Translate this page into:
Dermoscopy of Biett's sign and differential diagnosis with annular maculo-papular rashes with scaling
2 Department of Dermatology, Division of Medical, Surgical and Neurosciences, University of Siena, Siena, Italy
Correspondence Address:
Linda Tognetti
Department of Medical, Surgical and Neuro-Sciences, Dermatology Unit, University of Siena, Siena; Department of Medical Biotechnologies, University of Siena, Siena
Italy
| How to cite this article: Tognetti L, Sbano P, Fimiani M, Rubegni P. Dermoscopy of Biett's sign and differential diagnosis with annular maculo-papular rashes with scaling. Indian J Dermatol Venereol Leprol 2017;83:270-273 |
Laurent-Théodore Biett (1781–1840), a Swiss-born dermatologist, first described the thin white ring of scaling on the surface of secondary syphilis papules since known as “Biett's collarette.”[1] Although the clinical features allow the diagnosis of secondary syphilis in most cases, it may be at times difficult to differentiate it from other annular maculo-papular dermatoses with scaling. Dermoscopy has been most often used to improve the diagnostic accuracy in the clinical evaluation of pigmented skin lesions but it has also been found useful in the assessment of vascular structures that are not visible to the naked eye. As a consequence, dermoscopy has been more widely employed for the differential diagnosis of even non-pigmented skin conditions including tumors and also inflammatory and infectious dermatoses.[2],[3],[4],[5],[6],[7] Though some dermatoscopic features appear to be highly specific for a particular disease, others can be seen in more than one entity and are subsequently considered “non-specific.” However, a “non-specific” dermatoscopic feature may be rendered particularly valuable when coupled with certain other clinical and/or dermoscopic criteria, forming a set of features that are relatively specific for certain disorders.
Biett's Sign in Secondary Syphilis
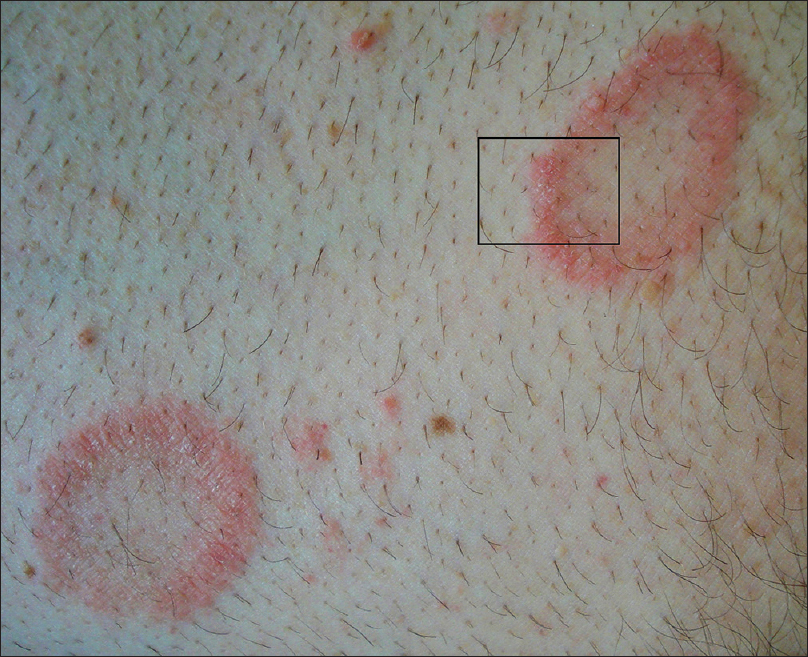
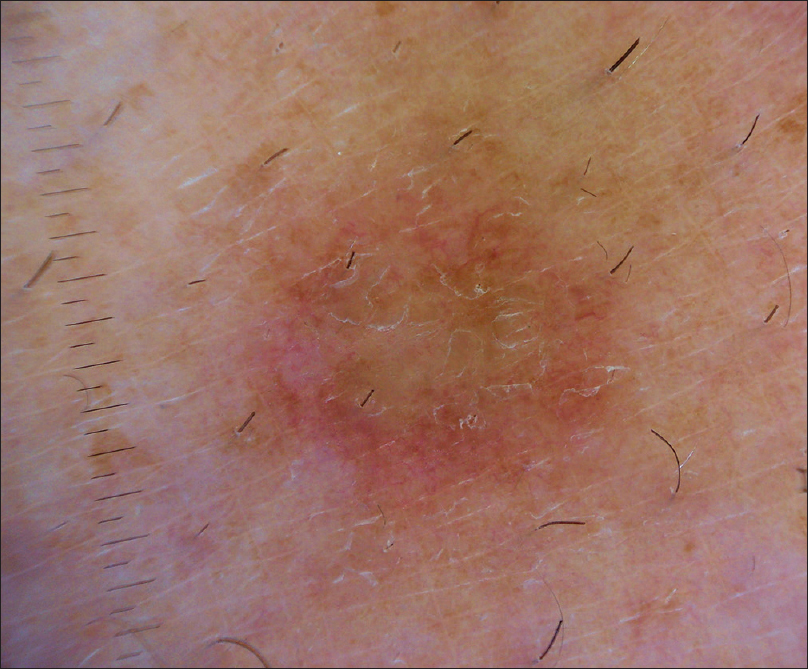
An otherwise healthy 21-year-old man presented with a 2-week history of non-pruritic maculo-papular rash involving the trunk and distal portions of the arms and legs. The rash began on the palms and soles and over 48 hours spread to involve the trunk and extremities. There was no associated fever, lethargy, headache or arthralgia. Physical examination showed erythematous, copper-colored, oval and circular macules and papules, 2–7 mm in diameter. On the palms and soles, some lesions were annular in shape with slight peripheral hyperkeratosis [Figure 1a]. Dermoscopy of the hyperkeratotic palmar lesions [Figure 1b] revealed diffuse monomorphic dotted and glomerular vessels on a diffuse, yellowish red background. A circular scaling edge (outward direction) was evident within the lesions: This appearance was interpreted as typical Biett's sign on dermoscopy, suggesting secondary syphilis. The sign was detected also in surrounding non- scaly lesions. There were no mucosal lesions, alopecia or lymphadenopathy. A venereal disease research laboratory (VDRL) test was positive at a titer of 1:640 and a Treponema pallidum hemagglutination assay (TPHA) was reactive confirming the suspicion of secondary syphilis. Penicillin G benzathine (2.4 million units) was administered intramuscularly in a single dose and the rash disappeared in 2 weeks.
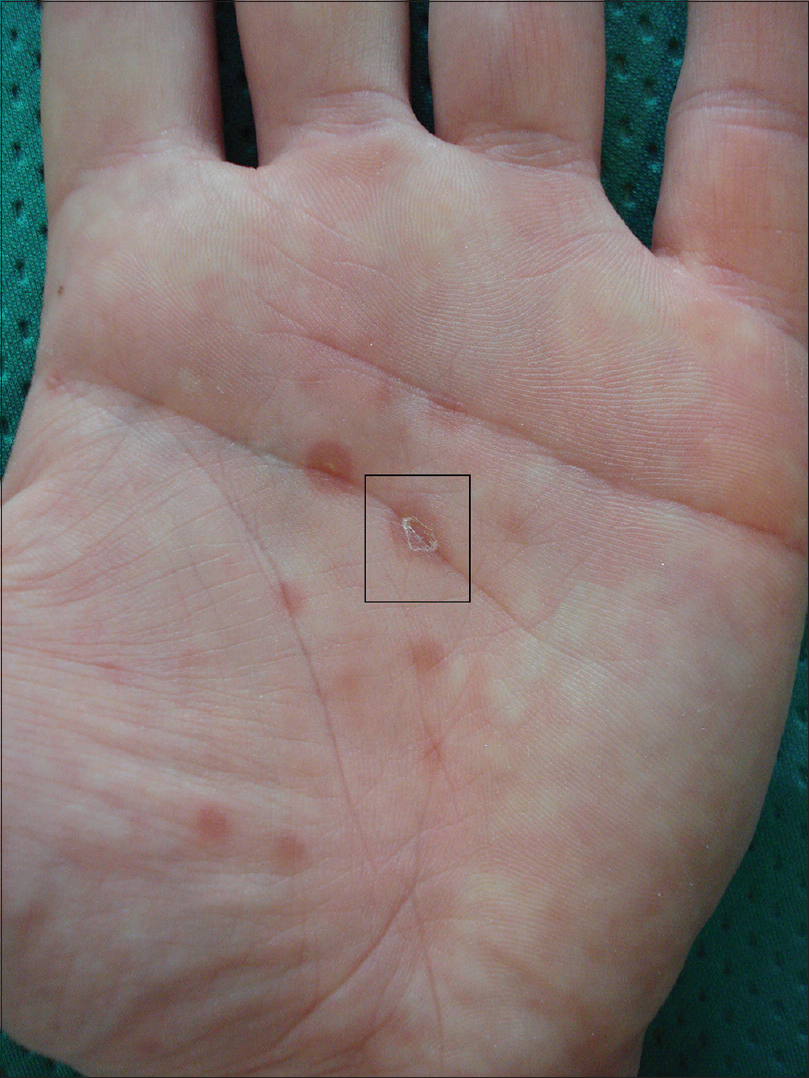 |
| Figure 1a: Maculopapular lesions of the palm in a 28-year-old man |
 |
| Figure 1b: “Biett's collarette” on dermoscopy: The central papule is encircled by a continuous homogeneous ring of scales which is surrounded by an erythematous halo; peeling is progressing in an outward direction |
Differential Diagnoses
Syphilis is known as the great mimicker due to its polymorphic appearance. Secondary syphilis has varied cutaneous features and Biett's sign is considered a strong indicator of secondary syphilis.[1]
However, many different skin diseases may have lesions with a similar annular maculo-papular erythematous morphology and scaling, e.g., pityriasis rosea of Gibert,[2],[3] actinic porokeratosis,[4] erythema annulare centrifugum,[5] granuloma annulare,[7]subacute or discoid lupus erythematosus [6] and certain annular variants of psoriasis.[3] Some of these also have palmo-plantar involvement where these need to be differentiated from from the rash of secondary syphilis. In these cases, dermoscopy makes it possible to differentiate Biett's sign of secondary syphilis from the annular scaling lesions typical of other diseases.
In darker skin, the dermoscopic features of scaling are similar but the vascular structures (and, consequently, the erythema) are usually less evident.
Actinic porokeratosis
Annular lesions of actinic porokeratosis show an irregular, thicker and more elevated collarette than Biett's sign, especially on the hands [Figure 2a]. Dermoscopic examination reveals rough, uneven scales attached at the peripheral and internal borders of the scaling edge, indicating peeling directed both inwardly and outwardly [Figure 2b].
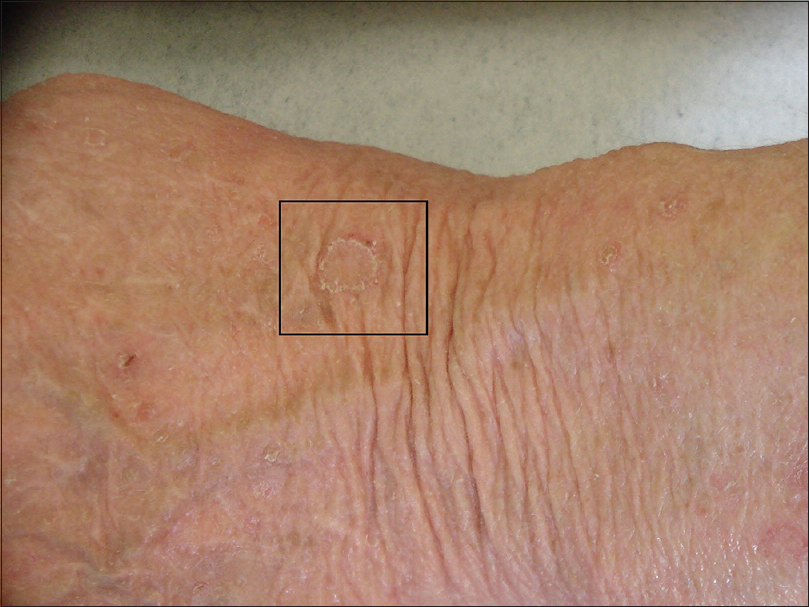 |
| Figure 2a: Actinic porokeratosis lesion in a 75-year-old woman |
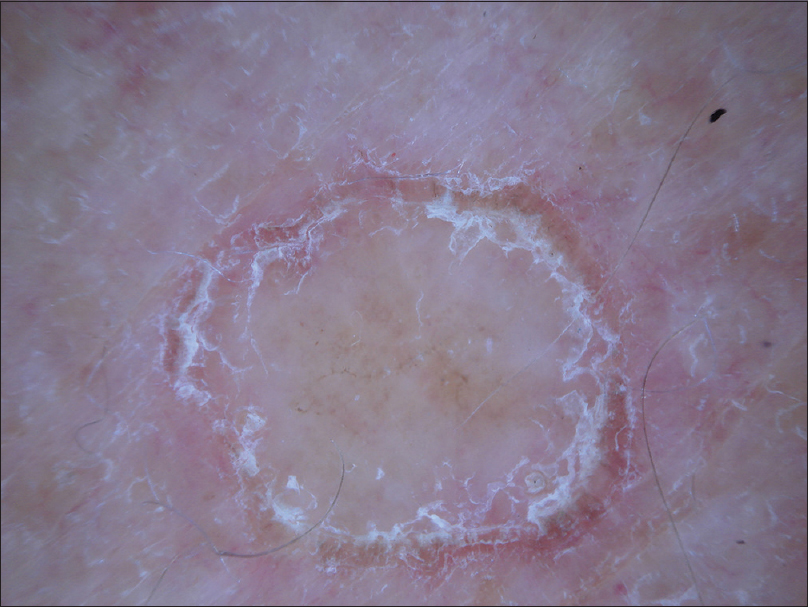 |
| Figure 2b: Dermoscopy shows a thick scaling edge with rough scales and peeling, proceeding both inwardly and outwardly |
Erythema annulare centrifugum
Homogeneous collarette scaling is also present in lesions of erythema annulare centrifugum which may manifest on both extremities and trunk. However, these scales are fine and fragile [Figure 3a] and the scaling edge appears irregular, thinner and with no clear direction of peeling when observed by dermoscopy [Figure 3b].
 |
| Figure 3a: Axillary lesion of erythema annulare centrifugum in a 43-year-old man |
 |
| Figure 3b: On dermoscopy, the scaling edge is irregular and thin, scales appear very fine with an unclear direction of peeling |
Pityriasis rosea
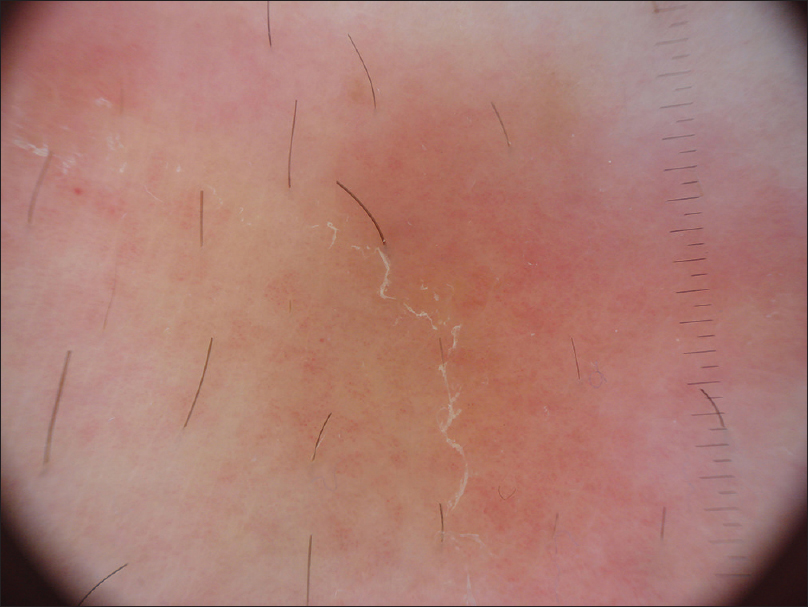
Annular lesions of pityriasis rosea usually present with a spreading erythematous border of diffuse irregular scaling [Figure 4a] which may clinically resemble a collarette. However, dermoscopic observation reveals a pattern of multiple fine fragments of scales with undefined direction [Figure 4b].[2]
 |
| Figure 4a: Annular pityriasis rosea lesions on the thigh of a 34-year-old man |
 |
| Figure 4b: On dermoscopy, lesional borders appear to have multiple fine scales with undefined direction of peeling |
Discoid lupus erythematosus
Discoid lupus erythematosus may manifest with annular to circinate lesions on the hands or as erythematous plaques with thick adherent scales [Figure 5a]. Dermoscopy highlights diffuse pink areas, arborizing vessels and irregular scales with no specific direction of peeling [Figure 5b].
 |
| Figure 5a: Subacute cutaneous lupus erythematosus on the hand of a 57-year-old woman |
 |
| Figure 5b: Dermoscopy reveals thick adherent scales covering the plaque, both peripherally and centrally, whereas no direction of scaling is evident |
Granuloma annulare
Finally, lesions of granuloma annulare can sometimes present as annular plaques with fine scaling and erythematous raised borders [Figure 6a].[7] Under dermoscopy [Figure 6b], these lesions demonstrate a non-specific diffuse scaling pattern over both the center and periphery of the lesion with no specific direction of peeling. In addition, arborizing vessels appear to be homogenously distributed all over the slightly elevated border.
 |
| Figure 6a: Granuloma annulare lesions on the leg of a 51-year-old woman: multiple annular patches with fine scaling, erythematous raised border and pale center |
 |
| Figure 6b: Dermoscopy highlights non-specific diffuse scaling pattern all over the border with arborizing vessels homogeneously arranged |
Conclusion
We underline that although dermoscopy is traditionally used for the diagnosis of skin tumors, it has also become increasingly useful as an adjunct in the clinical diagnosis of a variety of inflammatory and infectious skin, hair and scalp disorders.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Angus J, Langan SM, Stanway A, Leach IH, Littlewood SM, English JS. The many faces of secondary syphilis: A re-emergence of an old disease. Clin Exp Dermatol 2006;31:741-5.
[Google Scholar]
|
| 2. |
Chuh AA. Collarette scaling in pityriasis rosea demonstrated by digital epiluminescence dermatoscopy. Australas J Dermatol 2001;42:288-90.
[Google Scholar]
|
| 3. |
Lallas A, Giacomel J, Argenziano G, García-García B, González-Fernández D, Zalaudek I, et al. Dermoscopy in general dermatology: Practical tips for the clinician. Br J Dermatol 2014;170:514-26.
[Google Scholar]
|
| 4. |
Oiso N, Kawada A. Dermoscopic features in disseminated superficial actinic porokeratosis. Eur J Dermatol 2011;21:439-40.
[Google Scholar]
|
| 5. |
Vázquez-López F, Kreusch J, Marghoob AA. Dermoscopic semiology: Further insights into vascular features by screening a large spectrum of nontumoral skin lesions. Br J Dermatol 2004;150:226-31.
[Google Scholar]
|
| 6. |
Lallas A, Apalla Z, Lefaki I, Sotiriou E, Lazaridou E, Ioannides D, et al. Dermoscopy of discoid lupus erythematosus. Br J Dermatol 2013;168:284-8.
[Google Scholar]
|
| 7. |
Narayanasetty NK, Pai VV, Athanikar SB. Annular lesions in dermatology. Indian J Dermatol 2013;58:157.
[Google Scholar]
|
Fulltext Views
15,756
PDF downloads
2,697




