Translate this page into:
Facial involutive tumors: A case of tumor-like eosinophilic granuloma of the skin
2 Department of Pathology, Hospital Sanitas La Zarzuela, Madrid, Spain
Correspondence Address:
Elizabeth Deysy Cieza-D�az
Department of Dermatology, Hospital Sanitas La Zarzuela, Pléyades 25, CP 28023, Madrid
Spain
| How to cite this article: Cieza-D�az ED, Blanco CC, Heffernan JA, Ochaita PL. Facial involutive tumors: A case of tumor-like eosinophilic granuloma of the skin. Indian J Dermatol Venereol Leprol 2016;82:87-89 |
Sir,
The auto-involutive mucocutaneous eosinophilic dermatoses manifest as mucocutaneous lesions reactive to an unknown stimulus with a benign course and a spontaneous resolution. The histology is characterized by a dermal inflammatory infiltrate with a predominance of eosinophils.[1] The eosinophilic ulcer of the oral mucosa is the most well-known process but tumor-like eosinophilic granuloma of the skin and transient eosinophilic nodulomatosis are rare entities described in the literature.[1],[2],[3],[4]
A 42-year-old, previously healthy woman presented with a 3-week history of an asymptomatic, rapidly growing lesion on her chin. The physical examination revealed a reddish solid tumor of approximately 2 cm in diameter with central ulceration. The lesion was scheduled for a biopsy and when the patient returned 15 days later, it had completely disappeared. Instead, a new tumor with a similar appearance had appeared on her upper lip [Figure - 1]. There was no regional lymphadenopathy. She had no fever and no history of previous infections.
 |
| Figure 1: Solid red tumor of approximately 2 cm in diameter with central ulceration on the upper lip |
The differential diagnosis included malignant tumors such as keratoacanthoma or lymphoma and infectious disease caused by mycobacteria, deep mycoses or leishmania. We performed a biopsy of the tumor on the upper lip for histological and microbiological analysis. Subsequently, the tumor on the lip also began to regress spontaneously and it completely disappeared within 2 months [Figure - 2]. Skin lesions did not recur during the follow-up period of 12 months.
 |
| Figure 2: Total resolution of the lesion on the upper lip |
Histological examination revealed a reactive epidermis with irregular acanthosis without dysplasia. Dense, superficial and deep inflammatory infiltrates, comprising mostly of eosinophils, small lymphocytes, histiocytes without granulomas, neutrophils and nuclear dust were observed in the dermis [Figure - 3] and [Figure - 4]. Despite the large eosinophilic component, flame figures were not present. Immunohistochemical studies were performed to rule out the possibility of lymphoma. It revealed a variable presence of B (CD20) and T lymphocytes (CD3, CD5) with a predominance of the latter. No CD30 expression was observed. CD68 showed presence of a few macrophages with no granulomas. Periodic acid–Schiff and Ziehl–Neelsen stains were negative and intracellular leishmanial organisms were not present. Bacterial, fungal and mycobacterial cultures were negative.
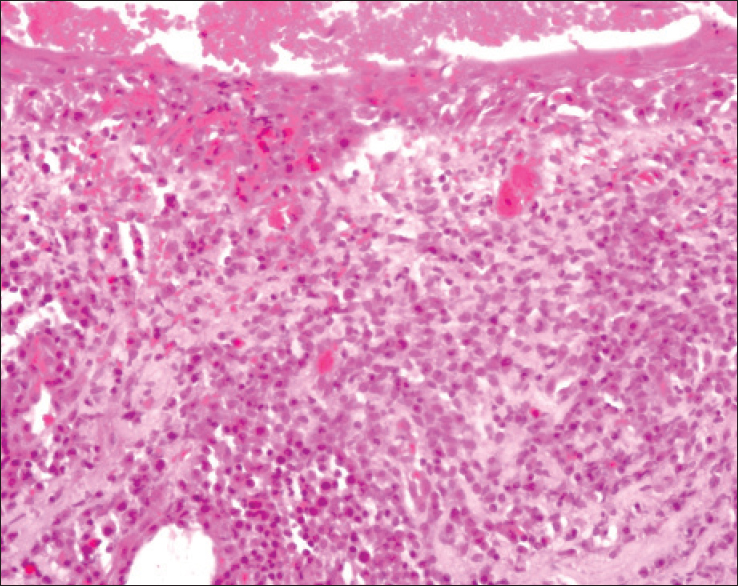 |
| Figure 3: Dense, superfi cial and deep infl ammatory infi ltrates (H and E, ×200) |
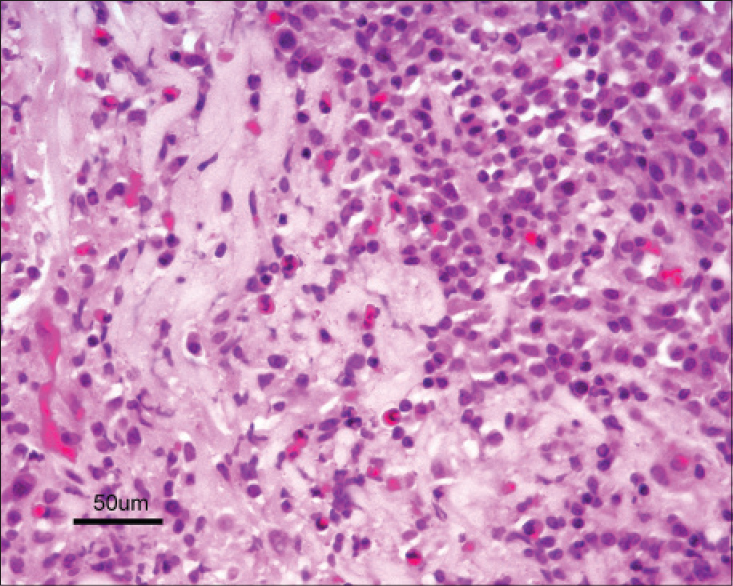 |
| Figure 4: Dermal infl ammatory infi ltrate with a large number of eosinophils (H and E, ×400) |
Blood analysis including angiotensin-converting enzyme, C-reactive protein, complements C3 and C4, antinuclear antibody (ANA) and antineutrophil cytoplasmic antibody (ANCA) were normal. The Mantoux tuberculin skin test and the chest radiograph were normal.
Skin nodules with tissue eosinophilia include auto-involutive muco-cutaneous eosinophilic dermatoses, granuloma faciale and erythema elevatum diutinum, angiolymphoid hyperplasia with eosinophilia, Well's syndrome, skin lesions of Churg–Strauss syndrome, Langerhans and non-Langerhans cell histiocytosis, malignant histiocytosis, mastocytoma and insect bite reactions.[1]
Tumor-like eosinophilic granuloma of the skin was first described in the literature in 1952 by Kuske.[3] We found only one other published report.[4] Kuske described a patient with atopic hand eczema with a rapidly growing tumor on the dorsum of the hand that disappeared spontaneously and whose etiology could not be determined. Biopsy revealed a dense dermal infiltrate composed of histiocytes and lymphocytes with numerous eosinophils.[3]
The other case was reported in 2000 by Gerbig et al.[4] A patient with a personal history of atopic dermatitis and prostate malignancy presented with two reddish-brown, solid skin tumors on his forearm and on his abdomen that resolved spontaneously 7 weeks after a curative prostatectomy. Histological examination was similar to the case described by Kuske. These authors proposed diagnostic criteria for tumor-like eosinophilic granuloma of the skin. The clinical criteria are: firm skin tumor(s) suggesting malignancy, spontaneous regression within months and no preceding infectious disease. The histological criteria are: nodular, superficial and deep dermal infiltrates consisting mainly of eosinophils, neutrophils, epithelioid cells and histiocytes; foci of necrosis with nuclear dust, no flame figures and negative stains for bacteria, mycobacteria and fungi.[4]
Based on clinical, laboratory and histological findings, our present case can be classified as Kuske's tumor-like eosinophilic granuloma of the skin according to these diagnostic criteria. Other eosinophilic dermatoses can be excluded on clinical and histopathological grounds. Transient eosinophilic nodulomatosis is clinically and histologically quite similar but it occurs mostly in children and is preceded by an infectious disease.[1],[4]
Granuloma faciale, another rare dermatoses, might have a similar histology to the present case with a dense dermal accumulation of inflammatory cells including neutrophils, eosinophils, as well as lymphocytes and histiocytes.[5] Vasculitic changes including perivascular inflammation with nuclear dust and vessel wall damage are observed. However, granuloma faciale is characterized by reddish-brown or violaceous plaques, sometimes as nodules but does not manifest as a tumor, has a chronic course and is resistant to treatment.[5]
Tumor-like eosinophilic granuloma of the skin is an infrequent entity that should be considered in the differential diagnosis of skin tumors with a predominance of eosinophils that have a benign course and spontaneous resolution. The two previously reported cases and our case all began in adult life, though there was no history of atopy in our case. The etiology of the condition is unknown but it could be considered a cutaneous hypersensitivity reaction to an unknown antigen, with or without a background of atopy.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Rodríguez Díaz E, Álvarez Cuesta V, Blanco Barrios S, Galache Osuna C, Requena Caballero C. Dermatosis eosinofílicas (I). Actas Dermosifiliogr 2003;94:65-79.
[Google Scholar]
|
| 2. |
Ada S, Seckin D, Tarhan E, Buyuklu F, Cakmak O, Arikan U. Eosinophilic ulcer of the tongue. Australas J Dermatol 2007;48:248-50.
[Google Scholar]
|
| 3. |
Kuske H. Tumorfoermige eosinophile granulome der haut. Dermatologica 1952;104:254-9.
[Google Scholar]
|
| 4. |
Gerbig AW, Zala L, Hunziker T. Tumorlike eosinophilic granuloma of the skin. Am J Dermatopathol 2000;22:75-8.
[Google Scholar]
|
| 5. |
Ortonne N, Wechsler J, Bagot M, Grosshans E, Cribier B. Granuloma faciale: A clinicopathologic study of 66 patients. J Am Acad Dermatol 2005;53:1002-9.
[Google Scholar]
|
Fulltext Views
5,071
PDF downloads
1,688





![[Figure - 1]](#fig_ijdvl_2016_82_1_87_172906_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_1_87_172906_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2016_82_1_87_172906_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2016_82_1_87_172906_f4.jpg){kind=link}