot worse, the score should change more than if they feel only slightly worse, and similarly when they feel better.
This property, referred to as responsiveness, was demonstrated for VIS-22 in 72 patients who were tested at baseline and at the end of 12 weeks. The change in VIS-22 scores correlated moderately well (r = 0.49, P < 0.001) with the change in patient-perceived vitiligo distress. The VIS-22 scores were statistically significantly higher (P < 0.001) in patients whose distress had worsened as compared to those whose distress had reduced. The change in VIS-22 scores also mirrored the change in disease activity; VIS-22 scores were statistically significantly higher when vitiligo worsened, did not change significantly when clinical status remained unchanged and showed a graded decrease for every degree of clinical improvement.5 Similarly, a graded change in VIS-22 scores corresponding to improvement or worsening in the patients’ quality of life was recorded in a subsequent study.6
Clinical meaningfulness of VIS-22 scores
Scale scores are numbers but dermatologists need to know how to interpret the numbers; what does a particular score say about the severity of impact? Interpretability or clinical meaningfulness refers to assigning a severity grade (for example, mild, moderate or severe) to the scale scores.
A study of a cohort of 391 patients showed that a VIS-22 score of 0-5 indicates no impact; 6-15, mild impact; 16-25, moderate impact; 26-40, large impact and 41-66, very large impact.7 The interpretability of VIS-22 scores was studied using an anchor-based approach where a global question (GQ) concerning the effect of vitiligo on patients’ lives ("How much does vitiligo affect your life?") on a five-point Likert scale: 0, no effect; 1, mild effect; 2, moderate effect; 3, large effect and 4, very large effect was used as the anchor. The VIS-22 scores showed a good correlation with the GQ score (r = 0.76, P < 0.001).
Overall, the VIS-22 bands agreed with GQ bands in 197 (51.6%) patients. This was statistically significantly better than the agreement of DLQI bands with GQ in 138 (36.1%) patients. On comparing VIS-22 with DLQI, the latter misclassified patients more frequently (VIS-22, 7.9% vs DLQI, 15.4%). In addition, DLQI placed patients in a lower distress category more frequently than VIS-22 (50.8% vs 20.9%). These findings suggest that VIS-22 may be better than DLQI in assessing vitiligo-related burden and categorizing its severity.7
Minimal important change of VIS-22 scores
If a patient’s scale score is 20 on one occasion and 24 at a follow-up visit three months later, does this represent worsening? If the scores are 36 and 30 respectively, does this mean the patient is feeling better? The minimal important change of a scale refers to the smallest difference in its scores that are considered clinically significant by the patient or clinician.
The minimal important change of VIS-22 scores was estimated to be five points for both improvement as well as worsening. The minimal important change of VIS-22 scores was estimated in a study on 309 patients using an anchor- and distribution-based approach.6 For this purpose, a GQ (see above) and a global rating of change question concerning the change in quality-of-life on a five-point Likert scale (-2, a lot worse;-1, worse; 0, no change; +1, better; +2, a lot better) were used as anchors, while standard error of measurement and one-half of standard deviation was considered as distribution-based estimates. The various estimates for the minimal important change in VIS-22 ranged from 4.1 to 7.05 for both improvements as well as worsening. Practically, a single estimate of five points may be considered as the minimally important change of VIS-22 scores in either direction. In simple terms, it means that a change of VIS-22 scores by five points or more should imply a clinically significant change in the quality of life of the patient.
Limitations
The scale was developed in a culture where vitiligo places a heavy psycho-social burden on patients; its validity in other cultures needs to be studied. A Chinese study found that VIS-22 was better than DLQI in covering aspects of attitude, anxiety and family worries but lacked questions about physical symptoms and sexual activity. They also mentioned that some questions were not suitable for Chinese patients, though they did not mention which ones were unsuitable.
Language versions
VIS-22 was developed in English and Hindi. Studies using Kannada,8 Chinese9 and Urdu10 versions have been published. An unpublished Arabic translation prepared by Egyptian researchers is also available (personal communication).
Permission for use
Permission to use VIS-22 is required but academic, non-commercial use is permitted free of charge. Permission can be obtained by emailing a request to the authors of the scale.
Conclusion
VIS-22 is a valid, reliable and responsive vitiligo-specific quality-of-life scale that was developed to address issues important to patients.11 Scale scores range from 0 to 66 and a score of 26 or higher indicates large or very large impact. A change in score of 5 or more is clinically significant. It is a tool that has been used for vitiligo research8-10,12-14 and can also be used in the clinic.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors are members of the team that developed VIS-22.
References
- Development and validation of a vitiligo-specific quality-of-life instrument (VitiQoL) J Am Acad Dermatol. 2013;69:e11-8.
- [CrossRef] [PubMed] [Google Scholar]
- Development of a quality of life scale for vitiligo. Dermatol Basel Switz. 2013;226:185-90.
- [CrossRef] [PubMed] [Google Scholar]
- Vitiligo impact scale: An instrument to assess the psychosocial burden of vitiligo. Indian J Dermatol Venereol Leprol. 2013;79:205-10.
- [CrossRef] [PubMed] [Google Scholar]
- The psychosocial impact of vitiligo in Indian patients. Indian J Dermatol Venereol Leprol. 2013;79:679-85.
- [CrossRef] [PubMed] [Google Scholar]
- Measurement properties of the Vitiligo Impact Scale-22 (VIS-22), a vitiligo-specific quality-of-life instrument. Br J Dermatol. 2014;171:1084-90.
- [CrossRef] [PubMed] [Google Scholar]
- Determining the minimal important change scores of the Vitiligo Impact Scale (VIS)-22 and Dermatology Life Quality Index (DLQI) scores in Indian patients with vitiligo using anchor- and distribution-based approaches. Br J Dermatol. 2020;183:393-4.
- [CrossRef] [PubMed] [Google Scholar]
- What do Vitiligo Impact Scale-22 scores mean? Studying the clinical interpretation of scores using an anchor-based approach. Br J Dermatol. 2019;180:580-5.
- [CrossRef] [PubMed] [Google Scholar]
- Validation of vitiligo impact scale-22 among North Karnataka population. Clin Dermatol Rev. 2020;4:31-5.
- [CrossRef] [Google Scholar]
- Quality of life of adult vitiligo patients using camouflage: A survey in a Chinese vitiligo community. PloS One. 2019;14:e0210581.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Psychosocial predictors of quality of life in patients with vitiligo. Pak J Psychol Res. 2021;36:19-36.
- [CrossRef] [Google Scholar]
- Measuring quality of life in Indian vitiligo patients. Indian J Dermatol. 2016;61:334-5.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- The impact of vitiligo on patients’ psychological status and sexual function: Cross-sectional questionnaire-based study. Open Dermatol J. 2021;15:23-30.
- [CrossRef] [Google Scholar]
- Quality of life in vitiligo: Relationship to clinical severity and demographic data. Pigment Int. 2017;4:104-8.
- [CrossRef] [Google Scholar]
- Study on assessment of quality of life and depression in patients of vitiligo. Indian Dermatol Online J. 2019;10:153-7.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




