Translate this page into:
Histoid leprosy presenting with figurate lesions: A unique and rare presentation
Correspondence Address:
Angoori Gnaneshwar Rao
F12, B8, HIG-2 APHB, Baghlingampally, Hyderabad - 500 044, Telangana
India
| How to cite this article: Rao AG, Kolli A, Farheen SS, Reddy UD, Karanam A, Jagadevapuram K, Haqqani R. Histoid leprosy presenting with figurate lesions: A unique and rare presentation. Indian J Dermatol Venereol Leprol 2018;84:736-739 |
Sir,
Histoid leprosy rarely presents with figurate lesions. Here we report such a presentation in a young man. A 37-year-old man presented to us with multiple asymptomatic skin-colored papules on the face and trunk for the last 6 months. Examination revealed multiple shiny, dome-shaped, firm skin colored papules and nodules on an apparently normal skin, arranged in linear, curvilinear, arciform and annular pattern affecting the face, temple and front of chest. Some of the papules showed central depression [Figure - 1], [Figure - 2], [Figure - 3]. Both ulnar, lateral popliteal and supratrochlear nerves were thickened and nontender. We made a provisional diagnosis of histoid leprosy, while cutaneous sarcoidosis, xanthomata and dermatofibroma were considered as the differentials. All routine investigations including Venereal Disease Research Laboratory test and human immune deficiency virus 1 and 2 serology were unremarkable. Lesional and ear-lobe Slit-skin smears showed discreet and clumped long, slender, acid-fast bacilli [Figure - 4] (bacteriological index: 6+, morphological index: 5%). Biopsy from the curvilinear lesion on the front of right lower chest showed grenz zone with a dense collection of foamy histiocytes, spindle cells and few lymphocytes thus confirming the diagnosis of histoid leprosy. [Figure - 5] and [Figure - 6]. The patient was started on multibacillary multidrug therapy resulting in considerable resolution of all the figurate lesions of histoid leprosy by 3 months. [Figure - 7], [Figure - 8], [Figure - 9].
 |
| Figure 1: Annular plaque on the left side of the face below temple and small plaque on left cheek |
 |
| Figure 2: Linear plaque on the right cheek extending toward inner canthus |
 |
| Figure 3: Curvilinear plaque on the front of lower chest and trunk |
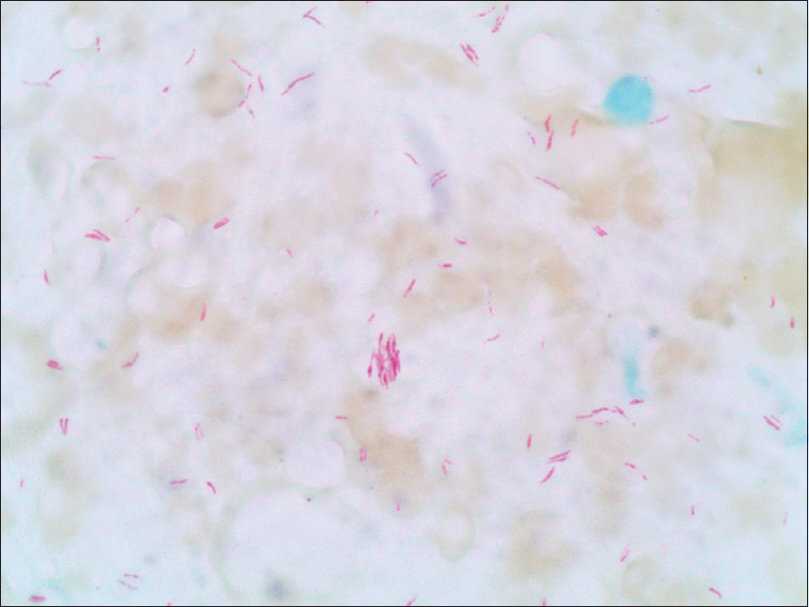 |
| Figure 4: Slit-skin smear from nodule showing solid staining and granular lepra bacilli both singly and in groups (Ziehl–Neelsen, ×1000) |
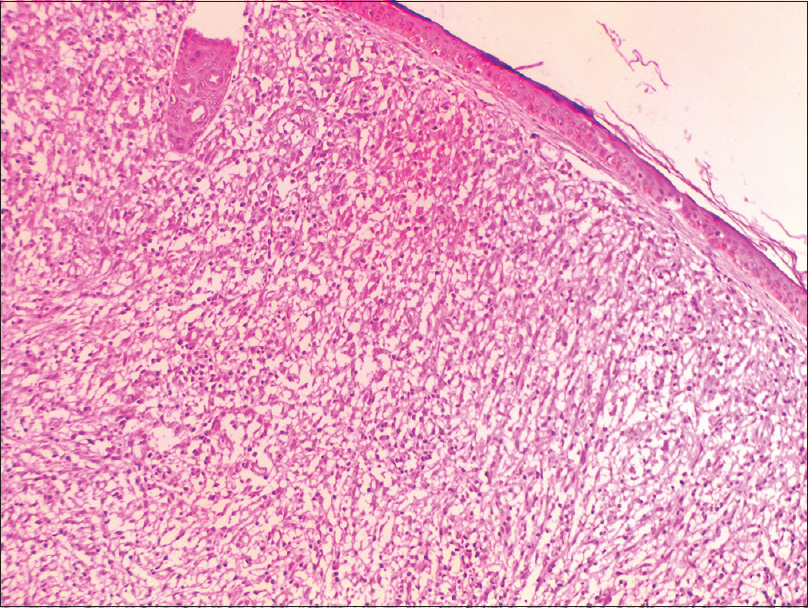 |
| Figure 5: Histopathology of nodule showing grenz zone and dense collection of foamy histiocytes, spindle cells [hematoxylin and eosin (H and E), ×100] |
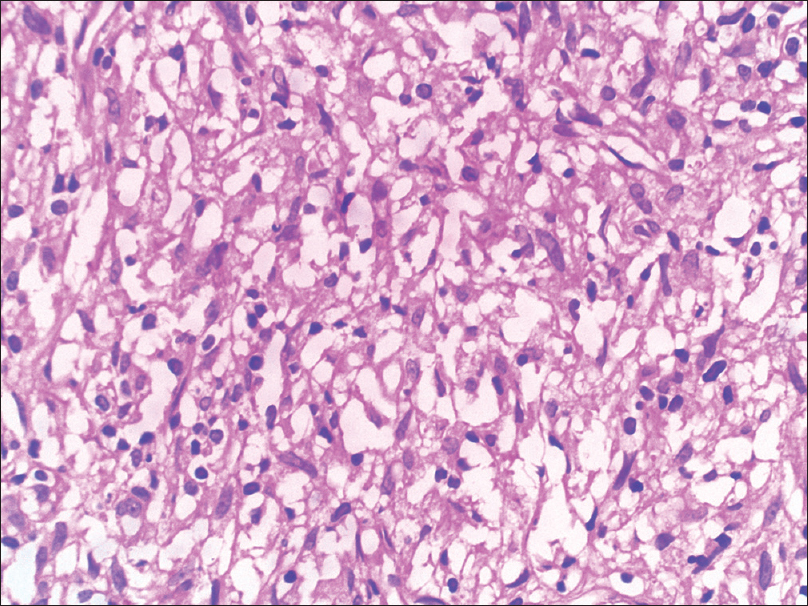 |
| Figure 6: Histopathology of nodule showing dense collection of foamy histiocytes, spindle cells (H and E, ×400) |
 |
| Figure 7: Considerable resolution of plaques on left cheek and temple following 3 months of multibacillary multidrug therapy |
 |
| Figure 8: Considerable resolution of plaque on the right cheek posttreatment |
 |
| Figure 9: Partial resolution of plaque on the lower chest and trunk posttreatment |
The term histoid is derived from the microscopic appearance of the nodule showing spindle-shaped cells resembling dermatofibroma. Histoid leprosy is an uncommon variant of lepromatous leprosy, first described by Wade in 1960.[1] It is characterized by skin colored papules and/or subcutaneous nodules and plaques on an apparently normal skin with distinct histopathology and characteristic bacterial morphology. It is usually seen in patients relapsing after dapsone monotherapy and in the presence of dapsone resistance. An occurrence of 1.2% has been reported among lepromatous leprosy patients.[2]
The cell-mediated immunity is better in histoid leprosy than in active lepromatous patients as substantiated by increased CD36 expression by the keratinocytes, predominance of CD4 lymphocyte over CD8 lymphocytes and increased number of activated lymphocytes and macrophages in the lesion.[2] Bacteriologically, there is large bacillary load in histoid lesions, which is attributed to the focal loss of immunity. Furthermore, the acid-fast bacilli in these cases are measurably longer than ordinary lepra bacilli and are arranged in groups or parallel bundles in spindle-shaped histiocytes, described as histoid habitus by Wade. One of the significant electron microscopic features of histoid lesion is the absence of electron transparent zone or foam, which interferes with bacterial metabolism leading to cell death, in contrast to lepromatous lesions. The absence of this zone probably results in intracellular preservation of bacilli within the histoid lesions.[3]
Umbilicated papules resembling molluscum contagiosum have been reported rarely in histoid leprosy. Nonetheless, some of the papules displayed umbilication in our case. Although the definite cause of umbilication is unclear, central softening secondary to high bacterial load is a possible mechanism. Namisato et al. proposed the phenomena of transepidermal elimination of lepra bacilli from the lesions and consequent implantation following trivial trauma, which results in the formation of new lesions of leprosy;[4] similar to the pseudo-isomorphic phenomenon observed in warts and molluscum contagiosum. The disposition of lesions in our case is novel and unique as it evolved into various figurate forms, viz., linear, curvilinear, arciform and annular pattern, distributed asymmetrically. These linear, curvilinear and arciform lesions may be explained by the pseudo-isomorphic phenomenon. In concert with linear molluscoid lesions reported in the literature, the index case also revealed linear molluscoid morphology.[5]
The possible mechanism for the characterization of annular lesions in leprosy has been elucidated by Lee et al., by immunological studies on biopsy specimens from the inner active border and outer perilesional normal skin to detect more than 50% T-cells, with predominance of T-helper cells in the dermis with 75% HLA-DR positivity at the active border.[6] In contrast, 40% T cells with an equal number of T-helper and T-suppressor cells with 10% HLA-DR positivity was detected inside the active border. Based on these findings, they highlighted the important role of T-cell-mediated immune response against Mycobacterium leprae in the formation and extension of annular lesions in leprosy. Similarly, the same immunological mechanism may be ascribed for the formation of annular plaques in our case.
In conclusion, occurrence of figurate lesions in histoid leprosy is rare and these morphological patterns may be added to the various manifestations of histoid leprosy.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Wade HW. The histoid leproma. Int J Lepr 1960;28:469-70.
[Google Scholar]
|
| 2. |
Sehgal VN, Gautam RK, Srivastava G, Koranne RV, Beohar PC. Erythema nodosum leprosum (ENL) in histoid leprosy. Indian J Lepr 1985;57:346-9.
[Google Scholar]
|
| 3. |
Job CK, Chacko CJ, Taylor PM. Electromicroscopic study of histoid leprosy with special reference to its histogenesis. Lepr India 1977;49:467-71.
[Google Scholar]
|
| 4. |
Namisato M, Kakuta M, Kawatsu K, Obara A, Izumi S, Ogawa H, et al. Transepidermal elimination of lepromatous granuloma: A mechanism for mass transport of viable bacilli. Lepr Rev 1997;68:167-72.
[Google Scholar]
|
| 5. |
Ghorpade A. Molluscoid skin lesions in histoid leprosy with pseudo-isomorphic Koebner phenomenon. Int J Dermatol 2008;47:1278-80.
[Google Scholar]
|
| 6. |
Lee CW, Lee HY, Son SJ, Kim Do 2nd. In situ characterization of immune cells in the annular lesions of leprosy. Korean J Dermatol 1986;24:49-55.
[Google Scholar]
|
Fulltext Views
10,920
PDF downloads
2,030





![[Figure - 1]](#fig_ijdvl_2018_84_6_736_242675_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_6_736_242675_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2018_84_6_736_242675_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2018_84_6_736_242675_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2018_84_6_736_242675_f5.jpg){kind=link}
![[Figure - 6]](#fig_ijdvl_2018_84_6_736_242675_f6.jpg){kind=link}
![[Figure - 7]](#fig_ijdvl_2018_84_6_736_242675_f7.jpg){kind=link}
![[Figure - 8]](#fig_ijdvl_2018_84_6_736_242675_f8.jpg){kind=link}
![[Figure - 9]](#fig_ijdvl_2018_84_6_736_242675_f9.jpg){kind=link}