
Translate this page into:
Vertical versus transverse sectioning in histopathological diagnosis of alopecia: A comparative study
Corresponding author: Dr. Shipra Agarwal, Department of Pathology, All India Institute of Medical Sciences, New Delhi, India. drshipra0902@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Yadav D, Mahajan S, Agarwal S, Khandpur S, Pandey A, Singh MK. Vertical versus transverse sectioning in histopathological diagnosis of alopecia: A comparative study. Indian J Dermatol Venereol Leprol 2023;89:126-9.
Sir,
The most appropriate method to section a scalp biopsy is a matter of contention. Different sectioning techniques, all with respective advantages and disadvantages, have been suggested. In the current study, we prospectively compared the accuracy of serial vertical sections with that of transverse sections in the characterisation of primary alopecia after obtaining institutional ethics committee approval (IEC-668/01.12.2017). Consecutive consenting patients with alopecia were recruited after a thorough history and clinical examination. Dermoscopy was used as an additional tool to supplement the clinical diagnosis. Routine workup included relevant blood investigations like haemogram and thyroid function tests. Two 4 mm punch scalp biopsies were taken using standard methods from the most representative area. To determine the normal counts of vellus and non-anagen hair follicles in vertical sections, the uninvolved occipital scalp of six consenting patients of cicatricial alopecia was also biopsied. For transverse and vertical sections, each biopsy was exhausted in eight slides (8–10 sections per slide) while trimming the block in between. These haematoxylin-eosin stained slides were then assessed by two dermatopathologists (SA, DY) independently, blinded to the clinical details. Any possible bias was avoided by separately examining the transverse and vertical sections of each case. Various quantitative and qualitative histological parameters were assessed. For transverse sections, a ratio of ≤4: 1 at the isthmus level was considered abnormal for anagen to non-anagen and terminal to vellus hair ratios.1 For vertical sections, >2 catagen hair per section and >1 vellus hair per section were used as cut-offs for increased non-anagen hair and miniaturisation, respectively. These were in agreement with previous suggestions from literature and our findings on vertical sections from the normal scalp (catagen hair = 0–2/section; vellus hair = 0–1/section).1,2 As the same hair follicle may be visualised on serial vertical sections, follicular ratios could not be calculated on vertical sections due to the lack of a denominator. The disagreement between the two dermatopathologists was resolved with the help of a third dermatopathologist (SK). Statistical analysis was performed using clinicopathological diagnosis as the gold standard and Stata version 16.0 (StataCorp, College Station, TX, U.S.A.). A P-value <0.05 was considered significant. Percentage agreement was calculated between the gold standard and the diagnosis made by combining the results of transverse and vertical sectioning. Percentage agreement was also calculated between the gold standard and the results obtained on transverse and vertical sections individually. Results were analysed using Cohen’s kappa value (value greater than 0.90 indicating almost perfect agreement) between the gold standard (clinico-pathological correlation) and individual sectioning technique (vertical or transverse sectioning).
Seventy-eight alopecia patients (after excluding 8 due to poor sectioning) were recruited. The mean age was 27.7 years; the male: female ratio was 1.4:1, and the mean duration of illness was 4.4 years. There were 43 cases of non-cicatricial alopecia (alopecia areata: 25; androgenetic alopecia: 16; chronic telogen effluvium and trichotillomania: 1 each) and 35 cases of cicatricial alopecia (lichen planopilaris: 15; pseudopelade of Brocq: 12; discoid lupus erythematosus: 4; folliculitis decalvans: 3; linear morphea: 1). Diagnostic agreement was ‘almost perfect’ (k = 0.92, P < 0.001) for transverse sections and ‘moderate’ (k = 0.74, P < 0.001) for vertical sections. On sub-group analysis, the agreements achieved with transverse and vertical sections were ‘almost perfect’ (k = 0.91, P < 0.001) and ‘weak’ (k = 0.50, P < 0.001), respectively in non-cicatricial alopecia; and ‘strong’ (k = 0.87, P < 0.001) with either technique in cicatricial alopecia. Considering individual alopecia types, the diagnostic accuracy of transverse sections was significantly more than vertical sections for alopecia areata (97.7% and 86%, P = 0.05) and androgenetic alopecia (97.7% and 81.4%, P = 0.01). The results were similar with both techniques for lichen planopilaris (vertical section = 100%; transverse section = 97.1%, P = 0.30) and pseudopelade of Brocq (vertical section = 100%; transverse section=97.1%, P = 0.30). Amongst individual parameters, increased non-anagen hair count (39/43, 90.7% vs 23/43, 53.5%, P < 0.001), miniaturisation (40/43, 93% vs 27/43, 62.8%, P = 0.001) and vascular stelae (36/43, 83.7% vs 24/43, 55.8%, P = 0.009) were found significantly more frequently in transverse than vertical sections.
Sectioning technique for a scalp biopsy done for alopecia often depends upon the dermatopathologist’s preference. Cutting transverse sections needs specialised training and may not be preferred in resource-limited settings. While transverse sections allow better assessment of various follicular ratios essential for evaluating non-cicatricial alopecia; vertical sections allow quick examination of all levels of the hair follicle and dermo-epidermal junction helpful in cicatricial alopecia. Data comparing the diagnostic accuracy of transverse and vertical sections is limited and conflicting [Table 1].3-10 In a recent meta-analysis, Du did not find any statistically significant difference between the diagnostic accuracy of transverse and vertical sections for cicatricial and non-cicatricial alopecia.11 Bathish found that serial vertical sections improved the diagnostic yield in 48 (48%) cases. This was higher for non-cicatricial (52.5%) than cicatricial alopecia (48.5%).12 In the current study, we compared the diagnostic accuracy of serial vertical sections with transverse sections. To overcome the shortcoming of a limited number of follicles seen on vertical sections, we exhausted the entire biopsy on eight slides, each having 8–10 sections. Amongst the individual alopecia types, transverse sections did significantly well in alopecia areata and androgenetic alopecia. In our study, five out of 25 (20%) of alopecia areata could not be diagnosed on vertical sections. Transverse sections could establish the diagnosis in all these cases based on features like increased non-anagen hair, miniaturisation, and pigment casts in the absence of characteristic peri-bulbar inflammation [Figure 1].8 In androgenetic alopecia, miniaturisation was missed in seven (43.7%) on vertical sections and in one (6.2%) on transverse sections. Nevertheless, the two techniques did equally well in cicatricial alopecia. Interestingly, epidermal and dermo-epidermal changes could be appreciated equally well on transverse and vertical sections.
| Study | Type of study | Sectioning technique | Number of sections | No. of cases | Percentage cases accurately diagnosed on TS | Percentage cases accurately diagnosed on VS | Conclusion |
|---|---|---|---|---|---|---|---|
| Whiting3, 1993 | Prospective | VS: bisected into half TS: sectioned at the level of entry of sebaceous ducts into the follicle (approximately 1-1.5 mm below the dermoepidermal junction, depending on dermal thickness) |
VS: 6 TS: 24 |
A:106* CA: 0 NCA: 106 |
100% | 93% | TS provided more diagnostic information than VS^ |
| Whiting4, 1995 | Prospective | VS: NS TS: NS |
NS | A: 287# CA: 0 NCA: 287 |
67% | 49% | TS provided more diagnostic information than VS^ |
| Elston5, 2005 | Retrospective | VS: NS TS: step cuts from deeper fat to papillary dermis |
NS | A: 102 CA: 73 NCA: 29 |
78.4% | 94.1% | Combination of TS and VS is better, VS alone had higher concordance than TS alone^ |
| Garcia and Poletti6, 2007 | Retrospective | VS: NS TS: NS |
NS | A: 276 CA: 64 NCA: 202 Normal: 10 |
100% | 100% | TS and VS performed equally well^ |
| Özcan7, 2011 | Prospective | VS: bisected into half TS: sectioned at 1 mm below the dermoepidermal junction |
V: 6$ T: 3-4$ |
A: 47 CA:17 NCA: 30 |
A: 91.5% CA: 76.5% NCA: 100% |
A: 82% CA: 82.4% NCA: 83.3% |
TS better than VS for NCA; TS and VS are equally diagnostic for CA |
| Peckham8, 2011 | Retrospective | VS: NS TS: NS |
NS | A: 15# CA: 0 NCA: 15 |
93.3% | 100% | TS and VS gave comparable results^ |
| Singh9, 2016 | Prospective | VS: NS TS: sectioned around 1–2 mm below the epidermal surface |
NS | A: 30# CA: 0 NCA: 30 |
100% | 93.3% | TS performed better than VS^ |
| Palo10 -, 2017 |
Retrospective | VS: NS TS: sectioned around 1-1.5 mm below the epidermal surface |
NS | A: 228 CA: 44 NCA: 162 Inconclusive: 22 |
90.4% | 90.4% | TS and VS performed equally well^ |
| Present study | Prospective | VS: whole processed, without prior bisection into two halves TS: whole processed without prior bisection into two halves |
VS: 60-80 TS: 60-80 |
A: 78 CA: 35 NCA: 43 |
A: 96.1% CA: 97.1% NCA: 95.3% |
A: 78.2% CA: 94.2% NCA: 65.1% |
TS better than VS for NCA, TS and VS are equally diagnostic in CA |
A: all alopecia cases, CA: cicatricial alopecia, NCA: non-cicatricial alopecia, NS: not specified, VS: vertical, TS: transverse, *: only androgenetic alopecia cases, #: only alopecia areata cases, $: 4 additional sections were examined if required, ^: P -value not mentioned in the study

- Alopecia areata: Smooth non scarring alopecia patch over fronto-temporal scalp
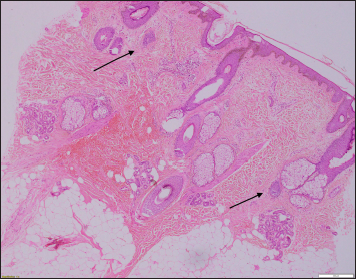
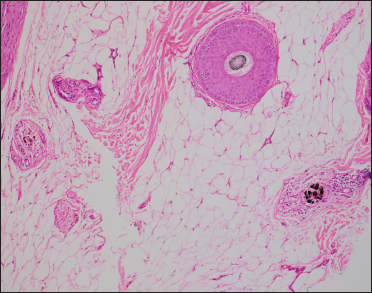
- Alopecia areata: Increased vellus hair (marked with arrows) indicating miniaturisation on vertical sections (H&E, ×40)
- Alopecia areata: Vascular stelae without pigment casts on vertical section (H&E, ×100)
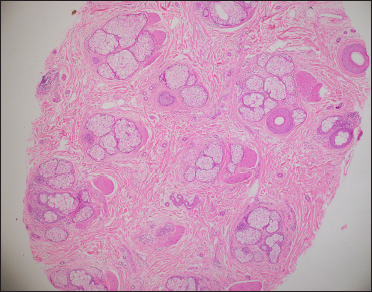
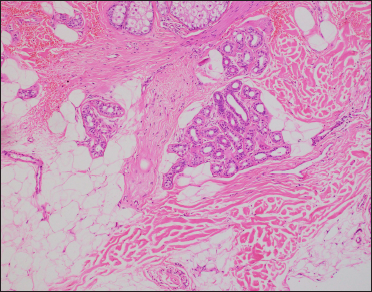
- Alopecia areata: Miniaturisation with increased non-anagen hair count on transverse sections at the level of isthmus (H&E, ×40)
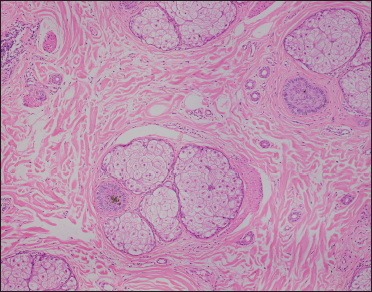
- Alopecia areata: Miniaturised telogen hair with coarse pigment casts on transverse section (H&E, ×100)
- Alopecia areata: Vascular stelae with coarse pigment casts on transverse section at the level of subcutis (H&E, ×100)
Our study used serial vertical sections (reducing the sampling error) and performed appropriate statistical measures for comparing the two techniques. Although there are a few limitations, including a relatively small sample size, especially telogen effluvium cases, and a lack of ancillary studies like immunofluorescence and special stains, we got significant results. Transverse sections performed better than serial vertical sections in non-cicatricial alopecia but equally well in cicatricial cases. Hence, transverse sections should be the preferred technique in the histopathological evaluation of non-cicatricial alopecia. For cicatricial alopecia, either of the two sectioning methods may be used, depending upon the preferences of the laboratory personnel.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflict of interest
There are no conflicts of interest.
References
- An Atlas of Hair Pathology with Clinical Correlations (ed 2). London: Informa Healthcare; 2012.
- [Google Scholar]
- Histopathologic approach to alopecia. Indian J Dermatopathol Diagn Dermatol. 2018;5:79-88.
- [CrossRef] [Google Scholar]
- Diagnostic and predictive value of horizontal sections of scalp biopsy specimens in male pattern androgenetic alopecia. J Am Acad Dermatol. 1993;28:755-63.
- [CrossRef] [PubMed] [Google Scholar]
- Histopathology of alopecia areata in horizontal sections of scalp biopsies. J Invest Dermatol. 1995;104:26S-27S.
- [CrossRef] [PubMed] [Google Scholar]
- A comparison of vertical versus transverse sections in the evaluation of alopecia biopsy specimens. J Am Acad Dermatol. 2005;53:267-72.
- [CrossRef] [PubMed] [Google Scholar]
- Scalp biopsy specimens: Transverse vs vertical sections. Arch Dermatol. 2007;143:268.
- [CrossRef] [PubMed] [Google Scholar]
- Vertical vs. transverse sections of scalp biopsy specimens: A pilot study on the comparison of the diagnostic value of two techniques in alopecia. Clin Exp Dermatol. 2011;36:855-63.
- [CrossRef] [PubMed] [Google Scholar]
- Histologic features of alopecia areata other than peribulbar lymphocytic infiltrates. J Am Acad Dermatol. 2011;65:615-20.
- [CrossRef] [PubMed] [Google Scholar]
- A comparison of vertical and transverse sections in the histological diagnosis of alopecia areata scalp biopsy specimens. Int J Trichology. 2016;8:111-5.
- [CrossRef] [PubMed] [Google Scholar]
- Utility of horizontal and vertical sections of scalp biopsies in various forms of primary alopecias. J Lab Physicians. 2018;10:95-100.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnostic value of horizontal versus vertical sections for scarring and non-scarring alopecia: A systematic review and meta-analysis. Eur J Dermatol. 2016;26:361-9.
- [CrossRef] [PubMed] [Google Scholar]
- A study of serial vertical sectioning of scalp biopsies to increase the histological diagnostic yield in alopecias. J Eur Acad Dermatol Venereol. 2010;24:709-15.
- [CrossRef] [PubMed] [Google Scholar]




