
Translate this page into:
Detection of a novel genetic variant in a patient with Berardinelli–Seip syndrome

Corresponding author: Dr. Sakshi Patidar, Department of Dermatology, Venereology and Leprosy, B. J. Medical College, Ahmedabad, India. sakshipatidar875@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Pandya RM, Patidar S, Joshi RR. Detection of a novel genetic variant in a patient with Berardinelli–Seip syndrome. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_685_2024
Dear Editor,
Lipodystrophies constitute a heterogeneous group of disorders with selective loss of peripheral subcutaneous fat accompanied by accumulation of visceral fat. Berardinelli–Seip congenital lipodystrophy (BSCL) or congenital generalised lipodystrophy (CGL) is a rare disorder resulting from defective adipocyte differentiation and/or lipid droplet formation.1 Here we report a patient with Berardinelli–Seip congenital lipodystrophy Type 2.
A 11-year-old female, first born of a third-degree consanguineous marriage, presented with complaints of loss of fat all over the body, hyperpigmentation of the neck and body folds, and developmental delay since 3 years of age. Her mother reported poor weight gain despite a voracious appetite along with extreme discomfort in hot weather. She was born at full term by normal vaginal delivery. There was no family history of similar complaints [Supplementary Figure 1].
General examination revealed cadaveric triangular facies, curly brittle hair, mild prognathism [Figure 1a], muscular body habitus [Figure 1b], and acromegalic hands and feet. We noted generalised absence of subcutaneous fat, hypertrophy of pectoral, deltoid, and thigh muscles along with engorged subcutaneous veins [Figure 1c]. Her skin was thick and hyperpigmented over the neck and bilateral axillae [Figure 2a], popliteal [Figure 2b] and antecubital fossae [Figure 2c]. Oral examination revealed tonsillar hypertrophy with a right-sided deviation of the uvula [Figure 3]. The remaining mucosae and genitalia were unremarkable. Her body mass index was 28.1 kg/m2. Intelligence quotient assessment revealed intellectual deficiency. Tanner’s stage of sexual maturity was found to be I. We considered congenital generalised lipodystrophy, progeroid syndromes such as Werner syndrome and Hutchinson–Gilford syndrome as differentials.

- Cadaveric triangular facies, prognathism, and curly hair.
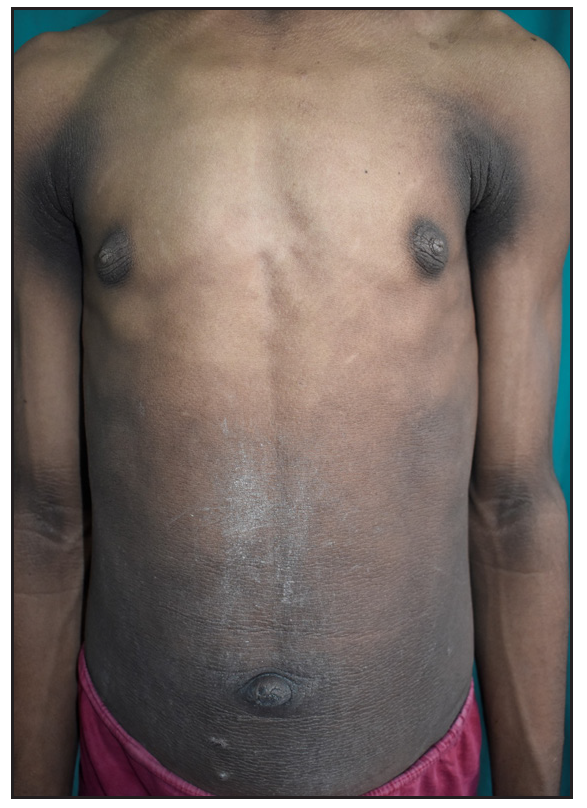
- Muscular body habitus with prominent pectoral muscles.

- Prominent subcutaneous veins.
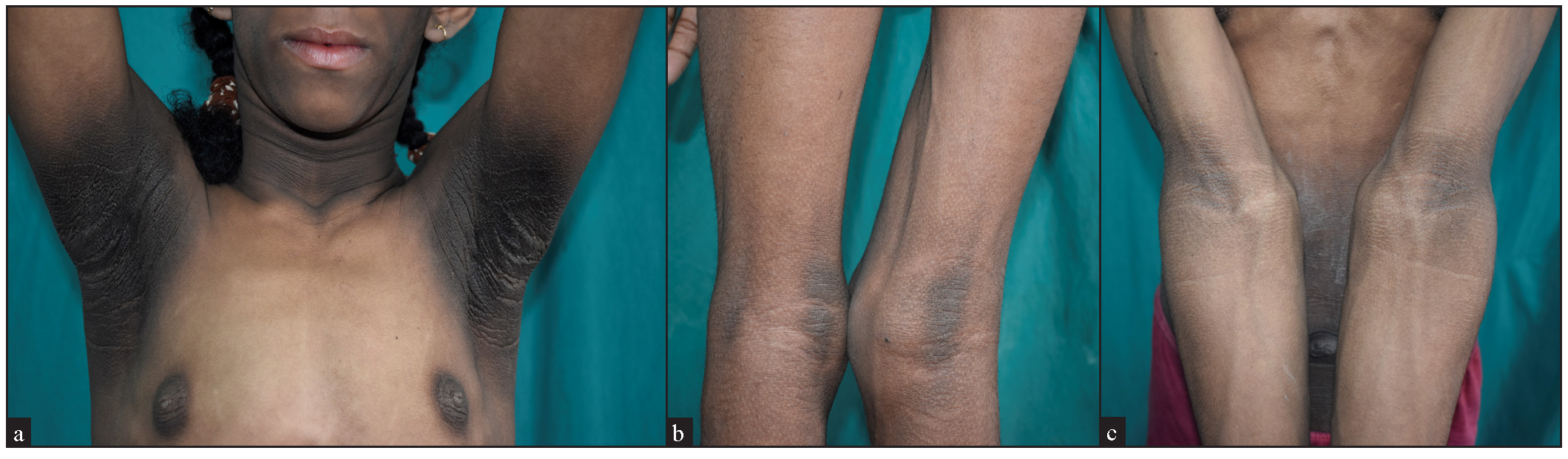
- Thickened and hyperpigmented skin (Acanthosis nigricans) over (a) Neck and bilateral axillae, (b) Popliteal and (c) Anti-cubital fossae.
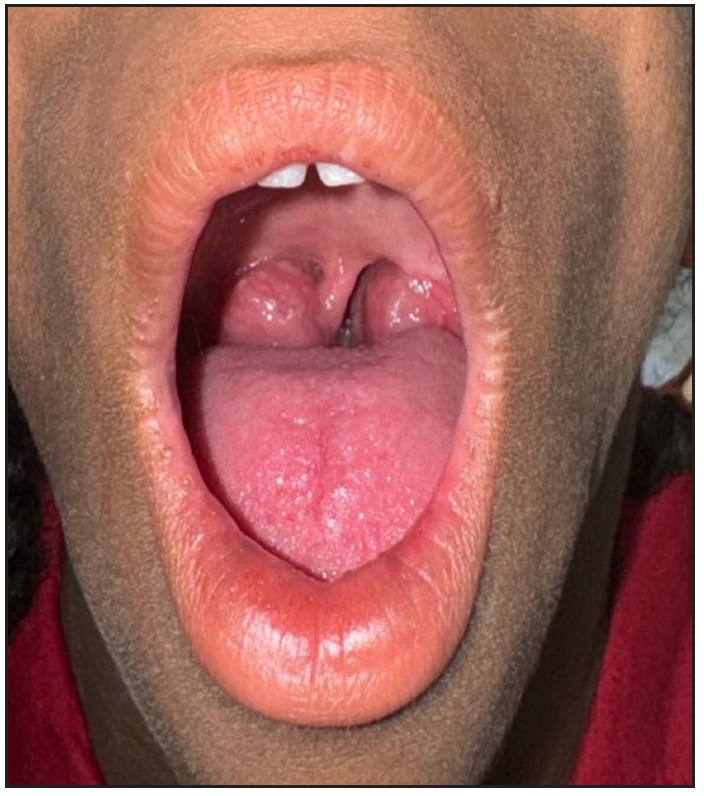
- Tonsillar hypertrophy with a right-sided deviation of uvula.
Laboratory investigations revealed elevated liver enzymes (aspartate transaminase/AST - 76 IU/L, alanine transaminase/ALT - 109 IU/L). Serum total triglycerides and very low-density lipoprotein (VLDL) levels were raised with values of 224 mg/dL and 44.8 mg/dL, respectively while high-density lipoprotein (HDL) level was low at 20 mg/dL. Fasting blood sugar level was 114 mg/dL and postprandial blood sugar level was 191 mg/dL with an elevated glycosylated haemoglobin (HbA1c) level of 7.6%. Serum fasting insulin was raised with a value of 28 µIU/mL (normal: 2–25 µIU/mL) suggesting insulin resistance. Urine routine microscopic examination revealed traces of sugar. Creatine phosphokinase (MB) and total levels were elevated with values of 38 and 268 IU/L, respectively. Hemogram, thyroid function test and renal function tests including serum electrolytes were within normal limits. Serology for Human Immunodeficiency Virus infection was negative. Abdominal ultrasonography demonstrated hepatomegaly (18.5 cm) with bright echogenicity. Electrocardiogram, echocardiography, and ophthalmologic evaluation revealed no abnormality. X-ray of the skull, trunk, and limbs detected normal bone age.
Considering the age of onset, characteristic dysmorphology, and metabolic derangement, a diagnosis of congenital generalised lipodystrophy was made. Targeted genome sequencing detected homozygous single base pair duplication in exon 7 of the BSCL2 gene [c.825dup (p.Ala276SerfsTer62)] with a depth of 505x and coverage of >80–100x classified as pathogenic for the syndrome (in silico prediction: damaging by MutationTaster2). This confirmed the diagnosis of Berardinelli–Seip syndrome type 2 variant. She was advised to follow a low-fat diet and regular daily exercise. She was prescribed tablet Metformin (500 mg) and tablet Pioglitazone (15 mg) twice daily following endocrinologist consultation. The patient was however lost to follow up.
Berardinelli–Seip syndrome was first reported by W. Berardinelli in 1954 in Brazil and later confirmed by Martin Seip in 1959 in Norway.2 It is an autosomal recessive disorder with four known genetic subtypes wherein the two major forms, types 1 and 2, are caused by mutations in genes AGPAT2 and BSCL2/seipin, respectively. These mutations result in abnormal adipocyte function leading to metabolic syndrome. Insulin resistance stimulates keratinocytes and fibroblasts resulting in acanthosis nigricans.3
According to the criteria proposed by Lionel Van Maldergem, the diagnosis of BSCL is established with three major or two major criteria plus two or more minor criteria and/or by the identification of biallelic pathogenic variants in AGPAT2 or BSCL2 [Supplementary Table 1].2 Evaluation includes assessment of pubertal states, neurological, endocrinological, cardiovascular, ophthalmological and orthopedic consultations. Out of >250 genetically confirmed cases worldwide and >12 mutations detected in the BSCL2 gene through screening of 1000 genomes, ExAC databases, the genetic variant detected in our case was not found to be reported.4,5 Longitudinal survelliance of these patients is imperative to monitor for sequelae of diabetes, cirrhosis, premature atherosclerosis, pancreatitis, and hypertrophic cardiomyopathy.6
Lifestyle modifications including a low-fat diet rich in omega-3 polyunsaturated fatty acids along with exercise can improve metabolic syndrome. Thiazolidinediones (PPAR-γ agonists) and fibrates (PPAR-α agonists) can be used to treat hypertriglyceridemia. Recombinant methionyl human leptin (r- metHuLeptin) is a novel, effective, promising option for long-term treatment.7
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Lipodystrophies. In: Bolognia JL, ed. Dermatology (4th ed). Elsevier; 2018. p. :1758-74.
- [Google Scholar]
- Berardinelli-Seip Congenital Lipodystrophy. 2003 Sep 8 [Updated 2016 Dec 8].
- Berardinelli-seip syndrome in a 6-year- old boy. Indian J Dermatol Venereol Leprol. 2008;74:644-6.
- [Google Scholar]
- Congenital generalized Lipodystrophy of Berardinelli-Seip type: A rare case. Indian J Dermatol Venereol Leprol. 2011;77:402.
- [Google Scholar]
- Berardinelli Seip Congenital Lipodystrophy Syndrome: 10 Year Follow-up. Indian Pediatr.. 2019;56:877-8.
- [Google Scholar]
- Berardinelli-seip congenital lipodystrophy in two siblings. Indian Dermatol Online J. 2014;5:S20-2.
- [Google Scholar]




