
Translate this page into:
Black grains in cough: Revisiting chest wall eumycetoma
Corresponding author: Dr. Sujay Khandpur, Department of Dermatology and Venereology, All India Institute of Medical Sciences, New Delhi, Delhi, India. sujay_khandpur@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Ahuja R, Aulakh RS, Verma V, Dixit S, Aggarwal A, Khandpur S. Black grains in cough: Revisiting chest wall eumycetoma. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_1204_2024
Dear Editor,
A 38-year-old male farmer presented with a well-defined, hard, indurated swelling on the left posterolateral chest. There were multiple overlying erythematous nodules and sinuses discharging pus and black grains [Figure 1]. The intervening areas showed depigmentation with scarring.

- Involvement of left posterolateral thoracic wall in the form of ruptured nodules and discharging sinus with granulation tissue and black grains.
The lesion had begun as a single cystic swelling initially over his left lateral chest more than 10 years ago which was incised and drained. Over the years, the swelling became indurated and expanded, extending from the left anterior axillary line to the paraspinal region and from the 4th to the 11th rib with multiple nodules and discharging sinuses. He did not recall any preceding local trauma. Despite multiple courses of antibiotics including antituberculosis treatment (ATT), there was no improvement. About a year ago, he developed a productive cough with sputum mixed with blood, pus, and tiny black grains. He had no known comorbidities and his blood sugar and viral markers were unremarkable.
Potassium hydroxide smear from the crushed grains discharged from the sinuses and from the sputum revealed thick septate hyphae. Skin biopsies were sent for histopathological examination, fungal culture, and Polymerase chain reaction (PCR). Haematoxylin and eosin staining revealed numerous neutrophilic abscesses in the dermis with multiple grains containing spores and hyphae embedded within a brown cement-like substance [Figures 2a], surrounded by deep eosinophilic material, indicating the Splendore–Hoeppli phenomenon. The fungal profile was better highlighted on the gomori methanamine silver (GMS) stain [Figure 2b]. The tissue specimen was positive for pan-fungal PCR, although no growth was observed on Sabouraud dextrose agar from either the tissue specimen or the grains.
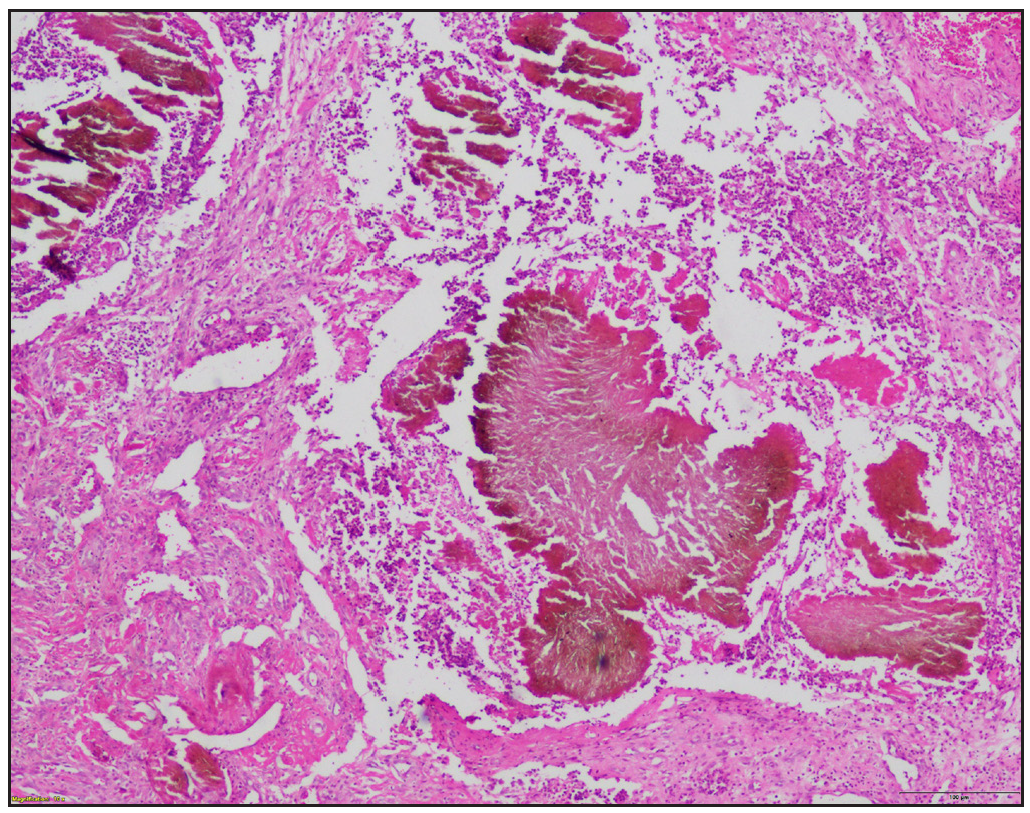
- Grains with broad hyphae embedded in a brown cementum (Haematoxylin and eosin, 40x).
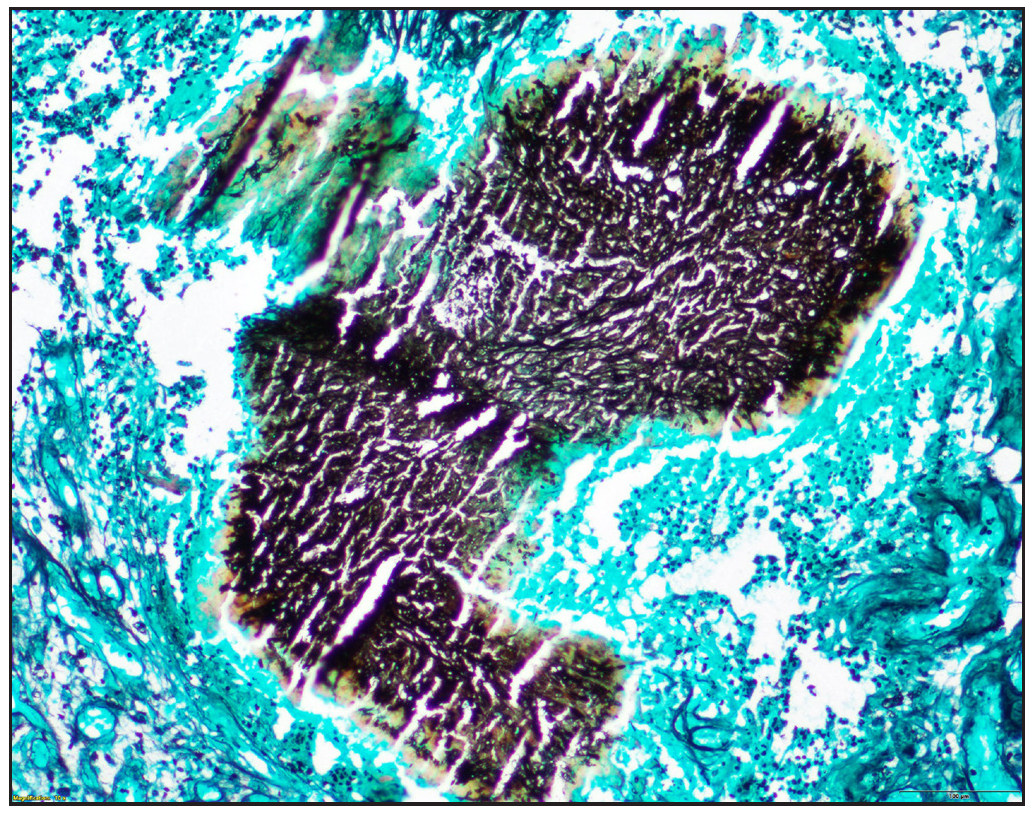
- On Gomori’s methenamine silver stain, the thick fungal hyphae stained black (GMS, 100x)
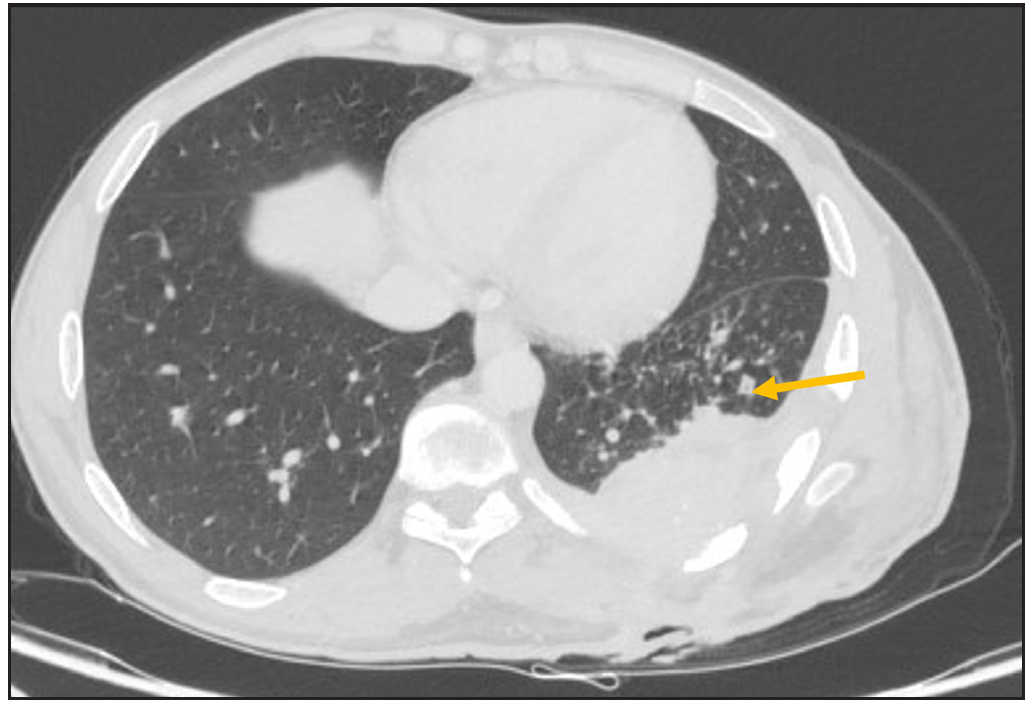
Imaging with contrast-enhanced computed tomography (CECT) of the chest showed a 4.5 cm thick, heterogeneously enhancing soft tissue swelling on the left posterolateral thoracic wall, extending intrapulmonarily into the adjacent posterior and lateral segments of the left lower lobe. Within the thorax, a central cavitating mass (3 cm × 5.4 cm) was observed with surrounding ground glass opacities and irregular spiculations radiating towards the hilum. In addition, there were ill-defined lytic lesions in the 7th to 10th ribs [Figures 3a–3d]. CECT of the abdomen was unremarkable.
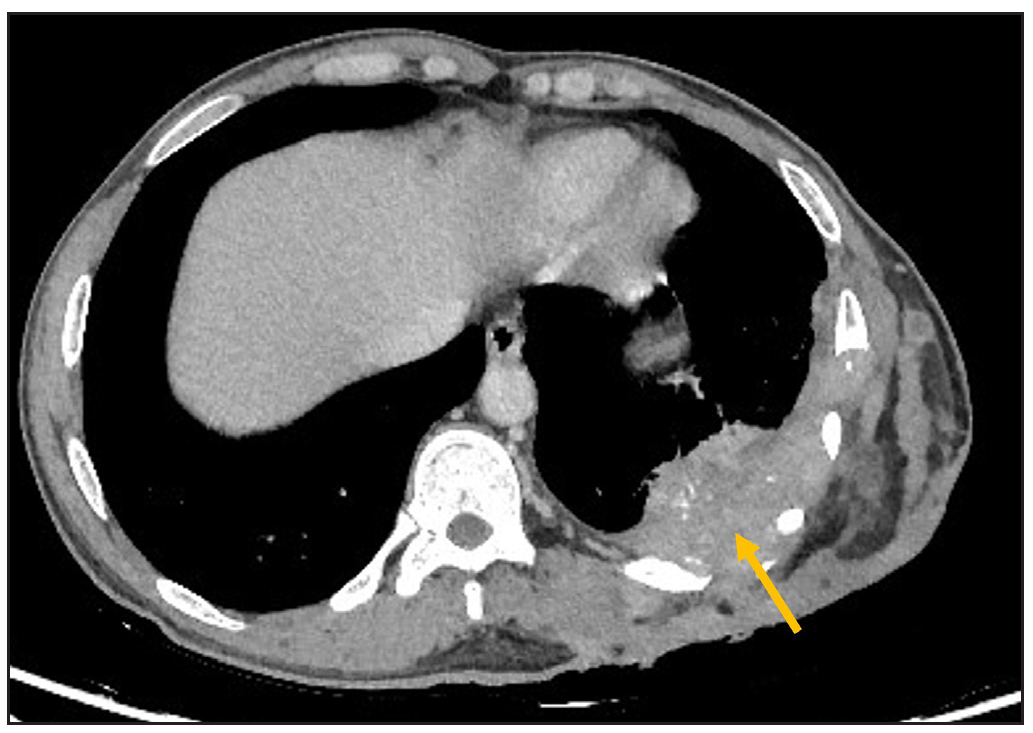
- CECT axial image depicts infiltrative enhancing soft tissue lesion (yellow arrow) in the posterolateral chest wall involving the skin, subcutaneous tissue, muscles, and having contiguous intrathoracic extension; coronal mediastinal window image.
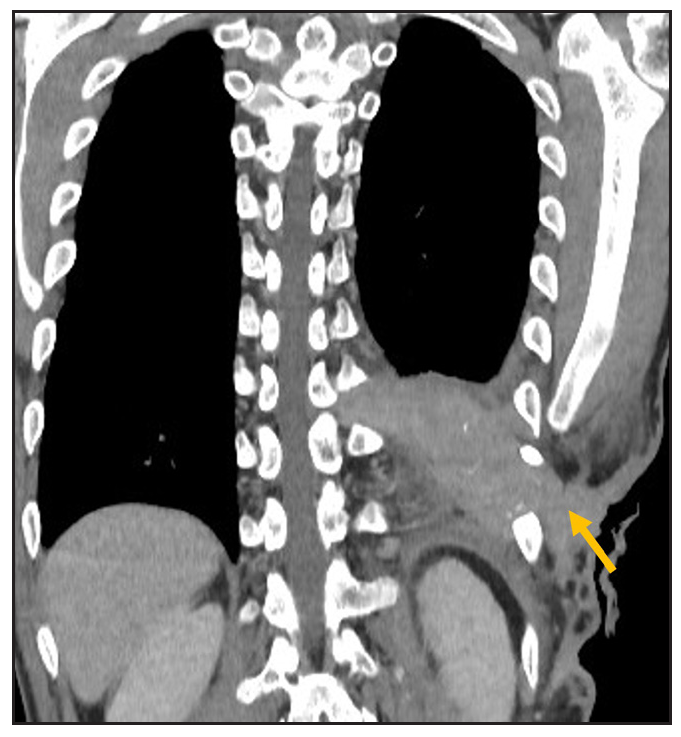
- Shows the exact extent of the lesion (yellow arrow) from the skin till the chest wall; axial lung window image.
- Shows minimal fibrotic changes (yellow arrow) in the adjacent lung; sagittal bone window image.
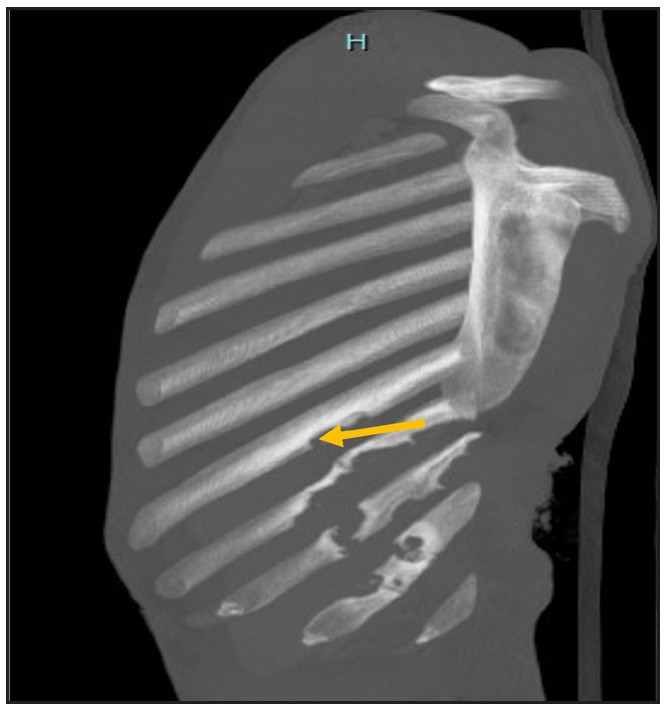
- Shows erosion (yellow arrow) and sclerosis of the underlying ribs.
The patient was diagnosed with eumycetoma of the chest with intrapulmonary extension. He was initially administered oral itraconazole 200 mg twice daily. After a month, there was a considerable reduction in the discharge and a complete resolution of cough and expectoration. However, symptoms recurred after 2 months with increased discharge, new sinuses, and cough with purulent sputum. Itraconazole was continued for 6 more months without improvement and was subsequently discontinued.
The patient was then administered voriconazole, 200 mg twice daily. By the end of the first month, the cough had completely resolved. Three months later, there was a complete resolution of discharge with resolving sinuses and healing granulation tissue [Figure 4].

- Significant improvement after 3 months of voriconazole with resolving sinuses and healing granulation tissue.
In mycetoma, the foot is the most commonly affected site, accounting for 68.7% of cases, followed by the leg (9.9%), trunk (6.1%), and arm (4.0%).1 The chest wall is a rare site, accounting for only 0.1% of 6,792 mycetoma patients seen at the Mycetoma Research Centre (MRC) between 1991 and 2014.2,3 In chest wall mycetoma, the infection typically spreads to involve the underlying muscle, bone, pleura, and even the lung parenchyma, like in our case. Though mycetoma lung secondaries have been reported from distant eumycetomas occurring on the extremities (gluteal),4 direct intrapulmonary extension is infrequent.
A 60-year old woman who had a left chest wall-eumycetoma along with a communicating broncho-pleuro-cutaneous fistula was reported at the University of Khartoum. Like in our case, she showed no signs of respiratory distress. Sinuses discharging exudative material with black grains were noted in the midaxillary line of the left chest with the discharge increasing during coughing.5 Due to a large central parenchymal cavitating mass, our patient was coughing up black grains in his sputum.
CT imaging in the above case was also similar, showing chest wall thickening, left-sided hydropneumothorax, and lower lobe collapse and consolidation of the lingual parenchyma.5 Although we were unable to culture M. mycetomatis, like in the reported case,5 the presence of spores and hyphae embedded within a brown cement-like substance and positivity on pan-fungal PCR suggested a likely diagnosis of eumycetoma.
Itraconazole is the preferred treatment for black-grain eumycetoma, though voriconazole (200 mg twice daily) or posaconazole are considered if the response is inadequate. In cases of invasive mycetomas, combining antifungals, such as azoles with terbinafine or posaconazole with flucytosine, may provide synergistic benefits.6 Given the intense inflammatory response seen in eumycetoma, the addition of anti-inflammatory drugs like diclofenac has been shown to enhance outcomes, as demonstrated in a patient with refractory disease of 20 years who responded well to a combination of posaconazole, flucytosine, and diclofenac.7 Bacterial coinfections, commonly Staphylococcus aureus, complicate treatment and the addition of antibacterial agents like amoxicillin-clavulanic acid (2 g per day) or ciprofloxacin (1 g per day) alongside antifungals has been shown to improve clinical outcomes.6 Some studies report good results with combinations like cotrimoxazole and liposomal amphotericin B, or itraconazole with trimethoprim-sulfamethoxazole, suggesting the potential activity of sulfamethoxazole-trimethoprim against the causative fungi.8 Medical treatment may be combined with surgical intervention for debridement and debulking of the infected tissue.
This case highlights an unusual presentation of eumycetoma outside the typical sites with the involvement of lung parenchyma. The patient’s clinical course, initially responsive to itraconazole, necessitating a switch to voriconazole due to disease progression, underscores the importance of continued follow-up.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Global burden of human mycetoma: A systematic review and meta-analysis. PLoS Negl Trop Dis. 2013;7:e2550.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Mycetoma caused by Madurella mycetomatis: A neglected infectious burden. Lancet Infect Dis. 2004;4:566-74.
- [CrossRef] [PubMed] [Google Scholar]
- Mycetoma: Experience of 482 cases in a single center in Mexico. PLoS Negl Trop Dis. 2014;8:e3102.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Multiple mycetoma lung secondaries from knee eumycetoma: An unusual complication. PLoS Negl Trop Dis. 2016;10:e0004735.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Broncho-pleuro-cutaneous fistula and pneumothorax: Rare challenging complications of chest wall eumycetoma. PLoS Negl Trop Dis. 2017;11:e0005737.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Madurella mycetomatis causing eumycetoma medical treatment: The challenges and prospects. PLoS Negl Trop Dis. 2020;14:e0008307.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Role of a NSAID in the apparent cure of a fungal mycetoma. J Mycol Med. 2016;26:86-93.
- [CrossRef] [PubMed] [Google Scholar]
- Mycetoma: A retrospective study of 41 cases seen in São Paulo, Brazil, from 1978 to 1989. Mycoses. 1993;36:89-95.
- [CrossRef] [PubMed] [Google Scholar]




