
Translate this page into:
A challenging case of Kyrle’s disease successfully treated with apremilast

Corresponding author: Dr. Apaopa Jemima Thekho, Department of Dermatology, Venereology and Leprosy, ESIC Medical College & Hospital, NIT-3, Faridabad, Haryana, India. thekho9@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Uikey D, Thekho AJ, Godara A. A challenging case of Kyrle’s disease successfully treated with apremilast. Indian J Dermatol Venereol Leprol. doi:10.25259/IJDVL_940_2024
Dear Editor,
A 29-year-old woman, with multiple chronic conditions including type 1 diabetes mellitus, hypertension, pancreatitis, gastric ulcer, hypothyroidism, and depression, visited the dermatology department with generalised hyperkeratotic papules associated with intense itching for the past four years. Examination revealed multiple discrete papules and nodules with central keratotic plugs accompanied by excoriations and post-inflammatory hyperpigmentation. Her upper and lower extremities had most of the lesions, with a few on her lower back and face body surface area (BSA>20%); the Koebner phenomenon was also observed [Figure 1a].

- Multiple discrete papules and nodules with central keratotic plugs on both lower legs.
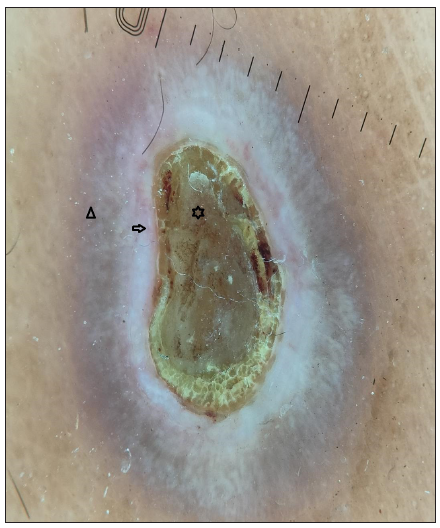
- Dermoscopy revealed four zones: a central keratotic plug with a structureless white area (black star), a structureless pink area with dotted vessels (black arrow), and a structureless brown area in concentric rings (black triangle); (Dermlite DL5, 10 X, polarised mode).
Dermoscopy (Dermlite DL5 in polarised mode) revealed four zones: a central keratotic plug with a structureless white area, a structureless pink area with dotted vessels, and a structureless brown area in concentric rings [Figure 1b]. Clinical differentials of perforating dermatosis (PD) and excoriated prurigo nodularis were considered. The haematological investigations revealed a significant elevation in blood glucose levels, with HbA1c reading of 11.5%. Complete haemogram, liver, and kidney function tests were normal, and anti-thyroid peroxidase or anti-islet cell antibodies were not detected. Other findings were atrophic pancreas with areas of calcification on computed tomography (CT), pangastritis, and duodenitis on upper gastrointestinal (GI) endoscopy. A punch biopsy from a keratotic papule was sent for histopathology, which depicted a cornified plug with basophilic debris embedded in an epidermal invagination with perifollicular inflammatory infiltrate [Figure 2a and 2b]. Special stains for collagen and elastin were negative. A final diagnosis of Kyrle’s disease (KD) with multisystem pathologies was made.
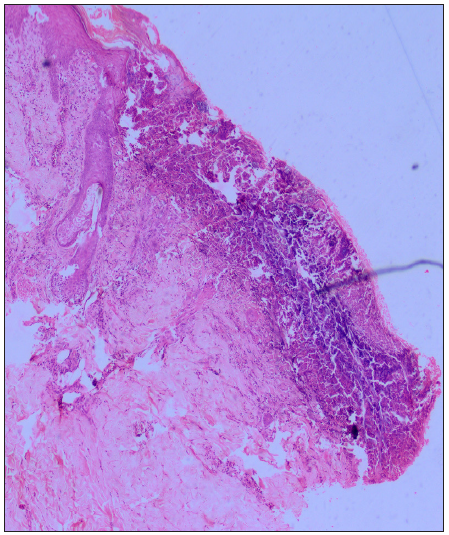
- Cornified plug with basophilic debris in an epidermal invagination. (Haematoxylin and eosin, 40x).
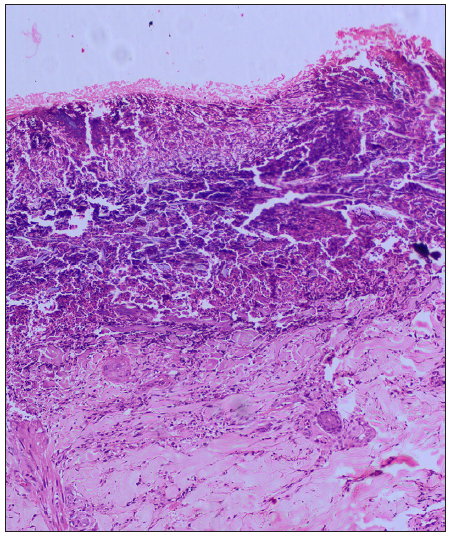
- Basophilic debris with no collagen or elastic fibres (Haematoxylin and eosin, 100x).
Based on the perforating dermatosis (PD) severity score suggested by Kawakami et al., the patient had an Eczema Area and Severity Index (EASI) of 12.2/36 and a pruritus score of 8/10, attaining a total score of 13 which comes under moderate (7–15) involvement.1
Considering the severity and its detrimental effect on the patient’s quality of life, systemic treatment was deemed appropriate. Systemic steroids and oral retinoids were not considered due to underlying comorbidities. Apremilast, a phosphodiesterase inhibitor was considered for treating this patient along with topical keratolytics. After three months of starting apremilast 30mg twice a day, the patient’s itch severity score improved significantly from 9 to 3. There has been a notable decrease in both new and existing lesions [Figure 3]. PD severity score also decreased from 13 to 4. Our patient has been maintaining the clinical response for the past eight months, without experiencing any adverse events.
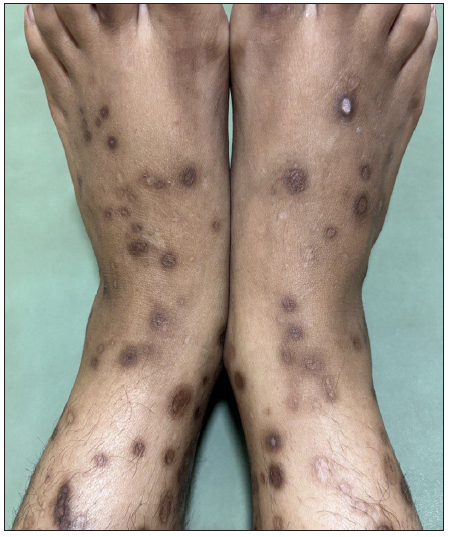
- Significant clinical improvement of skin lesions after four months therapy with apremilast.
KD is a type of acquired perforating dermatosis (APD), commonly observed in adults (30–50 years), predominantly among females. The condition manifests as discrete hyperkeratotic papules and nodules, predominantly affecting the extensor surface of the limbs, accompanied by pruritus and koebnerisation. Excoriated prurigo nodularis, insect bite hypersensitivity, chronic folliculitis, and other APDs are among the diagnostic considerations.
The exact pathogenesis of KD remains unclear. Due to its frequent associations, underlying systemic disorders are considered as the main etiology. Some factors that contribute to this are uremia (renal diseases), hyperphosphatemia, elevated fibronectin levels, advanced glycated end products (diabetes), abnormal low-density lipoprotein (LDL) levels (diabetes and lipid disorders), and occasionally infections. The proposed final pathway involves a disruption in the epidermal keratinisation process, leading to the accumulation of abnormal keratin. This triggers inflammation, resulting in the expulsion of material via the epidermis followed by re-epithelisation.2,3 Histologically, the epidermis is hyperplastic with cup-shaped invagination and a degenerative basophilic material with plug formation and no collagen or elastic fibres.4
The treatment of KD poses challenges and often yields unsatisfactory outcomes. Treatment options include topical corticosteroids, keratolytics, retinoids, oral corticosteroids, immunosuppressants, and phototherapy, but with limited effectiveness. Oral upadacitinib (oral selective Janus kinase [JAK] 1 inhibitor) has emerged as a novel treatment approach because of its action on JAK/signal transducers and activators of the transcription (STAT) pathway.3
Apremilast (phosphodiesterase-4 inhibitor) prevents the degradation of cyclic adenosine monophosphate (cAMP), which results in an antagonistic effect on the production of proinflammatory cytokines (TNF-α, IL-23, interferon (IFN)-γ and an increase in anti-inflammatory mediators (e.g. IL-10).5 This broad-spectrum anti-inflammatory action leads to a reduction in inflammatory cell infiltration in the epidermis, the inflammatory response against keratin, normalisation of epidermal keratinisation preventing hyperkeratosis, and reduction in itch severity.6
We encountered only a single case report describing a patient with Down syndrome who had psoriasis, hidradenitis suppurativa (HS), and PD. The patient’s PD showed a remarkable response to apremilast, which was initially prescribed for the treatment of psoriasis and HS.7
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of AI-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Clinical practice guide for the treatment of perforating dermatosis. J Dermatol. 2020;47:1374-82.
- [CrossRef] [PubMed] [Google Scholar]
- Dupilumab improve acquired reactive perforating collagenosis characterized by type 2 inflammation. Front Immunol. 2023;14:1240262.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- A potential new treatment with upadacitinib for acquired reactive perforating collagenosis. JAAD Case Rep. 2024;48:112-4.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Degenerative diseases and perforating disorders. Lever’s Histopathology of the Skin (11th edition). Philadelphia: Wolters Kluwer; 2015. p. :1006-36.
- Apremilast: A novel PDE4 inhibitor in the treatment of autoimmune and inflammatory diseases. Ther Adv Musculoskelet Dis. 2010;2:271-8.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Apremilast (Otezla): A New Oral Treatment for Adults With Psoriasis and Psoriatic Arthritis. P T. 2015;40:495-500.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Treatment of a perforating dermatosis with apremilast. JAAD Case Rep. 2021;16:155-7.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




