Translate this page into:
Proposed global drooping and wrinkles classification and scoring system for aging face with validation and experience on 54 Indian subjects
Correspondence Address:
Suruchi Garg
Aura Skin Institute, SCO44-45, Sector 9D, Madhya Marg, Chandigarh - 160 009
India
| How to cite this article: Garg S, Khan N, Makadia S. Proposed global drooping and wrinkles classification and scoring system for aging face with validation and experience on 54 Indian subjects. Indian J Dermatol Venereol Leprol 2018;84:672-677 |
Abstract
Background: Aging is an inevitable biological change, but understanding the process of aging of face is important to customize the treatment options for facial rejuvenation. Evidence-based estimation of global facial aging is necessary for the validation of various treatment modalities.
Aims: Classification and implementation of a scoring system for aging face based upon volume loss and surface changes as evident by drooping of different areas of the face and appearance of fine and deep wrinkles, respectively, and to apply this drooping–wrinkles classification on 54 participants to evaluate and understand the validity of scoring.
Methods: An observational study was conducted, and scores were calculated based on 13 parameters (7 areas of drooping and 6 areas of wrinkles on the face) at Aura Skin Institute, Chandigarh, India. Accordingly, age was divided in different age groups followed by clinical estimation of facial age and calculation of scores.
Results: According to our classification and scoring system, 61% (33 out of 54) of the participants were correlated with their chronological age group. Out of the remaining 21 (39%) participants who were aging faster, 13 (24%) were in the age group of 25–35 years. Approximately one-fourth of the patients in the age groups 36–45 and 46–55 years were aging faster. Only 1 patient had scores showing younger age in comparison to chronological age. Overall, there was a good correlation between the calculated score and the chronological age of patients. Moreover, a gradual increase in scores was noticed with increasing age groups.
Conclusions: This is a new clinical classification and scoring system for facial age which is much easier to apply in daily clinical practice for easy calculation of baseline scores and customizing their antiaging treatment options. Moreover, it will also make it easier to compare the efficacy of treatment in their future follow-ups. The limitation of this study is that it has been proposed for all skin types but validation has been done only for Indian participants.
Introduction
Every living being goes through the cycle of growth followed by aging. Though aging is inevitable, most of us do not like to look old and want to maintain our youthful look. Understanding the process and stages of aging face is of significant importance in planning and executing the various treatment options for facial rejuvenation. The latter has evolved from simple facelift procedures in the past to a variety of procedures such as thread lift, botulinum toxin, fillers, lasers, intense pulse light and chemical peels that has to be customized to each individual as different people age differently.[1] Evidence-based estimation of global facial aging is often necessary, especially for validation of these treatment modalities.[2] All the layers of the face such as skin, fat, muscle and bone age very dynamically. The human face may look older than it actually is due to accelerated skeletal, soft tissue and dermatological changes.[3] Therefore, to get a good result after rejuvenation procedure, it is of paramount importance to understand the effect of aging process on them.[4]
It is equally important to classify an aging face to help one choose the best combination of available facial rejuvenation procedures to offer the best result to the clients.[5] Although many clinical classifications for facial aging have been laid down in the recent past, they are still not fully satisfactory. Many of them have utilized limited areas of the face affected by aging process, which do not target the entire face and also do not include surface changes, making it difficult for clinicians to classify the patients and prepare their treatment framework.[5] Others are too complicated to be used by clinicians for daily practice.[2] Even the recently available digital software are not accurate in estimating facial age because of the variable effects of light, projection, camera effect, pose and expressions. After thorough literature review, we were unable to find a clinical scoring system which can be easily utilized by clinicians to analyze facial aging and assess treatment response.
In our study, we have taken into consideration seven areas of the face for sagging or drooping and six areas for wrinkles, and have devised a scoring system as an effort to simplify facial age estimation by assessing drooping and wrinkles as well as reduce the time required in customizing treatment options for individual participants along with an easier follow-up assessment and validation of the treatment modality offered.
Aim
Classification and implementation of a scoring system for aging face based upon volume loss and surface changes as evident by drooping of different areas of the face and appearance of fine and deep wrinkles, respectively, and applying this global drooping–wrinkles classification on 54 participants to evaluate the validity of the scoring.
Methods
This observational study was conducted in the Dermatology outpatient department at Aura skin institute after obtaining written and informed consent from the patients. All individuals above 25 years attending the dermatology outpatient department were included in the study. Participants who had undertaken antiaging treatments previously were excluded from the study. Their age and clinical photographs in standard five angles (front, frontolateral and sides) were taken followed by clinical estimation of facial age and calculation of scores.
Classification
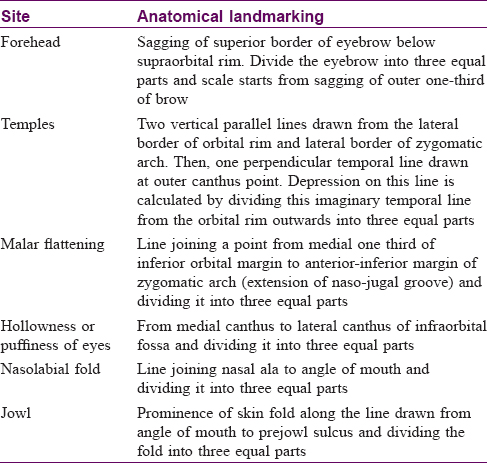
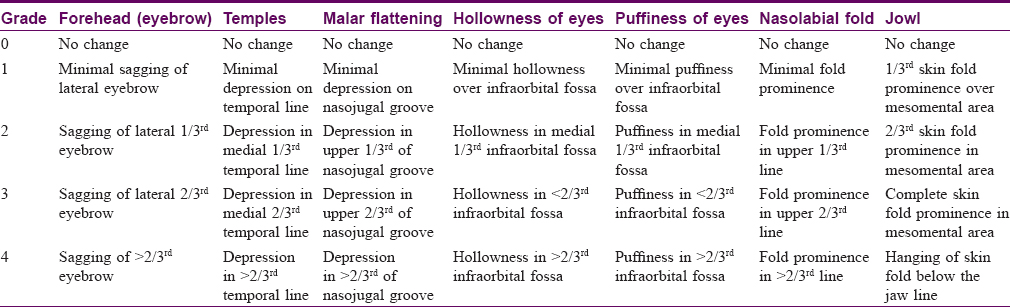
We have taken into consideration seven areas all over the face for drooping including forehead, temples, malar flattening, hollowness of eyes, puffiness of eyes, nasolabial folds and jowl [Table - 1] and [Table - 2] and [Figure - 1].
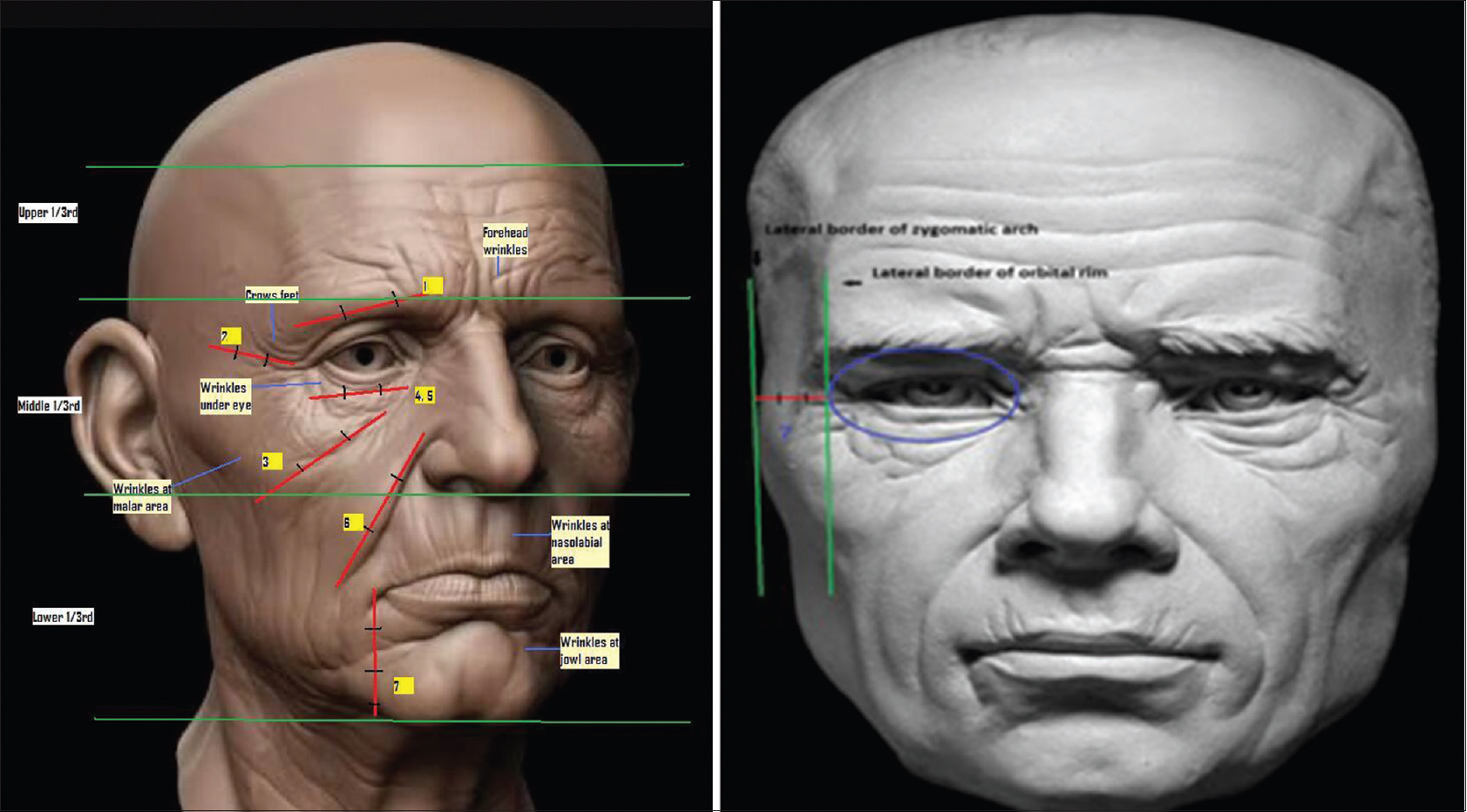 |
| Figure 1: Diagrammatic representation of areas of drooping and wrinkles (P.C.-Rodion's sketchbook). Footnote: (1) Eyebrow drooping, (2) Malar depression, (3) Eye hollowness, (4) Eye puffiness, (5) Nasolabial fold, (6) Jowl, (7) Temple depression Red line – Drooping/hollowness/depression, Green line – Area demarcation of face for wrinkles |
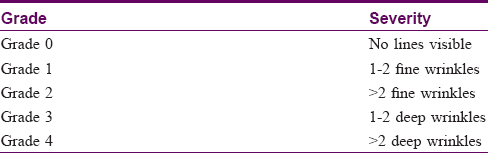
Wrinkles over the face were taken from six areas – forehead, temples, malar area, eyes, nasolabial area and jowl area – and were given grades in each area [Table - 3].
Scores were calculated based on the following thirteen parameters [7 areas of drooping and 6 areas of wrinkles (wrinkle around eyes instead of puffiness or hollowness)]; the minimum score obtained was 0 while the maximum was 52. Accordingly, calculated age was divided in different age groups [Table - 4].
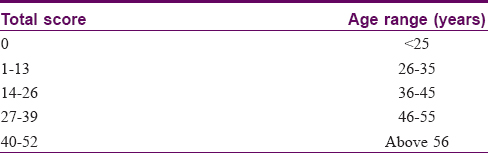
The area-based assessment can be done based on the score of individual area which varies from 0 to 8. A score of 0 signifies an age group <25 years, 1–2 shows 26–35 years, 3–4 is 36–45 years, 5–6 is 46–55 years and a score of 7–8 is >56 years. Sometimes periorbital area can age with hollowness, puffiness and wrinkles, and hence, a scoring of 0–12 will be valid here; otherwise a scoring between 0 and 8 will be good for individual assessment. For periorbital area aging with hollowness, puffiness and wrinkles, score 0 signifies the age group of <25 years, score 1–3 26–35 years, score 4–6 36–45 years, score 6–9 46–55 years and 10–12 the age group of >56 years.
Results
In our study, out of the total 54 participants, there were 9 males and 45 females. Majority of the patients were in the age group of 25–35 years. According to our classification and scoring system, 61% (33 out of 54) of the participants were corresponding with their chronological age group. Out of the 21 (39%) participants who were aging faster, 13 (24%) were in the age group of 25–35 years. Approximately 1/4th of the patients in age group 36–45 and 46–55 years were aging faster. Only 1 patient had scores showing younger age in comparison to the chronological age. Within the age group of 36–55 years, our proposed drooping–wrinkles classification was within 70–87% correlation with their actual age. Overall, there was a good correlation between the calculated score and the chronological age of patients. Moreover, gradual increase in scores was noticed with increasing age groups.
The relationship obtained between the actual age and perceptible age of patients in different age groups is described in [Table - 5] [Figure - 2], [Figure - 3], [Figure - 4], [Figure - 5].

 |
| Figure 2: Normal age: 25, drooping and wrinkles score: 19 (36–45 years) |
 |
| Figure 3: Normal age: 29, drooping and wrinkles score: 12 (26–35 years) |
 |
| Figure 4: Normal age: 45, drooping and wrinkles score: 25 (36–45 years) |
 |
| Figure 5: Normal age: 51, drooping and wrinkles score: 27 (46–55 years) |
Discussion
The concept of skin aging is contributed a lot by physiological or biological age which may not fit chronological age. Disparity has been noticed between visible age and the actual aging process which undergoes changes over years depending upon nutritional status, stress and daily caring. There can also be interindividual variation or ethnoracial variation due to different genetic backgrounds of different geographical populations.[6]
Since ages, people have used different modalities of treatments to arrest and mask the visible aging changes on the face to regain their beauty.[7],[8]
The youthful appearance and aging changes of the face are subjective and various efforts have been made to quantify facial aging to assess the need and results of various aesthetic interventions. Approaches have been made by many authors to estimate facial age who have developed rating scales based on digital photographs and even confocal microscopy of facial skin.[9] Some researchers devised scales based upon biomarker estimation.[10] However, these are technology driven approaches which are quite sophisticated for use in daily clinical practice and at times are not accurate in estimating visible age.
Many clinical classifications have been laid down by different researchers where they utilized limited areas of the face for aging signs and left out many important areas of the face where changes of aging are marked. Attempts have also been made to estimate facial age by considering specific areas of the face such as clinical score for lateral canthal lines.[11] However, in real life clinical practice when antiaging treatments have to be applied to the whole face, all these limited approaches do not work.
Till date, there are no validated and reliable global facial aging scales. Scale by Rzany et al. has been developed for European skin types using photographs.[12] A similar rating scale for the quantification of facial aging among Indian women from the Western part of India was developed by Bernois et al.[13] The quality of the photographs and the variable effects of size, luminosity, projection, color and expressions of photograph in these scales were not accurate and standardized in estimating facial age. Moreover, additional aging manifestations, such as skin texture and laxity, and whether the wrinkles are static or dynamic are best assessed by only clinical examination which is not possible while assessing facial age from a photograph. These limitations can be overcome by developing a scale for assessment of facial age which is not solely dependent on photographs but can be simply applied on clinical inspection by clinicians and aesthetic physicians.
An attempt was made by Sen et al. at developing a 13-point rating scale for estimation of facial aging in Indian population by clinical examination of skin changes; however they did not take into consideration few important areas of face such as depression over temples, sagging of eyebrow and appearance of crow's feet, which are critical in assessing facial age. Moreover, the scale is difficult to remember for application in day to day clinical practice.
We have further simplified this 13-point rating scale devised by Sen et al. by dividing the face into seven areas for drooping and six areas for wrinkles. This considerably reduces the time required to assess the facial age of patients and makes it much easier to calculate their baseline score. Further, we included patients above the age of 25 years which though shows minimal aging changes but are now frequent volunteers of antiaging treatments.
Many factors are involved in skin aging such as intrinsic factors – genetic, free radical injury, alteration in protein synthesis, exhaustion of stem cell reservoir, etc. and extrinsic factors – lifestyle, nutrition, smoking, exposure to toxins, sun exposure, etc.
Clinical signs of aging include:
Chronological
Flattening of dermoepidermal junction, increase in free water intake and decrease in proteins and proteoglycans in the superficial dermis leads to loss of transparency with cigarette paper skin, dull tone, crinkling, flaccidity or reduced firmness, which leads to fine lines or wrinkles.
Photoaging
Photoaging is more pronounced on sun exposed areas such as face, neck, volar forearm, dorsum of hand, with elastosis, pigmentation, actinic lentigines, but these changes may be less pronounced on Indian clients due to moderate presence of melanin.
In white population, since drooping is less pronounced, pigmentary changes and wrinkles are more marked; pigmentary changes can be assessed in individually defined areas along with drooping and wrinkles for precise estimation of age.
Face plays a major role in age perception of an individual where clinical signs of chronological aging and photoaging are mixed. Anatomic features are also important among signs of facial aging such as wrinkles and sagging.
Wrinkles
Wrinkles are a key sign of facial aging. Subcutaneous muscle contraction during facial expression leads to dynamic wrinkles which are anatomically localized, e.g., crow's feet, glabella, forehead, perioral, etc., which when repeated all life produces structural organization of dermal collagen fibers leading to change in texture and loss of firmness, which leads to permanent wrinkles substantiated further by the overactivity of underlying muscles. Elastosis also increases wrinkle depth and number.[3]
Facial sagging
Subcutaneous tissue changes due to normal aging, movement of mouth due to chewing and speaking and gravitational forces lead to the downward migration of fat planes causing prominence of lower cheeks, bags under eyes, increase of nasolabial folds and jowls and protrusion of the submental neck area.
Interpretation of aging signs is a subjective process. It can be mentioned that the skin has lost volume and elasticity and has developed wrinkles; however, the severity of these symptoms cannot be described.
Therefore, standardized systems for describing aging skin which will provide objective ways to evaluate emerging characteristics being displayed over time has become a necessity. More importantly, it will also help to choose the best antiaging solutions for individual patients.
Our scoring system provides an added measure of reliability for aging treatments and other recommended intervention programs along with the provision of an easier follow-up.
Majority of the participants in our study were females with cosmetic concerns. Maximum number of patients were in the age group of 25–35 years as this is the active age group of population which is more concerned about their appearance.
In this study, we noticed that as per our scoring system, majority of the participants were in the norm for their age group. Most participants who were aging faster were in the age group 25–35 years. Though we have included patients above 25 years of age, we noticed significant disparity between the chronological age and calculated age in younger group of patients (25–35 years), which was contradictory to our expectation as aging changes are mostly visible post 30 years of age. Faster aging could be explained by faulty lifestyle, stress, erratic eating habits such as diet high on junk foods and low on proteins, vitamins and minerals. This finding also implicates the need for further research to ascertain the cause of faster aging in this age group, which can be done by conducting comparative studies between different age groups. Around 1/4th of the patients in the age groups 36–45 and 46–55 years were aging faster. It can be attributed to the fact that this age group bears the maximum pressure of life and is in transition from adulthood to old age. Only 1 patient had scores showing a younger chronological age which could be because of genetic inheritance or good eating habits and skin care by the patient.[7] Approximately 70% of our participants were willing for antiaging treatments as the study was undertaken in a tertiary care lasers and cosmetic skin institute where majority of clients are concerned about their visual appearance.
This scoring system helped us in categorizing the patients making their baseline score to be assessed whether they are aging faster or not and prepare their treatment plan. The participants with a score of up to 26 usually have surface changes and can be managed effectively with chemical peels, lasers, energy-based devises, instant threads and botulinum toxin; whereas those with scores above 26 have volume loss and may require volume restoration with fillers, fat transplant, surgical threads, etc., Moreover, the scoring made it easier for the future follow up of patients when their scores can be reassessed area wise to find out problematic area/s and to analyze the treatment effect easily. Further studies can be undertaken comparing different age groups with ethnicities and gender differences.
Overall, there was a good correlation between calculated score and chronological age of patients. Moreover, gradual increase in scores was noticed with increasing age groups. This further supports the validity and usefulness of this classification and scoring system.
Limitation
Though the classification has been proposed to be applicable for all skin types, scoring and validation has been done on Indian patients only. More clinical and antiaging treatment-based studies should be done on different skin types to understand and validate this scoring system.
Conclusion
We devised a new clinical classification and scoring system for facial age which is much easier to apply in daily clinical practice by the dermatologist or plastic surgeons for easy calculation of baseline score and customizing their antiaging treatment options accordingly. Moreover, it will also make it easier to compare the efficacy of treatment in their future follow-ups.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Khazanchi RK. Facial aging: A clinical classification. Indian J Plast Surg 2007;40:181.
[Google Scholar]
|
| 2. |
Sen S, Choudhury S, Gangopadhyay A, Halder C, Biswas P, Jain A, et al. A clinical rating scale for the assessment of facial aging in Indian population. Indian J Dermatol Venereol Leprol 2016;82:151-61.
[Google Scholar]
|
| 3. |
Glogau RG. Aesthetic and anatomic analysis of the aging skin. Semin Cutan Med Surg 1996;15:134-8.
[Google Scholar]
|
| 4. |
Khazanchi R, Aggarwal A, Johar M. Anatomy of aging face. Indian J Plast Surg 2007;40:223-9.
[Google Scholar]
|
| 5. |
Shiffman MA. Facial aging: A clinical classification. Indian J Plast Surg 2007;40:178-80.
[Google Scholar]
|
| 6. |
Querleux B, Baldeweck T, Diridollou S, de Rigal J, Huguet E, Leroy F, et al. Skin from various ethnic origins and aging: An in vivo cross-sectional multimodality imaging study. Skin Res Technol 2009;15:306-13.
[Google Scholar]
|
| 7. |
Gunn DA, Rexbye H, Griffiths CE, Murray PG, Fereday A, Catt SD, et al. Why some women look young for their age. PLoS One 2009;4:e8021.
[Google Scholar]
|
| 8. |
Kreyden OP. Antiaging – A scientific topic or just a social trend? J Cosmet Dermatol 2005;4:228-9.
[Google Scholar]
|
| 9. |
Longo C, Casari A, De Pace B, Simonazzi S, Mazzaglia G, Pellacani G, et al. Proposal for an in vivo histopathologic scoring system for skin aging by means of confocal microscopy. Skin Res Technol 2013;19:e167-73.
[Google Scholar]
|
| 10. |
Chang AL, Lingala B, Chang TC, Kern DG, Wood SM, Toyoda H, et al. An exploratory study to determine the association between assessed facial skin aging and plasma isoprostane levels in middle-aged Japanese women. Dermatol Surg 2012;38:462-70.
[Google Scholar]
|
| 11. |
Hund T, Ascher B, Rzany B; Smile Study Group. Reproducibility of two four-point clinical severity scores for lateral canthal lines (crow's feet). Dermatol Surg 2006;32:1256-60.
[Google Scholar]
|
| 12. |
Rzany B, Carruthers A, Carruthers J, Flynn TC, Geister TL, Görtelmeyer R, et al. Validated composite assessment scales for the global face. Dermatol Surg 2012;38:294-308.
[Google Scholar]
|
| 13. |
Bernois A, Huber A, Derome C, Drouault Y, de Quéral D, Schnebert S, et al. A photographic scale for the evaluation of facial skin aging in Indian women. Eur J Dermatol 2011;21:700-4.
[Google Scholar]
|
Fulltext Views
5,105
PDF downloads
1,429





![[Table - 1]](#tbl_ijdvl_2018_84_6_672_233803_t6.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2018_84_6_672_233803_t7.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2018_84_6_672_233803_f1.jpg){kind=link}
![[Table - 3]](#tbl_ijdvl_2018_84_6_672_233803_t8.jpg){kind=link}
![[Table - 4]](#tbl_ijdvl_2018_84_6_672_233803_t9.jpg){kind=link}
![[Table - 5]](#tbl_ijdvl_2018_84_6_672_233803_t10.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_6_672_233803_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2018_84_6_672_233803_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2018_84_6_672_233803_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2018_84_6_672_233803_f5.jpg){kind=link}