Translate this page into:
Recurrent painful lesions on the lower lip
2 Department of Dermatology, University of Chile, Santiago, Chile
3 Department of Pathology, Hospital Santiago Oriente Dr. Luis Tisné Brousse, Santiago, Chile
Correspondence Address:
Paula Hasbún Acuña
Sargento Menadier # 1092, Postal Code. 8163345, Puente Alto, Santiago de Chile, Santiago
Chile
| How to cite this article: Acuña PH, Pardo AC, Roa MA. Recurrent painful lesions on the lower lip. Indian J Dermatol Venereol Leprol 2018;84:179-181 |
What Is Your Diagnosis?
A 25-year-old woman with no medical records presented to the Dermatology department with recurrent painful lesions in the lower lip, worsened by sun exposure, of 3-years ' duration. There was history of partial improvement in the cooler months of the year. Physical examination revealed diffuse erythema, desquamation, fissures and white/pink areas on the lower lip which appeared swollen and rough [Figure - 1]. The patient lived in the countryside, where she had worked for the last 5 years with significant sun exposure, without appropriate photoprotection. Furthermore, her mother had reported the same clinical manifestations for the last 20 years.
 |
| Figure 1: Diffuse erythema, desquamation, fissures and white/pink areas on the lower lip which appeared swollen and rough |
Incisional biopsies were performed as actinic cheilitis was suspected. The histopathology showed epithelial changes characterized by compact hyperkeratosis with parakeratosis, mild to moderate acanthosis, severe spongiosis and leukocyte exocytosis with a dense lymphohistiocytic inflammatory infiltrate of polymorphonuclear cells, some eosinophils and lymphoid follicles with germinal centers [Figure - 2]a and [Figure - 2]b.
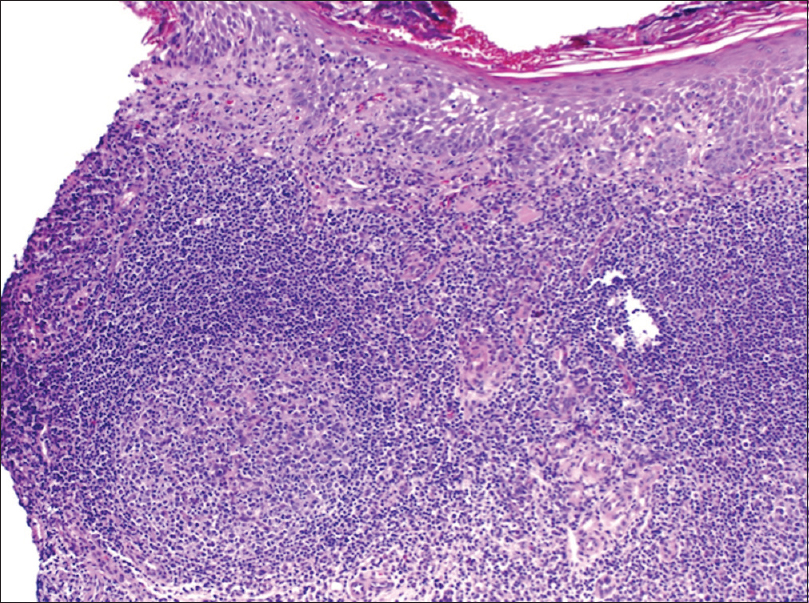 |
| Figure 2a: The epidermis exhibits hyperkeratosis, acanthosis and spongiosis. The dermis exhibits dense inflammatory infiltrates, showing reactive lymphoid follicles (H and E, ×200) |
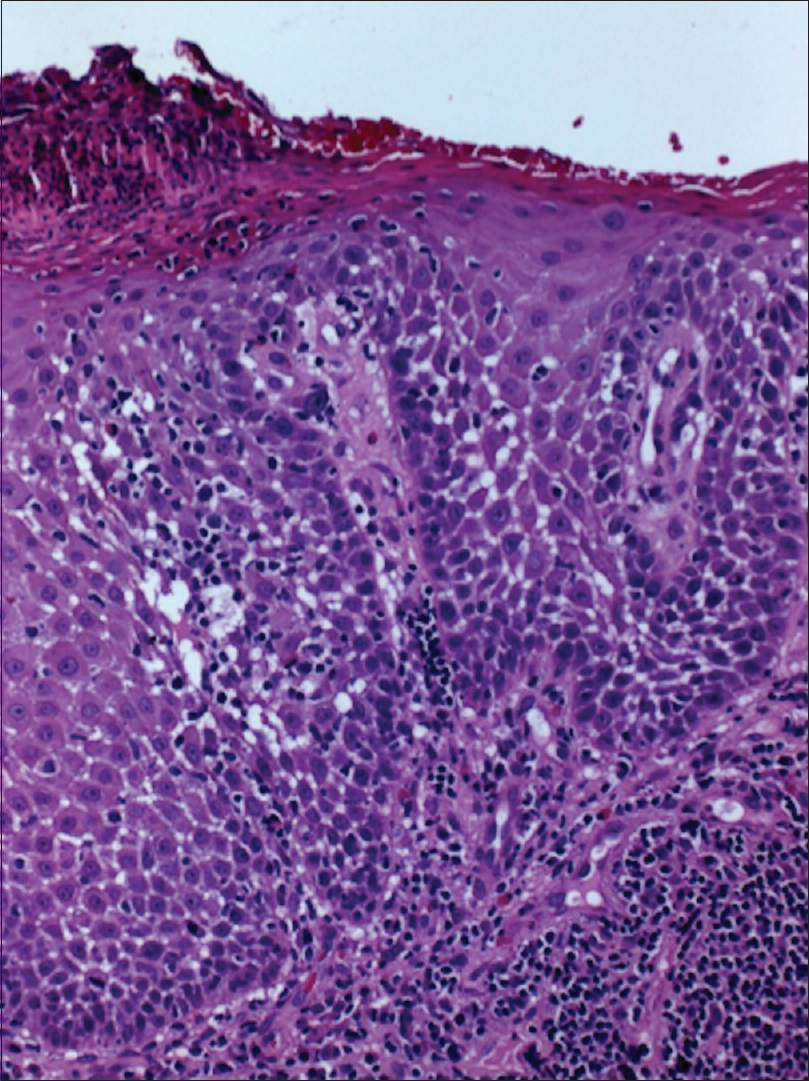 |
| Figure 2b: Irregular acanthosis, spongiosis and occasional dyskeratosis (H and E, ×400) |
Answer
Follicular cheilitis.
Discussion
Following diagnosis, triamcinolone acetonide cream 0.025% was prescribed twice daily for 10 days. In addition, the patient was instructed to apply sunscreens every 2 hrs during the day and to use physical barriers.
Complete remission of the lip lesions was observed after a month of treatment. Lesions reappeared after the patient discontinued the use of sunscreen and physical barriers.
Actinic prurigo is a chronic idiopathic photodermatosis affecting primarily sun-exposed areas. The lip involvement in actinic prurigo is known as “follicular cheilitis” and its prevalence has not yet been determined. In a recent study, 42 (56%) out of 75 patients with follicular cheilitis showed lip lesions as the only manifestation with no cutaneous involvement.[1] Follicular cheilitis may appear in patients of all ages ranging from 3 to 82 years.[1],[2] Clinically, follicular cheilitis is a chronic disease characterized by dry scaly lips with acute relapses of pain, pruritus, edema, yellowish crusts, exudation, fissures and secondary ulceration of the lip, all worsened by sun exposure.[3]
Histopathologic findings include epidermal spongiosis, intraepidermal vesicles, acanthosis, basal cell vacuolation, edema of the lamina propria, perivascular lymphocytic infiltrate, lymphoid follicles and in some cases, a variable number of eosinophils and melanophages.
Follicular cheilitis is an uncommon disease, often clinically indistinguishable from actinic cheilitis. In both cases, the vermilion border of the lower lip is most frequently affected.[4] Actinic cheilitis is an intraepithelial neoplasm induced by ultraviolet B radiation and usually requires prolonged sunlight exposure to develop enough cellular damage to produce malignant cell transformation.[4] Follicular cheilitis, instead, is an abnormal inflammatory reaction to sunlight exposure. The presence of pruritus can help differentiate follicular cheilitis from actinic cheilitis, but it is not a pathognomonic finding.
Other differential diagnoses of follicular cheilitis include: (1) photoallergic and photocontact dermatitis, (2) granulomatous cheilitis and (3) frictional contact cheilitis.
- In photoallergic and photocontact dermatitis, there is an exposure to systemic or topical agents. When this diagnosis is suspected, it is necessary to do a photopatch test.
- Granulomatous cheilitis is a painless chronic disease which usually affects the upper lip, mainly characterized by swelling. Its histopathology is non-specific and predominantly reveals nonnecrotizing granulomas.[5] In addition, the lymphoid follicles with germinal centers observed on the histopathology of the patient are considered to be a pathognomonic finding of follicular cheilitis.
- Frictional contact cheilitis is associated with repeated trauma.
- With regard to the treatment of follicular cheilitis, the most important recommendations are the reduction of sun exposure and the use of sunscreen every 2 hrs and physical barriers. These therapeutic measures can be very effective and prevent the need for additional treatments.
Conclusion
Follicular cheilitis is a chronic familial photodermatosis characterized by an abnormal inflammatory reaction to sunlight exposure. It is an uncommon condition and it could be clinically indistinguishable from actinic cheilitis. Other differential diagnoses include photoallergic and photocontact dermatitis, granulomatous cheilitis and frictional contact cheilitis. Education and general measures are the therapy of choice.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Plaza JA, Toussaint S, Prieto VG, Mercadillo P, Diez de Medina JC, Lourenco S, et al. Actinic prurigo cheilitis: A clinicopathologic review of 75 cases. Am J Dermatopathol 2016;38:418-22.
[Google Scholar]
|
| 2. |
Vega-Memije ME, Mosqueda-Taylor A, Irigoyen-Camacho ME, Hojyo-Tomoka MT, Domínguez-Soto L. Actinic prurigo cheilitis: Clinicopathologic analysis and therapeutic results in 116 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;94:83-91.
[Google Scholar]
|
| 3. |
Miranda AM, Ferrari TM, Werneck JT, Junior AS, Cunha KS, Dias EP. Actinic prurigo of the lip: Two case reports. World J Clin Cases 2014;2:385-90.
[Google Scholar]
|
| 4. |
Wood NH, Khammissa R, Meyerov R, Lemmer J, Feller L. Actinic cheilitis: A case report and a review of the literature. Eur J Dent 2011;5:101-6.
[Google Scholar]
|
| 5. |
Martínez Martínez ML, Azaña-Defez JM, Pérez-García LJ, López-Villaescusa MT, Rodríguez Vázquez M, Faura Berruga C. Granulomatous cheilitis: A report of 6 cases and a review of the literature. Actas Dermosifiliogr 2012;103:718-24.
[Google Scholar]
|
Fulltext Views
5,181
PDF downloads
2,757





![[Figure - 1]](#fig_ijdvl_2018_84_2_179_206092_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_2_179_206092_f2.jpg){kind=link}