Translate this page into:
Comparison of efficacy of platelet-rich plasma therapy with or without topical 5% minoxidil in male-type baldness: A randomized, double-blind placebo control trial
Correspondence Address:
Satyendra Kumar Singh
Department of Dermatology and Venereology, Institute of Medical Sciences, Banaras Hindu University, Varanasi - 221 005, Uttar Pradesh
India
| How to cite this article: Singh SK, Kumar V, Rai T. Comparison of efficacy of platelet-rich plasma therapy with or without topical 5% minoxidil in male-type baldness: A randomized, double-blind placebo control trial. Indian J Dermatol Venereol Leprol 2020;86:150-157 |
Abstract
Background: Male-type baldness is a common chronic hair loss disorder among males. Male type baldness is characterized by stepwise miniaturization of the hair follicle, due to alteration in the hair cycle dynamics, leading to transformation of the terminal hair follicle into a vellus one. Platelet-rich plasma (PRP) seems to be a new technique which may improve hair regrowth. We planned a randomized, double-blinded placebo control trial to see the efficacy of PRP with and without topical minoxidil and to compare with placebo and standard treatment.
Materials and Methods: The study design was a randomized, double-blind placebo control trial. The sample size was calculated, and randomization was done. Patients with male type baldness were allocated into four groups; first group topical minoxidil only, the second group PRP with minoxidil, the third group normal saline (NS), and fourth group PRP only. Interventions were done monthly for 3 months and patients were followed up for the next 2 months. Effects of interventions were assessed by hair density, patient self-assessment, and clinical photography.
Results: A total of 80 patients were included. The maximum improvement was found in PRP with minoxidil group. Increase in hair density (in descending order) was PRP with minoxidil group, PRP-alone group, minoxidil-alone group, while a decrease in hair density was found in NS group, after 5 months. The maximum patient satisfaction was found in PRP with minoxidil group followed by (in descending order), PRP-alone group, minoxidil-alone group, and NS group.
Limitation: Long-term follow up of patients was not done. Hair counts and hair thickness estimation were not estimated.
Conclusion: In our study, we found PRP with topical minoxidil is more effective than PRP alone and topical minoxidil alone.
Introduction
Hair loss results in low self-esteem due to a perceived decrease in personal attractiveness, and is an important feature of low self-image. A significant impairment in quality of life is seen equally in males and females suffering from androgenetic alopecia (AGA), which is known to affect greater than 50% of men over 50 years of age and can also affect females.[1],[2],[3] The Food and Drug Administration (FDA)–approved treatments for AGA are topical minoxidil and oral finasteride.[4] Minoxidil acts by promoting enhanced dermal vascularity, and has antiapoptotic, and mitogenic effects.[5],[6],[7] Finasteride, on the other hand, blocks 5α-reductase, reduces levels of dihydrotestosterone, and prolongs anagen, leading to thickening of miniaturized hairs and increasing hair counts.[8],[9] Dutasteride is another non-FDA-approved treatment for AGA. As the follicles have increased vascularity and vascular endothelial growth factor (VEGF) receptor during anagen phase, VEGF binds more effectively to dermal papillary cells in the anagen phase and hair loss treatments can be directed toward induction of anagen, prolongation of anagen, or inhibition of exogen.[6]
Platelet-rich plasma (PRP) is a three to eight times platelet-enhanced product of plasma. Platelets contain a variety of growth factors including transforming growth factor-β, VEGF, platelet-derived growth factor, insulin-like growth factor, and epithelial growth factor.[10],[11] PRP has been used in the treatment of AGA in the dermatological field, orthodontic conditions, chronic and refractory ulcers, injuries in orthopedics, and sports medicine as well as in neurological problems.
We were unable to find any previous study comparing four arms of PRP alone, topical minoxidil alone, PRP with topical minoxidil, and normal saline (NS).
Hence, we planned a randomized, double-blinded placebo controlled trial to see the efficacy of PRP with and without topical minoxidil and to compare with placebo and standard treatment.
Materials and Methods
Trial design
We conducted a single-center, prospective, randomized, double-blind control trial with four parallel arms. Informed written consent was taken from each patient participating in the study. Institution Ethics Committee approval was taken for the protocol submitted, after which the study was registered with the Clinical Trials Registry of India. Inclusion criteria were patients with male-type baldness of Hamilton–Norwood scale II–V within the age group of 18–60 years, not using topical minoxidil and oral or topical finasteride for at least 6 months and willing to come for regular follow-up.
Exclusion criteria were uncooperative patients and those having any inflammation or erythema (except mild seborrheic dermatitis), or scarring over the scalp. Patients taking anticoagulants, antihypertensives, anticonvulsants, aspirin, or other nonsteroidal anti-inflammatory drugs were excluded. Patients with or having previous history of malignancies, platelet or bleeding disorders, bone marrow aplasia, diabetes, HIV, hepatitis B or C infection or otherwise immunocompromised, and those having a propensity for keloids were also excluded.
The trial was conducted in dermatology outpatient department at Sir Sunderlal Hospital, Institute of Medical Sciences, Banaras Hindu University, Varanasi, on patients having male type baldness during the study period from February 2017 to February 2018.
Diagnosis of male type baldness
The diagnosis of male type baldness was established by a detailed medical history of diffuse hair loss, after ruling out any drug intake which could cause hair loss, and dermoscopic features (miniaturization and more than 20% variability in hair diameter between affected and uninvolved areas). Grading was done according to Hamilton–Norwood scale.
Baseline investigations were done including complete blood cell count, liver function tests, renal function tests, T3, T4, TSH, plasma glucose fasting, and postprandial; HbA1C, ELISA for HIV I and II, RPR test in dilution, anti-HBsAg, and anti HCV antibody.
Cases were randomized into four groups:
- Group I (Minoxidil): Minoxidil solution 5% topically 1 mL on dry scalp two times a day (12 hourly) was applied throughout the study period with intradermal (placebo) injection of NS monthly for 3 months.
- Group II (PRP with minoxidil): Minoxidil solution 5% topically 1 mL over dry scalp two times a day was applied throughout the study period with intradermal injection of PRP monthly for 3 months.
- Group III (NS): Topical placebo containing (58 mL of NS and 2 mL spirit) topically 1 mL over dry scalp two times a day was applied throughout the study period with intradermal (placebo) injection of NS monthly for 3 months.
- Group IV (PRP): Topical placebo containing (58 mL of NS and 2 mL spirit) topically 1 mL over dry scalp two times a day was applied throughout the study period with intradermal injection of PRP monthly for 3 months.
PRP preparation
A total of 18 ml of fresh whole blood was collected and mixed with 2 ml of 3.8% sodium citrate solution into an autoclaved Falcon tube under proper aseptic precautions. The tube was rotated in a centrifugation machine (Remi model R-8M) at 2200 revolutions per minute for 12 min. The “ first spin” allows blood separation into three layers, namely, bottom red blood cell layer, topmost acellular plasma layer called platelet-poor plasma (PPP), and an intermediate PRP layer called the “buffy coat.” The buffy coat along with plasma was collected with the help of Finnpipette into another Falcon tube. The “second spin” was done at 3000 revolutions per minute for 6 min. This allowed the platelets (PRP) to settle at the bottom of the tube. The upper two-third containing PPP was discarded, and the lower one-third of PRP was loaded in 1 mL BD syringe containing calcium gluconate (one part calcium gluconate 10% and nine parts of PRP) as an activator. By this method, we obtained 3–3.5 mL of PRP having a platelet concentration of 4.2 fold when compared with the whole blood. Platelet concentration in PRP was determined in the first 10 patients for standardization of procedure.
Topical anaesthetic cream was applied over the target area 1 h before administration of PRP. Areas to be treated (frontal, parietal, and vertex) were cleaned with 70% alcohol. PRP (0.05–0.1 mL/cm2) was injected intradermally by 1 mL Beckton Dickinson syringe in a retrograde fashion from deep to superficial, at a distance of 1 cm. Injection of PRP was given three times in each patient at intervals of 1 month. NS (placebo) was injected in a similar method.
Vital signs and adverse events reported by the patient or elicited by the clinician were assessed at each follow-up.
Patient assessment
All patients were evaluated in six stages: BT, before treatment; F1, at 1 month of follow-up; F2, at 2 months of follow-up; F3, at 3 months of follow-up; F4, at 4 months of follow-up; and F5, at 5 months of follow-up (total 5 months of study). The effect of the treatment was assessed by hair density, patient self-assessment, and clinical photography documented every month for 5 months.
The primary outcome of the study was done through assessment of improvement in hair density. The secondary outcome of the study was through a patient self-assessment score.
Assessment of improvement in hair density was done by dermoscopic pictures taken at a fixed site in a 1-cm2 area. Assessment area was fixed, that is, 10 cm above and 3 cm front from the upper end of the right tragus. A stamp of 1 × 1 cm was used to fix the area, and every month dermoscopic pictures were taken from this area.
Patient self-assessment score
Patients assessed their scalp hair on hair growth assessment scale of 0–4:
- 0: no improvement
- 1: 1%–25% improvement
- 2: 26%–50% improvement
- 3: 51%–75% improvement
- 4: 76%–100% improvement
Clinical photographs were taken at every session from the front, vertex, and lateral views of both the sides.
Sample size calculation
Sample size (n) = ( Z1−α+Z1−β) 2 SD2/d2
Z1−α=1.645.
Z1−β=1.28.
SD2 = SD12 + SD22-2r SD1 SD2.
where r = 0.50 (relationship between observation value at baseline and last follow-up, i.e. 5 months), d = difference between baseline and after 5 months of follow-up. It is taken as minimum improvement of 5%, that is, 5.6 (5% of 112),[12] standard deviation = 6, and sample size = 15.
Z1−α= Value from the standard normal distribution holding 1−α below it
Z1−β= Value from the standard normal distribution holding 1− β below it
α= Type I error
β = Type II error
Further assuming 20% loss to follow-up during treatment, n = 18.75 ≈ 19, that is, taken as 20 (95% confidence level, 90% power).
Randomization
The allocation sequence was generated using online randomization generator using website www.randomizer.org and concealed by a person unrelated to the trial management group. Only one person who was introducing the drugs had knowledge about the randomization of the subject. Patient, evaluator, and analyzer had no knowledge regarding the randomization group.
Statistical analysis
The data obtained were analyzed by SPSS 17.0 trial version. The data were presented in terms of means, standard deviation, and percentages. To assess the association between categorical variable, “Chi-square test” was used as per suitability, and to find out the effect of intervention after uninterrupted completion of 5 months' treatment, paired t-test and analysis of variance were used. P value less than 0.05 was taken as statistical significance.
Effectiveness analysis was done on a modified intention-to-treat basis with cases reporting for at least one post-baseline follow-up visit. Missing values were dealt with the last observation carried forward strategy.
Results
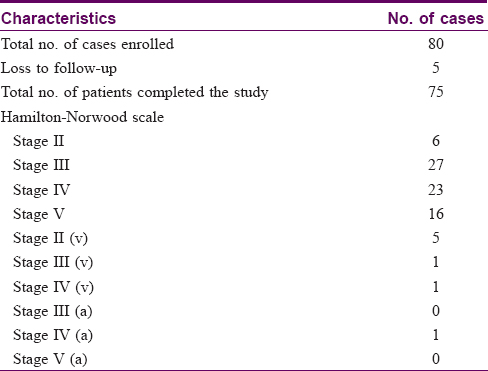
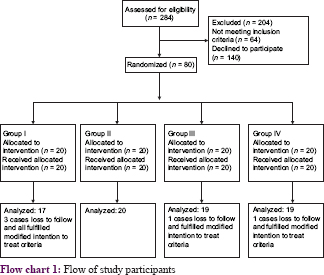
A total of 284 patients were assessed, and finally 80 cases were included and randomized for further study [Flow chart 1]. Patient characteristics are given in [Table - 1]. Five patients refused to continue the treatment protocol due to pain and discomfort during intervention.
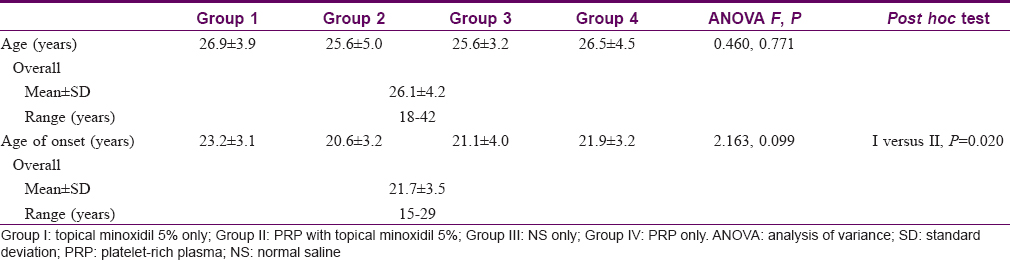
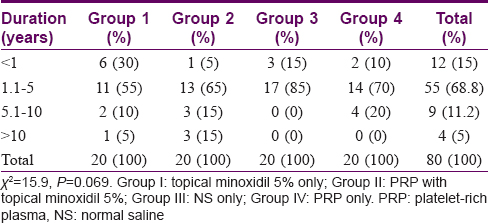
Age distribution and age of onset in different groups are given in [Table - 2]. There was no statistically significant difference in age distribution and onset among the four groups (P = 0.771 and P = 0.099, respectively). Duration of male type baldness in a majority of cases was from 1.1 to 5 years [Table - 3].
The effect of different interventions on hair density was assessed every month for 5 months. Intragroup and intergroup comparison was done [Table - 4] and [Graph 1]. In intragroup comparison, a highly significant increase in hair density was achieved after 3 months of treatment in group I (P< 0.001); a highly significant increase was achieved after 1 month in groups II and IV (P< 0.0.01); while in group III there was worsening after 5 months.
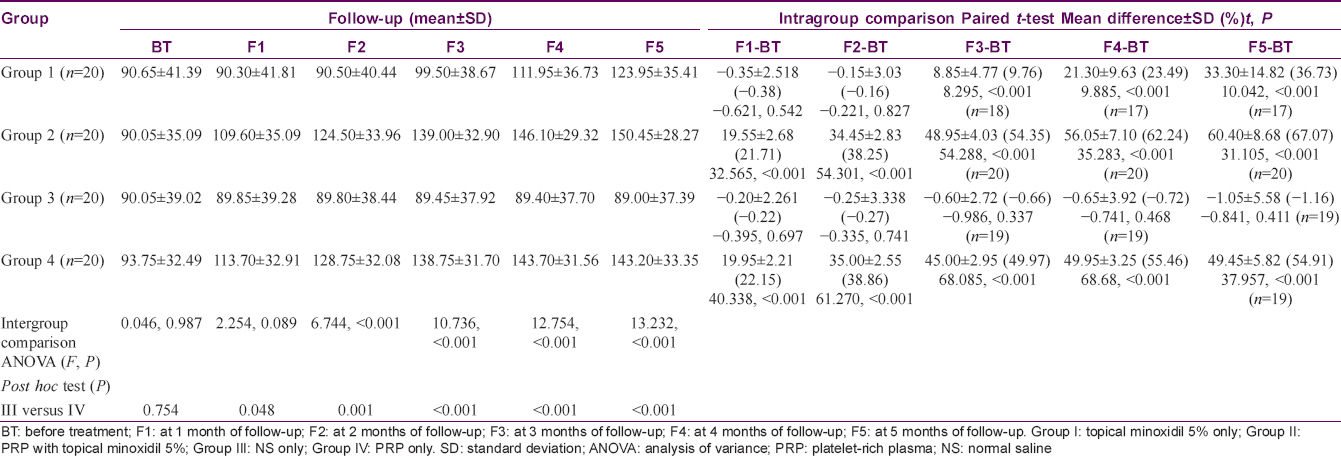
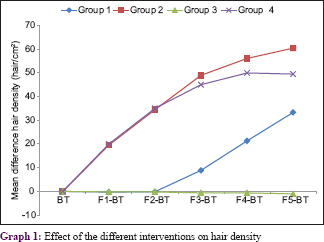
There was no significant difference between the groups before treatment in intergroup comparison. At the end of the study, there was a significant difference found between groups I and II, and groups I and III (P = 0.0 15 and 0.002, respectively). A highly significant difference was found in group II vs. group III and group III vs. group IV (P< 0.001), whereas there was no significant difference in group I vs. group IV and group II vs. group IV (P = 0.076 and 0.499, respectively). Maximum improvement in hair density was found in group II followed by groups IV and I, whereas worsening was found in group III.
Clinical images of scalp before treatment and after 5 months of groups I, II, III, and IV are shown in [Figure - 1] respectively.
 |
| Figure 1: |
Improvement in patient's satisfaction was found to be maximum in group II followed by group IV and group I, whereas none of the patients were satisfied in group III [Table - 5].

Various adverse effects were noted during the study period in different interventions. There was no major adverse effect seen in any group [Table - 6].

Discussion
Male type baldness not only affects the beauty but also results in lower self-esteem, sadness, depression, stress, and impaired quality of life.[3],[13] These problems are more pronounced in younger patients with more advanced disease. Therefore, there is a tangible need to develop an efficient treatment modality. Various topical and oral medications have been introduced for treating this condition. Among them, only topical minoxidil and oral finasteride have been approved by the FDA.[4] Efficacy of these medications is low and only lasts as long as they are used. We were unable to find any previous study comparing four arms of PRP alone, topical minoxidil alone, PRP with topical minoxidil, and NS. We conducted a double-blind, randomized placebo control trial, enrolling 80 cases. In a previous reported study by Schiavone et al., the largest sample size was 64.[14] Improvement in hair density was seen in three groups (minoxidil group, PRP with minoxidil group, and PRP group). Maximum improvement was found in PRP with minoxidil group. In a study conducted by Takikawa et al.[12] on 13 patients with AGA, 15 mL of fresh blood was taken and using double-spin method centrifugation at 1700 RPM for 15 min followed by 3000 RPM for 5 min to achieve 3 mL of PRP, which had platelet concentration of six times when compared with whole blood.[12] Activator was not mentioned in the given study. The outcome of that study showed that PRP and NS injection did not increase the number of hairs in patients, but it only increased the hair thickness. There was no increase in the number of hairs which may be due to non-addition of activator. The authors suggested that adding a carrier to PRP could increase PRP effect.[12]
Moreover, in Takikawaet al.'s study, the PRP injection was given every 2–3 weeks for five sessions, and it included both genders, with no report on the severity of their AGA. In our study, we gave three injections 1 month apart and only men with Hamilton–Norwood scale II–V were included. A few other studies have also used the double-spin method and found significant improvement in hair density (hairs/cm2).[15],[16],[17] In Guptaet al.'s study, after 6 sessions of PRP with a gap of 15 days, there was increase in hair density, hair diameter and independent observer clinical evaluation with mean difference ± standard deviation of 39.7 ± 16.5%, 39.8 ± 17.2% and 30.2 ± 12.2% respectively compared with baseline.[16] In Khatu et al.'s study, increase in follicular units per cm2 was 22.09 and patient satisfaction score was 7 out of 10 score.[17]
In our study, maximum improvement in patient self-assessment at the end of the study was found in PRP with minoxidil group followed by the PRP alone group and minoxidil alone group, whereas none of the patients were satisfied in the NS group. A few other studies have been reported where PRP alone also found similar results in patient satisfaction improvement.17-19 Two studies by Mapar et al.[20] and Puig et al.[21] demonstrated that PRP was not effective in treating AGA. In the former study, patient self-assessment was not done and clinician examination was performed by using magnifying glass to assess outcomes.[20] In the study by Puig et al., only one treatment was administered and PRP was not activated. 21 Significant improvement using objective measures was not detected, but they did document subjective improvement.[21]
In our study, temporary pain was encountered by patients in all cases after PRP treatment, while scalp pruritus, increased facial hair, and hyperpigmentation were found in some patients treated with topical minoxidil. There were no major adverse effects reported in other studies also. A systematic review by Picard et al. shows that the use of PRP injections in patients with AGA seems effective in promoting lost hair regrowth, decreasing hair loss, and increasing hair thickness.[22]
This study strengthens the evidence on the effect of PRP on AGA.
Limitations
Long-term follow-up of cases was not done Hair counts were not done over different parts of the scalp, nor were measurement of hair thickness and vellus hair counts. The effects of treatment on anagen and telogen hair were not observed.
Conclusion
PRP with topical minoxidil was the most effective treatment modality while PRP alone and topical minoxidil alone were more effective than placebo. There was no significant difference between PRP alone and topical minoxidil alone, but the effect of PRP was seen earlier than topical minoxidil. Overall, our study shows that PRP is an effective and safe method for male pattern baldness. It may be reconfirmed by further studies with a larger sample size.
Registration: Clinical Trial Registry – India (CTRI) number for the trial was CTRI/2018/05/014113.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
This study was financially supported by the Institutional Research Grant.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Alfonso M, Richter-Appelt H, Tosti A, Viera MS, García M. The psychosocial impact of hair loss among men: A multinational European study. Curr Med Res Opin 2005;21:1829-36.
[Google Scholar]
|
| 2. |
Leavitt M. Understanding and management of female pattern alopecia. Facial Plast Surg 2008;24:414-27.
[Google Scholar]
|
| 3. |
Cash TF. The psychological effects of androgenetic alopecia in men. J Am Acad Dermatol 1992;26:926-31.
[Google Scholar]
|
| 4. |
Sinclair R. Male pattern androgenetic alopecia. BMJ 1998;317:865-9.
[Google Scholar]
|
| 5. |
Mecklenburg L, Tobin DJ, Müller-Röver S, Handjiski B, Wendt G, Peters EM, et al. Active hair growth (anagen) is associated with angiogenesis. J Invest Dermatol 2000;114:909-16.
[Google Scholar]
|
| 6. |
Kozlowska U, Blume-Peytavi U, Kodelja V, Sommer C, Goerdt S, Majewski S, et al. Expression of vascular endothelial growth factor (VEGF) in various compartments of the human hair follicle. Arch Dermatol Res 1998;290:661-8.
[Google Scholar]
|
| 7. |
Han JH, Kwon OS, Chung JH, Cho KH, Eun HC, Kim KH. Effect of minoxidil on proliferation and apoptosis in dermal papilla cells of human hair follicle. J Dermatol Sci 2004;34:91-8.
[Google Scholar]
|
| 8. |
Tosti A, Piraccini BM. Finasteride and the hair cycle. J Am Acad Dermatol 2000;42:848-9.
[Google Scholar]
|
| 9. |
Kang JS, Zheng Z, Choi MJ, Lee SH, Kim DY, Cho SB. The effect of CD34+ cell-containing autologous platelet-rich plasma injection on pattern hair loss: A preliminary study. J Eur Acad Dermatol Venereol 2014;28:72-9.
[Google Scholar]
|
| 10. |
Tavakkol A, Elder JT, Griffiths CE, Cooper KD, Talwar H, Fisher GJ, et al. Expression of growth hormone receptor, insulin-like growth factor 1 (IGF-1) and IGF-1 receptor mRNA and proteins in human skin. J Invest Dermatol 1992;99:343-9.
[Google Scholar]
|
| 11. |
Arshdeep, Kumaran MS. Platelet-rich plasma in dermatology: Boon or a bane? Indian J Dermatol Venereol Leprol 2014;80:5-14.
[Google Scholar]
|
| 12. |
Takikawa M, Nakamura S, Nakamura S, Ishirara M, Kishimoto S, Sasaki K, et al. Enhanced effect of platelet-rich plasma containing a new carrier on hair growth. Dermatol Surg 2011;37:1721-9.
[Google Scholar]
|
| 13. |
Williamson D, Gonzalez M, Finlay AY. The effect of hair loss on quality of life. J Eur Acad Dermatol Venereol 2001;15:137-9.
[Google Scholar]
|
| 14. |
Schiavone G, Raskovic D, Greco J, Abeni D. Platelet-rich plasma for androgenetic alopecia: A pilot study. Dermatol Surg 2014;40:1010-9.
[Google Scholar]
|
| 15. |
Singhal P, Agarwal S, Dhot PS, Sayal SK. Efficacy of platelet-rich plasma in treatment of androgenic alopecia. Asian J Transfus Sci 2015;9:159-62.
[Google Scholar]
|
| 16. |
Gupta S, Revathi TN, Sacchidanand S, Nataraj HV. A study of the efficacy of platelet-rich plasma in the treatment of androgenetic alopecia in males. Indian J Dermatol Venereol Leprol 2017;83:412.
[Google Scholar]
|
| 17. |
Khatu SS, More YE, Gokhale NR, Chavhan DC, Bendsure N. Platelet-rich plasma in androgenic alopecia: Myth or an effective tool. J Cutan Aesthet Surg 2014;7:107-10.
[Google Scholar]
|
| 18. |
Gkini MA, Kouskoukis AE, Tripsianis G, Rigopoulos D, Kouskoukis K. Study of platelet-rich plasma injections in the treatment of androgenetic alopecia through an one-year period. J Cutan Aesthet Surg 2014;7:213-9.
[Google Scholar]
|
| 19. |
Betsi EE, Germain E, Kalbermatten DF, Tremp M, Emmenegger V. Platelet-rich plasma injection is effective and safe for the treatment of alopecia. Eur J Plast Surg 2013;36:407-12.
[Google Scholar]
|
| 20. |
Mapar MA, Shahriari S, Haghighizadeh MH. Efficacy of platelet-rich plasma in the treatment of androgenetic (male-patterned) alopecia: A pilot randomized controlled trial. J Cosmet Laser Ther 2016;18:452-5.
[Google Scholar]
|
| 21. |
Puig CJ, Reese R, Peters M. Double-blind, placebo-controlled pilot study on the use of platelet-rich plasma in women with female androgenetic alopecia. Dermatol Surg 2016;42:1243-7.
[Google Scholar]
|
| 22. |
Picard F, Hersant B, Niddam J, Meningaud JP. Injections of platelet-rich plasma for androgenic alopecia: A systematic review. J Stomatol Oral Maxillofac Surg 2017;118:291-7.
[Google Scholar]
|
Fulltext Views
31,866
PDF downloads
5,270





![[Table - 1]](#tbl_ijdvl_2020_86_2_150_272397_t2.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2020_86_2_150_272397_t3.jpg){kind=link}
![[Table - 3]](#tbl_ijdvl_2020_86_2_150_272397_t4.jpg){kind=link}
![[Table - 4]](#tbl_ijdvl_2020_86_2_150_272397_t5.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2020_86_2_150_272397_f1.jpg){kind=link}
![[Table - 5]](#tbl_ijdvl_2020_86_2_150_272397_t6.jpg){kind=link}
![[Table - 6]](#tbl_ijdvl_2020_86_2_150_272397_t7.jpg){kind=link}