Translate this page into:
Synovial sarcoma complicating Maffucci syndrome
Correspondence Address:
Rima Gammoudi
Department of Dermatology, Farhat Hached University Hospital, 4002 Ibn Jazzar Avenue, Sousse
Tunisia
| How to cite this article: Gammoudi R, Aounallah A, Belajouza C, Nouira R. Synovial sarcoma complicating Maffucci syndrome. Indian J Dermatol Venereol Leprol 2019;85:291-294 |
Abstract
Maffucci syndrome is a rare nonhereditary disorder comprising of lymphovascular malformations and multiple enchondromas, which may be associated with several internal malignancies. This report describes a new association of Maffucci syndrome with pedal synovial sarcoma. Our case is also remarkable as lymphangioma circumscriptum is the sole lymphovascular component, which has been rarely reported. The aim of this report is to generate awareness about this rare condition and also highlight the importance of screening for malignancies in this disorder.
Introduction
Enchondromatosis is a group of rare and nonhereditary disorder in which patients develop multiple enchondromas; Maffucci syndrome and Ollier's disease being the most common variants. Although these two entities belong to the same disease spectrum, diagnostic distinction is of paramount importance as Maffucci's syndrome carries a higher risk of internal malignancies. Association of synovial sarcoma with Maffucci syndrome has not yet been reported in the English literature. Here we describe an advanced case of Maffucci syndrome in a Tunisian man with synovial sarcoma of the foot.
Case Report
The 48-year-old man presented to our dermatology department with an enlarging painful mass on his right foot since last 9 months. At the age of 14, he underwent multiple osteotomies due to established scoliosis and limb length discrepancies. Family history and drug history were unremarkable.
Dermatological examination revealed a prominent, irregular shaped multiloculated soft tissue tumor on the forefoot associated with several painless, bony-hard subcutaneous swellings consistent with a diagnosiof enchondromas [Figure - 1]. We also noticed several clear fluid-filled vesicles of varying sizes distributed over the entire right thigh and buttocks extending up to the abdomen., These vesicles have appeared gradually since infancy being associated with recurrent episodes of oozing, pain and fever [Figure - 1]. This clinical presentation was suggestive of lymphangioma circumscriptum. Thus, we made a diagnosis of Maffucci's syndrome; no other vascular malformation was found.
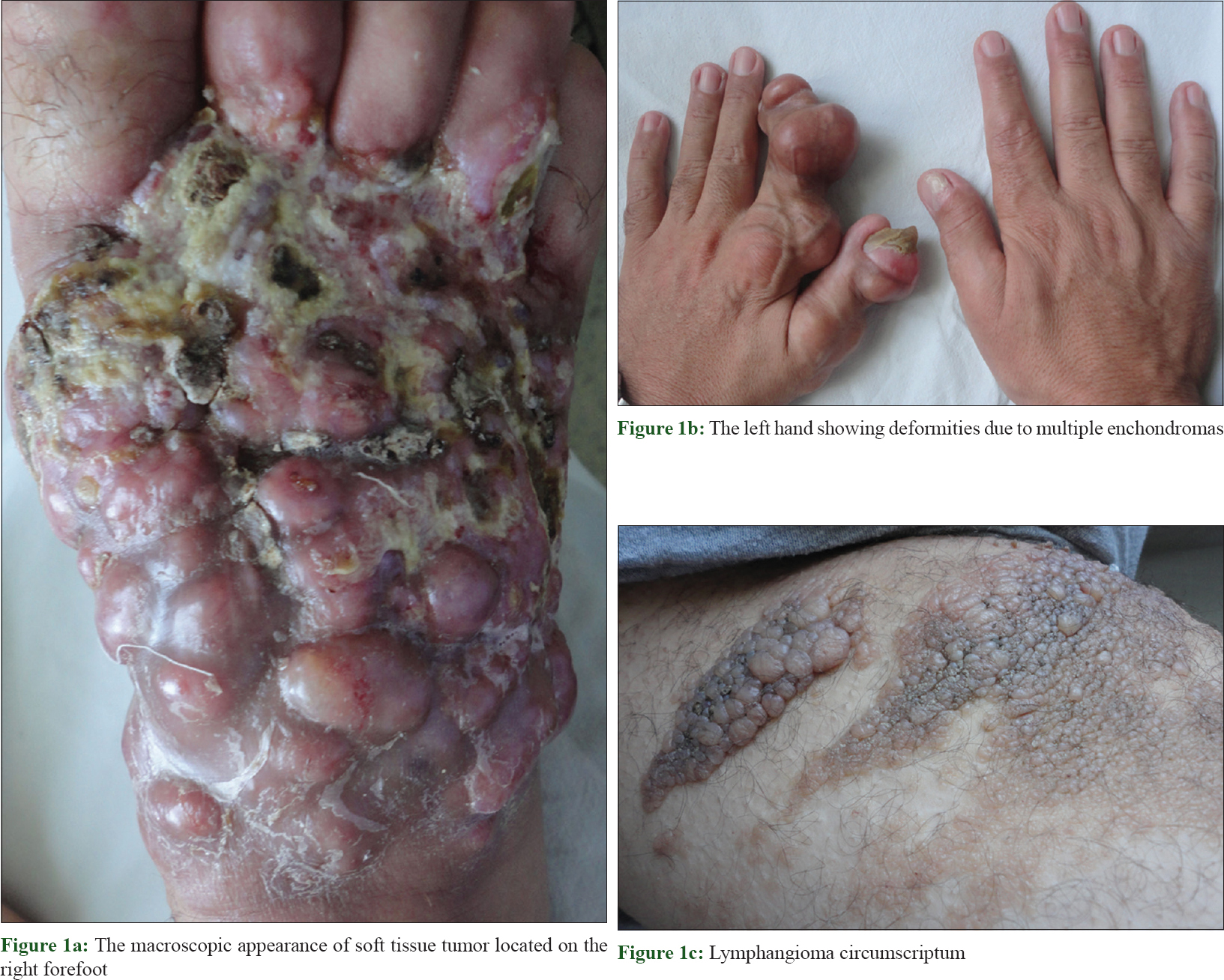 |
| Figure 1: |
We suspected the foot mass to be a soft tissue sarcoma, while Madura foot and nerve sheath tumor were considered as the differentials. A biopsy was performed, and the histopathologic study revealed two distinct cellular components: the spindle cell component interspersed with hemangiopericytoma-like vascular pattern; and the epithelial component, with epithelial cells forming glands with lumina. Spindle cells were immunoreactive for vimentin and Bcl2 but were negative for S100 protein, CD34 and muscular markers. Epithelial nests stained positive for cytokeratin [Figure - 2]. These findings were consistent with biphasic synovial sarcoma. By the fluorescence hybridization in situ technique, it was possible to demonstrate the rearrangement of the gene SYT t(X; 18). There was no evidence of distant metastasis of the tumor. After the pathological staging (T3N0M0), the patient was referred to medical oncology and orthopedics for complete surgical removal with amputation but he refused the treatment and dnot return to our office for follow-up.
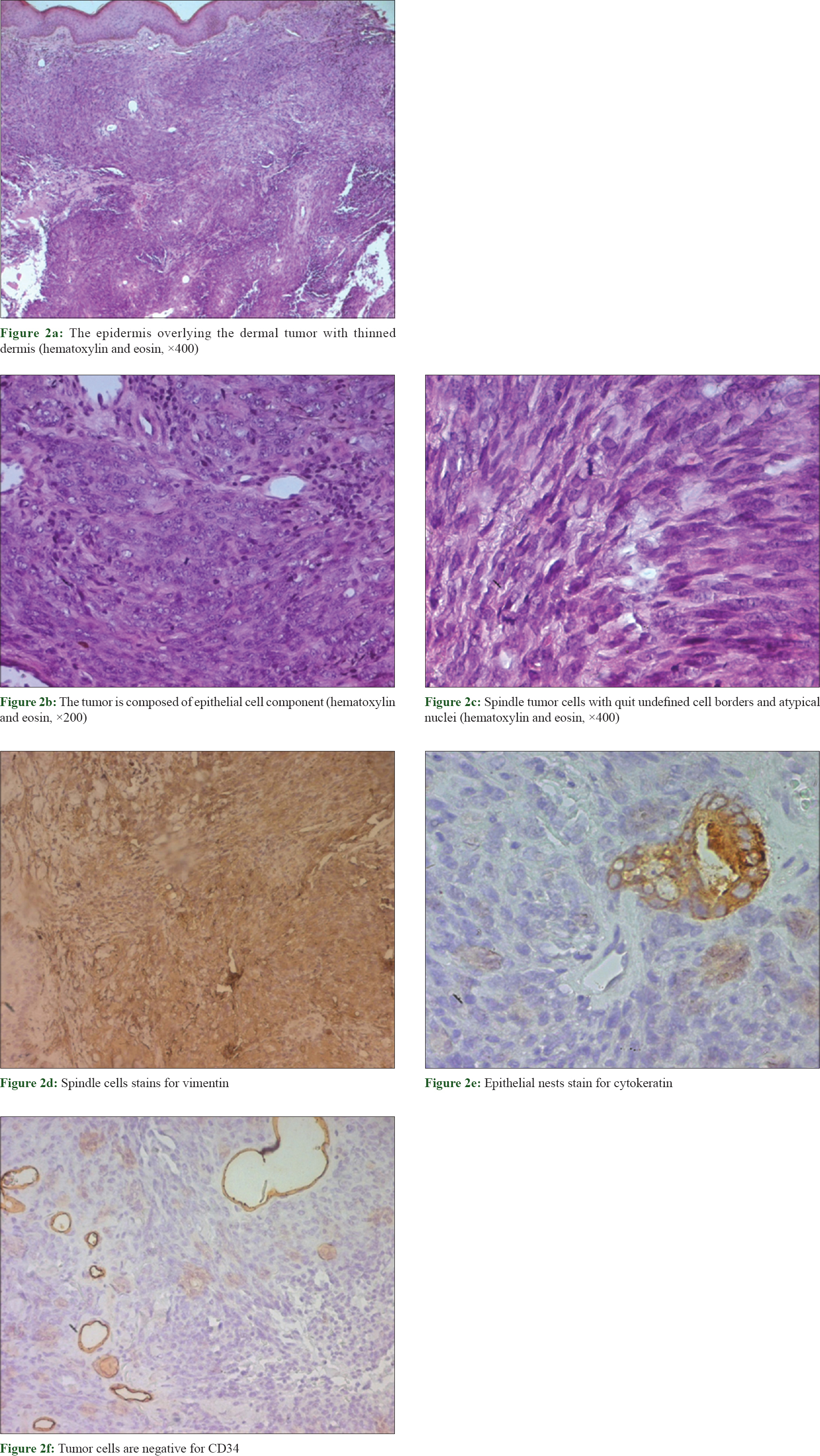 |
| Figure 2: |
Discussion
Maffucci syndrome is an exceedingly rare congenital mesodermal dysplasia characterized by multiple enchondromas, hemangiomas and less often, lymphangiomas.[1],[2],[3] We present a rare variant of this disease with lymphangioma circumscriptum as the exclusive lympho-vascular component. Till date, only few cases of this syndrome have been reported which presented with isolated lymphangiomas.[4],[5]
Maffucci syndrome carries a higher risk of internal malignancies compared to Ollier disease with a lifetime risk about 100%.[6] Schwartz et al. suggested that every patient would develop some form of malignant tumor by the age of 34 years.[7] Sarcomatous transformation occurs mainly in enchondromas, however soft tissues and bones may also be affected occassionally. To the best of our knowledge, this is the first report of synovial sarcoma in a setting of Maffucci syndrome, in the English literature. Despite its rarity (5–14% of all sarcomas), synovial sarcoma is the most common primary soft tissue sarcoma of the lower extremity and thus should be suspected in a case of any foot mass. It is characterized by the slow growth of a painful, multiloculated and well-defined mass. Histologically, it is characterized by the presence of two distinct proliferative cellular components, epithelial and spindle cell, hence the designation of biphasic sarcoma. The monophasic type refers to the proliferation of spindle cell componentalone.[8] Cytogenetic studies demonstrate the presence of gene SYT t(X;18) in more than 90% cases which is characteristic of these tumors, not occurring in other variants of soft tissue sarcoma. Similar histologic and cytologic findings were obtained in our case, thus confirming our diagnosis.
Early institution of therapy is mandated as it is a high grade tumour, surgical resection being the first-line treatment. Adjuvant radiation therapy and chemotherapy are frequently used. As synovial sarcoma is known to recur, a careful follow-up is mandatory. Synovial sarcomas may metastasize to bone, liver, skin, the central nervous system and even breast tissue. The prognosis remains bleak.[9]
We emphasize the importance of a careful clinical and radiologic follow-up of Maffucci syndrome while performing biopsies on suspicious lesions at earlier stages, when they are more amenable to treatment.
The rarity of our case has prompted this report.
Declaration of the patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Pansuriya TC, Kroon HM, Bovée JV. Enchondromatosis: Insights on the different subtypes. Int J Clin Exp Pathol 2010;3:557-69.
[Google Scholar]
|
| 2. |
Zwenneke Flach H, Ginai AZ, Wolter Oosterhuis J. Best cases from the AFIP. Maffucci syndrome: Radiologic and pathologic findings. Armed Forces Institutes of Pathology. Radiographics 2001;21:1311-6.
[Google Scholar]
|
| 3. |
Prokopchuk O, Andres S, Becker K, Holzapfel K, Hartmann D, Friess H, et al. Maffucci syndrome and neoplasms: A case report and review of the literature. BMC Res Notes 2016;9:126.
[Google Scholar]
|
| 4. |
Suringa DW, Ackerman AB. Cutaneous lymphangiomas with dyschondroplasia (Maffucci's syndrome). A unique variant of an unusual syndrome. Arch Dermatol 1970;101:472-4.
[Google Scholar]
|
| 5. |
Auyeung J, Mohanty K, Tayton K. Maffucci lymphangioma syndrome: An unusual variant of Ollier's disease, a case report and a review of the literature. J Pediatr Orthop B 2003;12:147-50.
[Google Scholar]
|
| 6. |
Lewis RJ, Ketcham AS. Maffucci's syndrome: Functional and neoplastic significance. Case report and review of the literature. J Bone Joint Surg Am 1973;55:1465-79.
[Google Scholar]
|
| 7. |
Schwartz HS, Zimmerman NB, Simon MA, Wroble RR, Millar EA, Bonfiglio M, et al. The malignant potential of enchondromatosis. J Bone Joint Surg Am 1987;69:269-74.
[Google Scholar]
|
| 8. |
Siegel HJ, Sessions W, Casillas MA Jr., Said-Al-Naief N, Lander PH, Lopez-Ben R, et al. Synovial sarcoma: Clinicopathologic features, treatment, and prognosis. Orthopedics 2007;30:1020-5.
[Google Scholar]
|
| 9. |
Deshmukh R, Mankin HJ, Singer S. Synovial sarcoma: The importance of size and location for survival. Clin Orthop Relat Res 2004419155-61.
[Google Scholar]
|
Fulltext Views
5,749
PDF downloads
2,258





![[Figure - 1]](#fig_ijdvl_2019_85_3_291_230253_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2019_85_3_291_230253_f2.jpg){kind=link}