
Translate this page into:
Baricitinib in the management of persistent actinic granuloma: An innovative therapeutic approach
Corresponding author: Dr. Junting Tang, Department of Dermatology, The First Affiliated Hospital of Kunming Medical University, Kunming, China. ar506529014@outlook.com
-
Received: ,
Accepted: ,
How to cite this article: An R, Tang J, Lei H-X, Tu Y. Baricitinib in the management of persistent actinic granuloma: An innovative therapeutic approach. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_554_2024
Dear Editor,
Actinic Granuloma (AG) is a rare, noninfectious granulomatous disorder primarily affecting skin exposed to sunlight. It is often compared to Granuloma Annulare (GA) and is thought to be triggered by solar-damaged elastic fibers. First described by O’Brien in 1975, AG is characterised by granulomatous inflammation resulting from ultraviolet radiation-induced alterations in elastic fibers. This condition predominantly affects the skin of middle-aged individuals. Although the exact pathogenesis of AG remains unclear, current theories suggest that UV exposure may initiate a cellular immune response to altered antigenic determinants on these fibers.1 We present a case of intractable AG, whose symptoms significantly improved with treatment using the JAK1/2 inhibitor baricitinib.
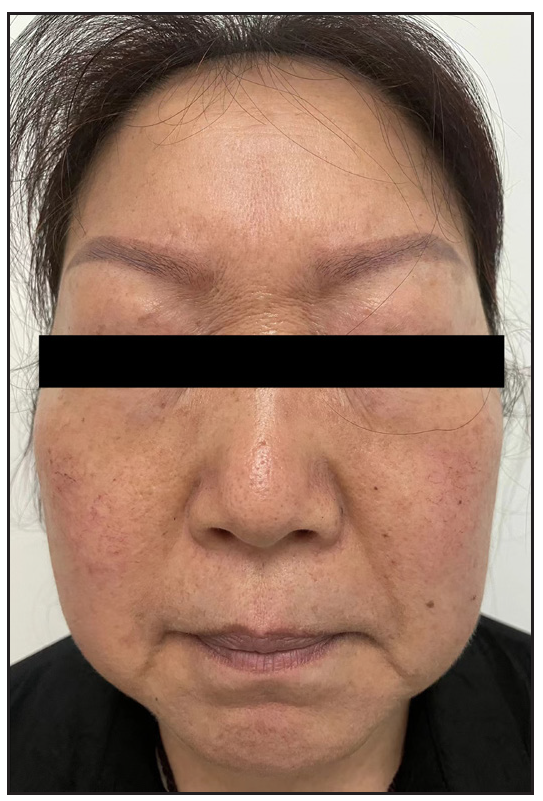
In 2023, a 57-year-old female was admitted due to a persistent two-year history of chronic erythematous and pruritic annular plaques localised on her face, neck, and upper extremities [Figures 1a-1b]. She was initially diagnosed with annular granuloma based on a histopathological evaluation from an external facility. However, treatment attempts with oral hydroxychloroquine and topical halometasone were minimally effective. Her clinical profile was noted for sun-induced dermatological disorders, with symptoms exacerbated by UV exposure. A subsequent dermatopathological examination at our centre reaffirmed the diagnosis of actinic granuloma [Figures 2a–2c]. Based on her clinical presentation and histopathological evidence, she was definitively diagnosed with AG. Although initial treatments with oral prednisolone showed limited efficacy, transitioning to baricitinib (2 mg/day) resulted in almost complete resolution of skin lesions within six weeks [Figures 3a-3b]. During a one-year follow-up, no new lesions appeared, and no adverse reactions were observed.

- Pretreatment facial lesions show scattered erythema and plaques with elevated, annular borders.

- Pretreatment lesions on the patient’s right hand reveal dense papules and plaques with annular changes.
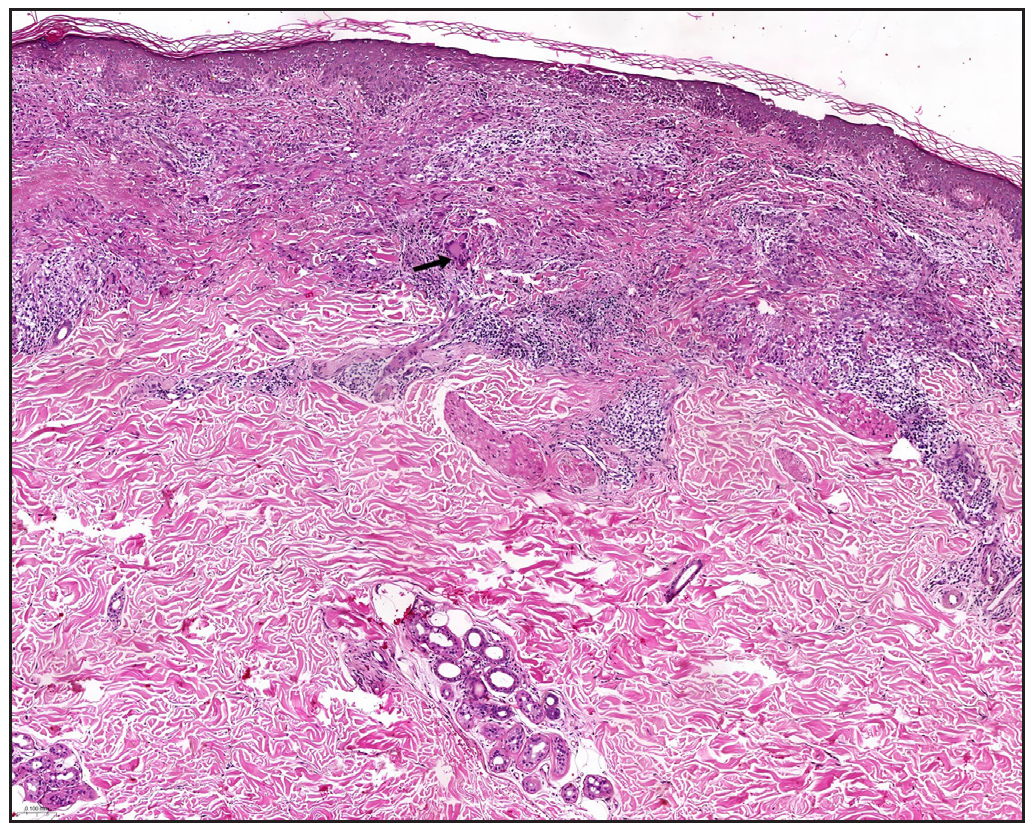
- Fencing-like granulomatous inflammation characterized by epithelioid histiocytes and multinucleated giant cells surrounding the granuloma, as indicated by the black arrows (Haematoxylin and eosin, 10x).
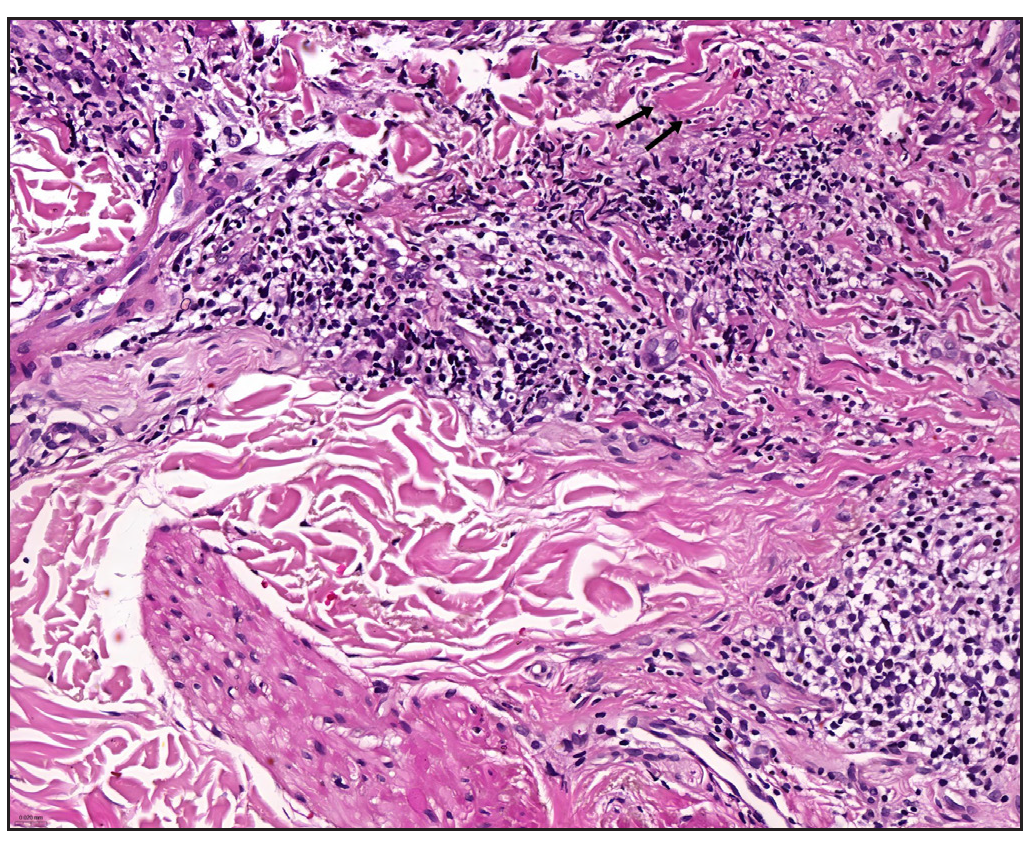
- Horizontally oriented collagen bundles appear thickened and stained red, as indicated by the black arrows (Haematoxylin and eosin, 40x).
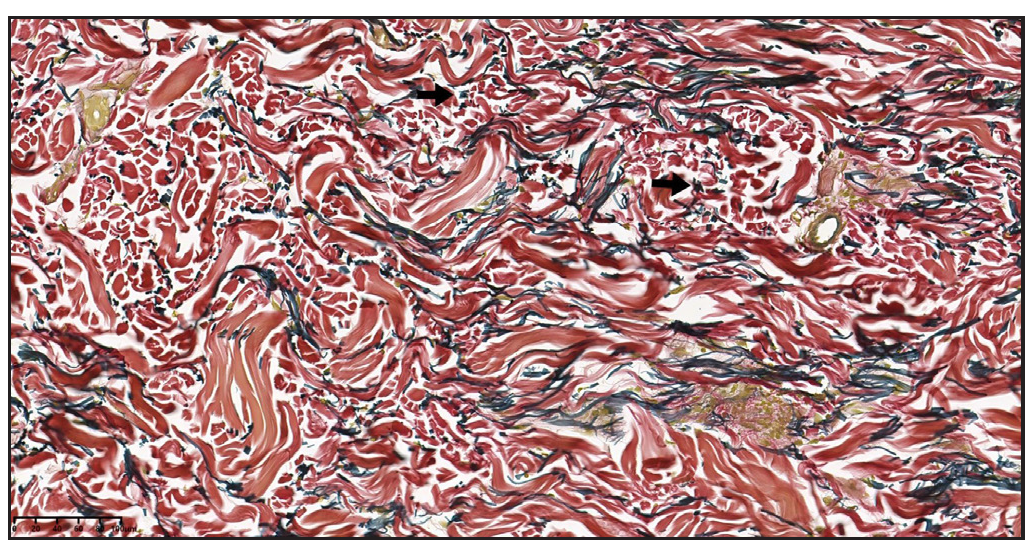
- Verhoeff-Van Gieson (VVG) staining reveals localised disruption of elastic fibres in the superficial dermis, as indicated by the black arrows. (100x)
- Post-treatment facial lesions demonstrate substantial resolution.

- Post-treatment lesions on the patient’s right hand show scattered post-inflammatory hyperpigmentation.
Actinic Granuloma (AG) tends to preferentially affect females, with epidemiological data indicating a female-to-male incidence ratio ranging from 1.2:1 to 2:1. The pathogenesis of AG remains unclear, but studies suggest that AG is a cell-mediated autoimmune response to sun-damaged elastic fibres, primarily mediated by CD4+ cells. Interferon-γ (IFN-γ) and tumour necrosis factor (TNF-α) play critical roles in this process, inducing granulomatous inflammation. Additionally, macrophages in AG express matrix metalloproteinase-12 (MMP-12), which degrades elastic fibres and is regulated by the Th-2 cytokine IL-4 in macrophages.2 Management of AG involves traditional methods such as topical and intralesional corticosteroids, psoralen plus ultraviolet A (PUVA) therapy, antimalarials, cyclosporine, methotrexate, and cryotherapy, as well as advanced laser treatments, including Pulsed Dye Laser (PDL) and fractionated CO2 laser. Additionally, the introduction of biologic agents represents a significant advancement in the treatment of granulomatous disorders. Greb, Jacqueline et al. documented the first use of adalimumab in treating AG, achieving clinical clearance with a regimen of 40 mg administered every two weeks.3 JAK inhibitors are an emerging molecular-targeted therapy for cutaneous granulomatous diseases. They work by blocking T-cell-mediated inflammation and inhibiting the JAK/STAT pathway, thereby reducing the effects of multiple cytokines and treating inflammatory diseases. McPhie et al. observed two refractory annular granuloma (GA) patients treated with tofacitinib (5 mg BID), where one patient showed rapid lesion reduction within one hour and sustained improvement after four weeks, while the other experienced nearly complete lesion resolution after nine months.4 Xiaoyuan Hou et al. treated a case of refractory GA with oral baricitinib (2 mg/day), resulting in significant rash resolution after one month and complete clearance after three months, with no new rashes observed during a six-month follow-up period.5 Similarly, Kim et al. reported the successful treatment of two patients with refractory generalised granuloma annulare using baricitinib, achieving rapid improvement.6 Baricitinib, a small molecule oral JAK inhibitor, has been shown to treat various inflammatory diseases by inhibiting the JAK-STAT signalling pathway. Bronte Vincenzo et al. found that baricitinib also reduces serum levels of TNF-α, IL-4, and IL-13 in COVID-19 patients, thereby modulating the immune environment and preventing severe disease progression. Moreover, baricitinib blocks the secretion of multiple cytokines, such as IL-4, IL-13, IL-31, TSLP, TNF-, and IFN-γ, through the MAPK, mTOR, and PI3K-Akt signalling pathways, thereby inhibiting inflammatory responses. AG is closely related to these cytokines and inflammatory pathways.7 Based on these findings, we opted to use baricitinib as our treatment method. After six weeks of baricitinib treatment, the patient’s AG symptoms significantly improved, achieving complete resolution without any adverse events or relapse. This promising outcome highlights baricitinib’s potential in AG management and underscores the need for further clinical investigation.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Actinic granuloma. An annular connective tissue disorder affecting sun- and heat-damaged (elastotic) skin. Arch Dermatol. 1975;111:460-6.
- [CrossRef] [PubMed] [Google Scholar]
- Annular elastolytic giant cell granuloma associated with prostate carcinoma: Demonstration of human metalloelastase (MMP-12) expression. Clin Exp Dermatol. 2012;37:70-2.
- [CrossRef] [PubMed] [Google Scholar]
- Adalimumab for the treatment of actinic granuloma. Dermatol Ther. 2017;30
- [CrossRef] [Google Scholar]
- Improvement of granulomatous skin conditions with tofacitinib in three patients: A case report. SAGE Open Med Case Rep. 2021;9:2050313X211039477.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- A case of granuloma annulare treated with the JAK inhibitor baricitinib. Chin J Dermatol.. 2024;57:461-2.
- [Google Scholar]
- Rapid improvement of refractory generalized granuloma annulare with the Janus kinase inhibitor baricitinib in two patients. Clin Exp Dermatol.. 2023;48:375-6.
- [CrossRef] [PubMed] [Google Scholar]
- Baricitinib restrains the immune dysregulation in patients with severe COVID-19. J Clin Invest. 2020;130:6409-16.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




