Translate this page into:
A subungual angiokeratoma with characteristic clinical and dermoscopic features
Correspondence Address:
Hoon Kang
Department of Dermatology, St. Paul's Hospital, College of Medicine, The Catholic University of Korea, 180, Wangsan-ro, Dongdaemun-gu, Seoul 02559
Republic of Korea
| How to cite this article: Sohn KM, Woo YJ, Kim JE, Kang H. A subungual angiokeratoma with characteristic clinical and dermoscopic features. Indian J Dermatol Venereol Leprol 2018;84:230-231 |
Sir,
An angiokeratoma is a benign vascular lesion characterized by superficial vascular ectasia and overlying epidermal hyperplasia. Many types of angiokeratomas have been described in the literature: solitary angiokeratoma, angiokeratoma corporis diffusum, angiokeratoma of Mibelli, angiokeratoma of Fordyce, angiokeratoma circumscriptum naeviforme and angiokeratoma of the tongue.[1] However, the development of angiokeratoma in the subungual region has rarely been reported. We herein describe an unusual case of a subungual angiokeratoma presenting with interesting clinical and dermoscopic features.
A 52-year-old woman was referred to us with a suspected diagnosis of subungual melanoma. She had noticed a brownish streak underneath the nail of her left little finger a year back and the pigmentation became more intense during the last 3 months. Physical examination revealed a dark brown longitudinal band, 3 mm in width on the left little fingernail [Figure - 1]a. Dermoscopic examination, using a DermLite DL3 (3Gen, San Juan Capistrano, CA, USA) at 10-fold magnification with non-polarized light revealed that the streak was composed of red-brown to dark brown lacunae and dots with a light brown background and focal mild dystrophic changes [Figure - 1]b. Based on the clinical and dermoscopic features, subungual hemorrhage was suspected. However, we could not rule out the possibility of the presence of a coincident neoplastic condition as there was accompanying focal nail dystrophy. Moreover, the duration of the lesion was longer than what one would expect with a typical subungual hemorrhage. Further, the nail pigmentation secondary to hemorrhage usually shows an irregular globular shape, while here the presentation was longitudinal. We decided to perform a histopathologic examination and the biopsy was taken targeting the nail matrix at the proximal nail fold adjacent to the longitudinal band using a 3-mm punch. Histopathological examination revealed erythrocyte aggregates in the ventral nail plate and a vascular lesion surrounded by nail matrix epithelium without atypical melanocytic proliferation [Figure - 2]. This was consistent with the histopathological appearance of angiokeratoma, in which intraepidermal hemorrhage with ectatic vessels and thrombosis is often seen. We recommended electrocautery of the lesion to the patient, but she was lost to follow-up.
 |
| Figure 1a: Physical examination revealed a dark brown longitudinal band of 3 mm width on the left little fingernail |
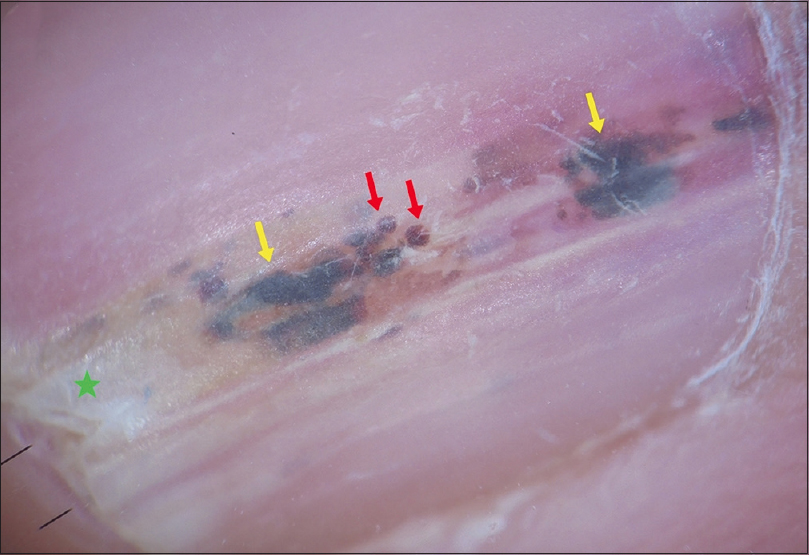 |
| Figure 1b: Dermoscopic examination disclosed a streak composed of red brown (red arrows) to dark brown (yellow arrows) lacunae and dots with a light brown background and focal mild dystrophic change (green star) (×100) |
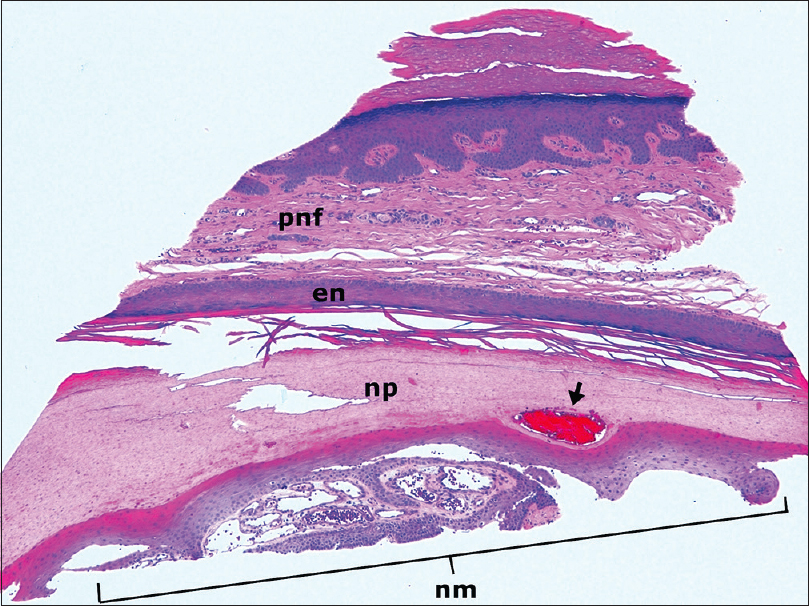 |
| Figure 2a: Histopathological examination revealed erythrocyte aggregates in the ventral nail plate (arrow) and ectatic vessels and thrombosis surrounded by nail matrix epithelium under the nail plate. pnf: Proximal nail fold, en: Eponychium; np: Nail plate, nm: Nail matrix (hematoxylin and eosin stain, ×40) |
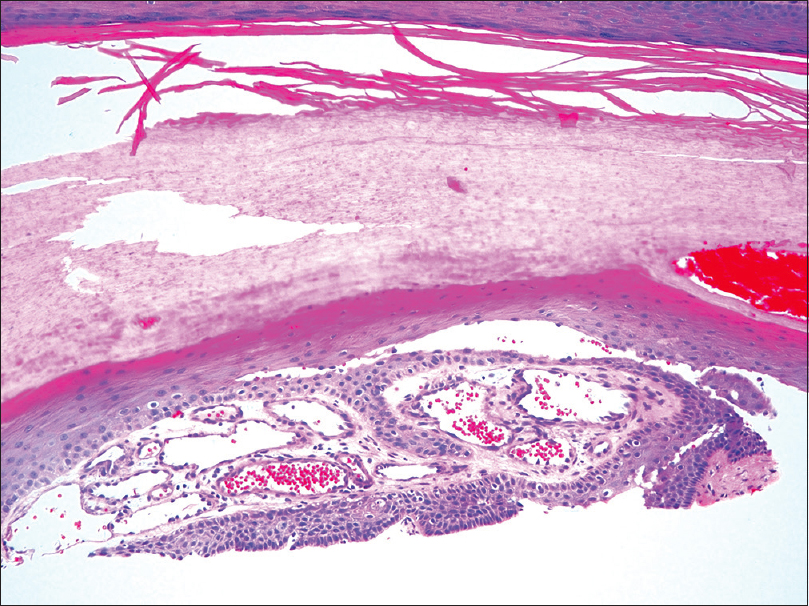 |
| Figure 2b: Histopathological examination revealed erythrocyte aggregates in the ventral nail plate (arrow) and ectatic vessels and thrombosis surrounded by nail matrix epithelium under the nail plate. pnf: Proximal nail fold, en: Eponychium; np: Nail plate, nm: Nail matrix (hematoxylin and eosin stain, ×100) |
The development of angiokeratoma in the subungual region and its pathophysiology has not been well known until now. Some reports suggest that the development of angiokeratomas is associated with increased venous pressure, proximal to the lesions.[2],[3] It has also been suggested that the development of solitary angiokeratomas may be triggered by previous trauma in the area, in which the lesions appear later.[4] As the fingers are easily exposed to trauma, it can be assumed that the lesion in this patient might have been triggered by previous trauma or accumulated damage.
We could find only one previous report of a longitudinal pigmented band caused by an angiokeratoma.[3] In that case, the patient presented with a longitudinal band on the toenail and a streak composed of red brown to dark brown globules with a light brown background was identified on dermoscopic examination. Histopathological examination revealed intraungual hemorrhage from a subungual angiokeratoma arising in the nail matrix. The authors also suspected an association of the lesion with venous incompetence and varicosities in the legs.
Zaballos et al. have suggested that dermoscopic features like dark lacunae, a whitish veil, erythema, peripheral erythema, red lacunae and hemorrhagic crusts are observed in at least 50% of the solitary angiokeratomas that occur on the body surface.[4] Although the dermoscopic features of a subungual angiokeratoma have not been well described due to its rarity, we herein suggest that the presence of a streak or linear grouped pattern of red brown to dark brown lacunae and dots with dystrophic change indicate a subungual angiokeratoma.
The causes of a pigmented longitudinal band on the nail are diverse and include subungual hemorrhage; melanocytic lesion (including lentigo, nevus, and melanoma); nail apparatus tumor; fungal infection; drugs; radiation; trauma; ethnicity; and inflammatory disorders.[5] The most concerning cause is subungual melanoma and dermoscopic examination was helpful in eliminating that possibility in our case. The dermoscopic findings of irregular longitudinal lines, Hutchinson's sign, a wide pigmented band or triangular pigmentation are associated with subungual melanoma.[5] In our case, the dermoscopic features were similar to those of a subungual hematoma with reddish-black globules. It is postulated that hemorrhages from an angiokeratoma in the matrix were incorporated into the nail plate and resulted in persistent longitudinal bands.
The present case is the second reported case of an angiokeratoma located in the subungual area. Despite its rare occurrence, dermatologists should consider the diagnosis of subungual angiokeratoma when a longitudinal pigmented band in the nail exhibits dermoscopic features similar to those seen in our case.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Zampetti A, Orteu CH, Antuzzi D, Bongiorno MR, Manco S, Gnarra M, et al. Angiokeratoma: Decision-making aid for the diagnosis of Fabry disease. Br J Dermatol 2012;166:712-20.
[Google Scholar]
|
| 2. |
Erkek E, Basar MM, Bagci Y, Karaduman A, Bilen CY, Gokoz A, et al. Fordyce angiokeratomas as clues to local venous hypertension. Arch Dermatol 2005;141:1325-6.
[Google Scholar]
|
| 3. |
Hasegawa M, Tamura A. Subungual angiokeratoma presenting as a longitudinal pigmented band in the nail. Acta Derm Venereol 2015;95:1001-2.
[Google Scholar]
|
| 4. |
Zaballos P, Daufí C, Puig S, Argenziano G, Moreno-Ramírez D, Cabo H, et al. Dermoscopy of solitary angiokeratomas: A morphological study. Arch Dermatol 2007;143:318-25.
[Google Scholar]
|
| 5. |
Braun RP, Baran R, Le Gal FA, Dalle S, Ronger S, Pandolfi R, et al. Diagnosis and management of nail pigmentations. J Am Acad Dermatol 2007;56:835-47.
[Google Scholar]
|
Fulltext Views
3,431
PDF downloads
1,433





![[Figure - 1]](#fig_ijdvl_2018_84_2_230_223997_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_2_230_223997_f2.jpg){kind=link}