
Translate this page into:
Treatment of auricular chondritis with tofacitinib

Corresponding author: Dr. Zhongxiang Shi, Dermatology Hospital of Shandong First Medical University, Jinan, Shandong, China. szxsd2003@sina.com
-
Received: ,
Accepted: ,
How to cite this article: Zhao X, Chen S, Liu H, Shi Z. Treatment of auricular chondritis with tofacitinib. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_44_2025
Dear Editor,
Auricular chondritis is a condition of unknown aetiology, commonly associated with relapsing polychondritis, where it represents the hallmark clinical manifestation. It is estimated that up to 90% of patients with relapsing polychondritis experience auricular chondritis during the disease.1 The condition typically results in redness and swelling of the external ear but does not involve the earlobe. A characteristic presentation includes painful, red, and swollen auricles. Recurrent episodes can lead to permanent cartilage destruction, resulting in a deformity known as the “cauliflower ear”.2 Additionally, repeated inflammation may cause dystrophic calcification of the ear cartilage, producing what is described as the “porcelain ear”.2
A 23-year-old male patient presented with a one-year history of recurrent left auricle swelling, accompanied by dark red infiltrative plaques, mild tenderness, and itching [Figure 1a, 1b, and 1c]. Previous treatment with various topical medications yielded minimal improvement. His medical history included allergic rhinitis. A dermatological examination revealed a swollen left auricle with a dark red infiltrative plaque and mild tenderness. The skin of the external ear and ear canal appeared normal, with no pain on traction. The nasal cartilage and trachea showed no collapse or deformity. No redness, swelling, or deformities were observed in the bones and joints throughout the body. Laboratory tests revealed decreased apolipoprotein A levels (10.97↓) and a negative ANA titre. The diagnosis of auricular chondritis was established based on clinical and pathological findings. After obtaining informed consent and ruling out contraindications, the patient was started on oral tofacitinib citrate tablets (5 mg bid), with monthly follow-ups. After one month of treatment, the swelling and pain were alleviated, and no adverse effects were reported [Figure 1d, 1e, and 1f]. Six months later, the swelling of the left auricle had largely subsided, and the shape of the auricle had returned to normal [Figure 1g, 1h, and 1i]. The diagnosis of the auricular chondritis was confirmed on histopathological examination of left ear tissue [Figure 2a and 2b].
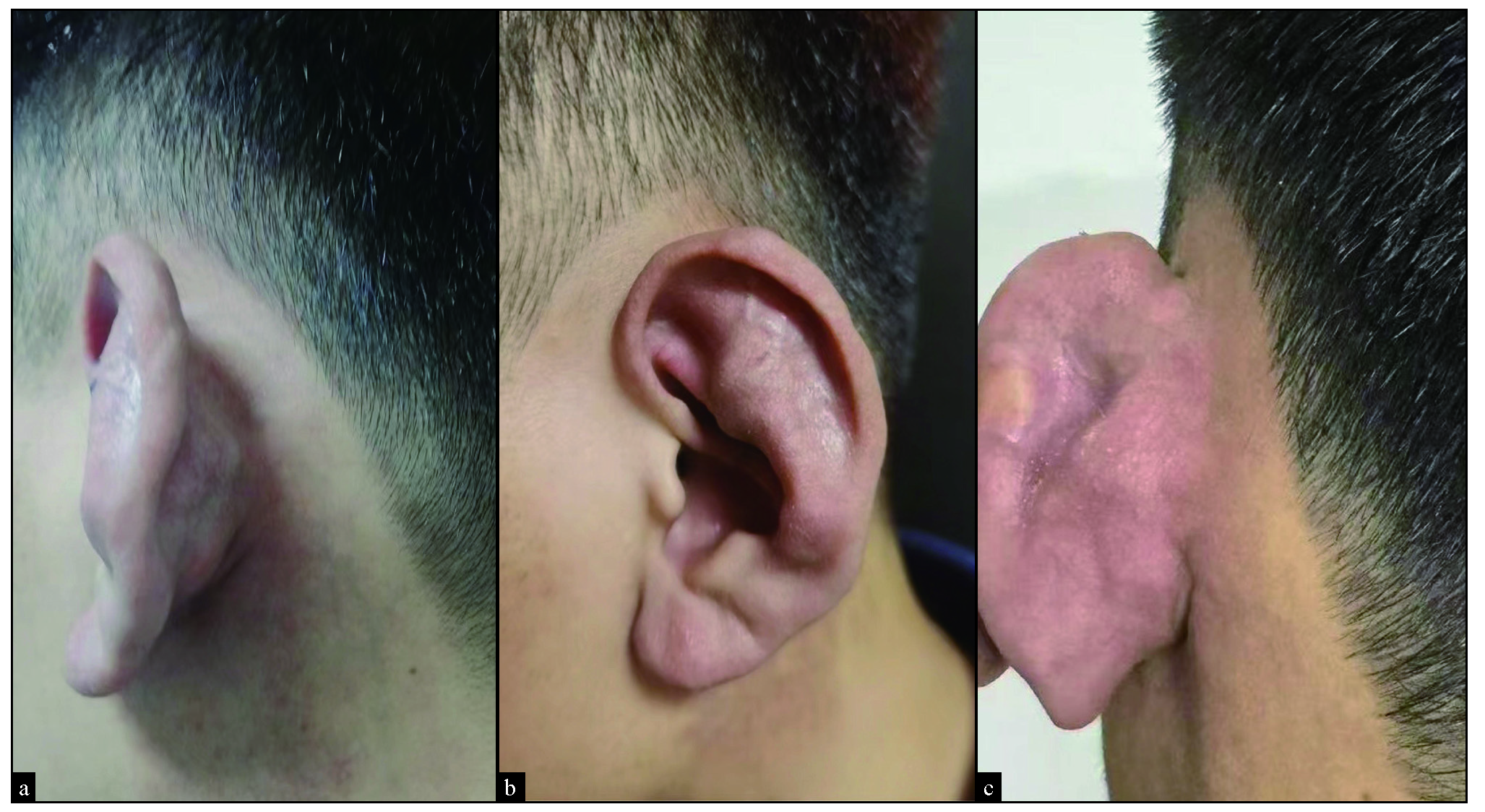
- Initial physical examination revealed left auricle swelling, accompanied by dark red infiltrative plaques, mild tenderness, and pruritus.

- At the one-month after treatment, swelling significantly had reduced with fading of the red infiltrative plaques and no tenderness.

- At the six-month follow-up; complete resolution of all signs and symptoms.

- (a) (left ear) Some chondrocytes exhibit eosinophilic degeneration, with a few lymphocytes infiltrating the surrounding area. Additionally, there is collagen proliferation in the subcutaneous dermal layer, accompanied by lymphocyte infiltration (Haematoxylin-eosin 40x), (b) (left ear) Some chondrocytes exhibit eosinophilic degeneration, with a few lymphocytes infiltrating the surrounding area. Additionally, there is collagen proliferation in the subcutaneous dermal layer, accompanied by lymphocyte infiltration (Haematoxylin-eosin 100x).
In this case, the patient presented with swelling of the left auricle, accompanied by dark red infiltrative plaques and mild tenderness, with pathology confirming auricular chondritis. However, no signs of involvement of other cartilaginous structures, such as joint pain, nasal swelling, ocular discomfort, visual impairment, or respiratory distress, were observed upon examination. The ANA titre was negative, and the patient did not meet the diagnostic criteria for RP. Auricular chondritis, often acute, may involve one or both ears alternately.2 Close follow-up with rheumatology referral for systemic treatment is required if symptoms develop. Auricular chondritis lacks a standardised treatment. Common therapies include NSAIDs (aspirin), glucocorticoids, DMARDs (methotrexate and cyclophosphamide), and biologics.3 relapsing polychondritis pathogenesis is characterised by JAK-STAT/NF-κB axis hyperactivation, Th17 cell-mediated overproduction of IL-17/IL-6 cytokines, and matrix metalloproteinase (MMP)-induced cartilage destruction.2 Tofacitinib, a selective JAK1/3 inhibitor, suppresses pathogenic cytokine cascades by attenuating STAT phosphorylation,4 concurrently inhibiting Th17 lineage differentiation. Emerging clinical evidence- including documented laryngeal chondritis resolution5 and rheumatoid arthritis trial data6 confirms its dual therapeutic modality: interleukin-6(IL-6)/JAK-STAT axis blockade and cartilage-protective immunoregulation. In terms of safety, long-term use of tofacitinib is associated with an increased risk of cardiovascular diseases and malignancies.7 However, in our case, the patient was a young male with no family history of cardiovascular diseases or cancer. Given the short treatment duration and strict monitoring regimen, the therapy demonstrated a favourable safety profile. This mechanistically grounded intervention was prioritised over conventional therapies due to relapsing polychondritis -specific signalling modulation, offering a rational therapeutic paradigm that warrants further studies.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Relapsing polychondritis: Best practice & clinical rheumatology. Best Pract Res Clin Rheumatol. 2023;37:101867.
- [CrossRef] [PubMed] [Google Scholar]
- Relapsing polychondritis: Clinical updates and new differential diagnoses. Nat Rev Rheumatol. 2024;20:347-60.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Unveiling the clinical spectrum of relapsing polychondritis: Insights into its pathogenesis, novel monogenic causes, and therapeutic strategies. Adv Rheumatol. 2024;64:29.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Histological outcomes and JAK-STAT signalling in ulcerative Colitis patients treated with tofacitinib. J Crohns Colitis.. 2024;18:1283-1291.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Tofacitinib in steroid-dependent relapsing polychondritis. Ann Rheum Dis. 2019;78:e72.
- [CrossRef] [PubMed] [Google Scholar]
- Comparative effectiveness of adalimumab vs tofacitinib in patients with rheumatoid arthritis in Australia. JAMA Netw Open. 2023;6:e2320851.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Cardiovascular and cancer risk with tofacitinib in rheumatoid arthritis. N Engl J Med. 2022;386:316-2.
- [CrossRef] [PubMed] [Google Scholar]




