Translate this page into:
Kimura's disease in an old case of leprosy
Correspondence Address:
Debeeka Hazarika
Urbashium, House No 10, Shantipur, Guwahati - 781 009, Assam
India
| How to cite this article: Hazarika D, Jahan N, Das AK. Kimura's disease in an old case of leprosy. Indian J Dermatol Venereol Leprol 2016;82:535-536 |
Sir,
Kimura's disease is a rare disorder mostly affecting young adult males of Asian origin. It presents as asymptomatic subcutaneous nodules and plaques over the head and neck with lymphadenopathy and salivary gland swelling. Tissue and blood eosinophilia and high serum immunoglobulin E levels are the other features.
A 32-year-old man presented with soft, painless, subcutaneous swellings over the face and right ear lobe. These began 2 years ago as small lesions over the left temporal region and cheek gradually increased in size, and new lesions appeared on the other side of face. There was no history of fever, joint pain or weight loss. Ten years back he was treated for multibacillary leprosy with ulcerative erythema nodosum leprosum. At presentation he had residual hypopigmented patches and thickened peripheral nerves. Deformities of hands and feet, collapsed nasal bridge, bilateral madarosis and scars were present as sequelae of the disease.
General physical and systemic examinations were normal. There were multiple nodules of varying size (5-9 cm) distributed over the left side of face, right cheek and ear lobe. The nodules were smooth, soft, mobile and non-tender with normal overlying skin [Figure - 1]a and b. Mucosal surfaces were normal. He had bilateral cervical lymphadenopathy with discrete, soft to firm, mobile and non-tender lymph nodes.
 |
| Figure 1: (a and b) Skin coloured nodular swelling over cheeks extending up to mandibular area with atrophic scars on face and nasal deformity |
The initial differential diagnoses were multicentric reticulohistiocytosis, Kimura's disease, angiolymphoid hyperplasia with eosinophilia, B-cell lymphoma and lipoma. Other possibilities considered were bacillary angiomatosis, pinta and granuloma faciale. Investigations revealed a total leucocyte count of 7650 cells/mm 3 with a differential eosinophil count of 20.9% and raised serum immunoglobulin E (100-300 IU/ml). Total urinary protein was marginally raised, 126 mg/24 hours. Slit skin smear was negative. Other laboratory parameters and radiographic screening were within nomal limits.
Ultrasonography of face and neck area revealed subcutaneous soft tissue swellings, bulky parotids and submandibular salivary glands as well as intra-parotid and cervical lymph node enlargement. Fine needle aspiration cytology from the swellings and glands was inconclusive.
A deep incisional biopsy from a facial nodule showed dermal and subcutaneous fibrosis with mixed chronic inflammatory cells mainly lymphocytes, plasma cells and plenty of eosinophils. There were focal eosinophilic abscesses [Figure - 2]a. Small lymphoid aggregates and proliferating blood vessels lined by flat endothelial cells were seen [Figure - 2]b.
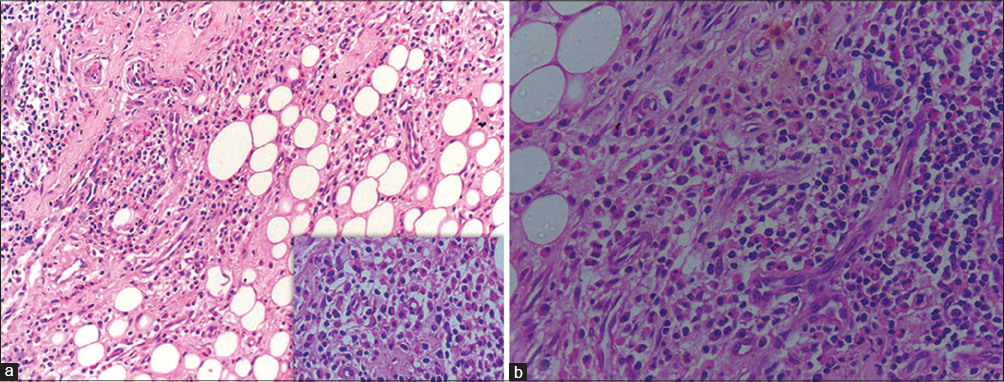 |
| Figure 2: (a) Infiltrates of eosinophils and lymphocytes are seen in a fibrous stroma, at places forming eosinophilic microabscesses (inset) [H and E ×100, ×400 (inset)] (b) Small lymphoid aggregates and proliferation of blood vessels are seen lined by flat endothelial cells (H and E, ×400) |
The clinical features, laboratory parameters and histopathological findings were consistent with the diagnosis of Kimura's disease.
The first clinical description of Kimura's disease appeared in the Chinese literature (1937) and the first histopathological description was given by Kimura et al. (1948).[1] It is a rare disorder, presenting with asymptomatic deep seated nodules, commonly located over the head and neck region. Often, there is involvement of salivary glands and lymph nodes. Peripheral blood eosinophilia, high serum immunoglobulin E and renal involvement may be present.[1],[2] The disease runs a chronic, relapsing course. Histopathological findings are obvious in the deep dermis or subcutis; there is a fibrous stroma with cellular infiltrate mostly composed of eosinophils and lymphocytes. Eosinophilic infiltration may be dense enough to form abscesses. Vascular channels are present in abundance.
Angiolymphoid hyperplasia with eosinophilia is a histopathological differential diagnosis of Kimura's disease because of coexisting tissue eosinophilia and vascular proliferation. However, clinically it is characterized by more superficial circumscribed nodules or plaques particularly along the hairline and peri-auricular area. Lymphadenopathy, salivary gland involvement, blood eosinophilia and raised serum immunoglobulin E are usually absent.[2] Histopathologically, the vascular proliferation is more prominent, lined by plump epithelioid endothelial cells.[3] Eosinophilic abscesses are very rare in angiolymphoid hyperplasia.[3],[4] Other causes of facial nodules and plaques such as multicentric reticulohistiocytosis, granuloma faciale, lymphoma, lipoma, bacillary angiomatosis and lepromatous leprosy can be excluded clinically and histopathologically.
Kimura's disease is a rare disorder and its occurrence in a treated case of leprosy posed a diagnostic challenge, though the association was probably coincidental.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Larroche C, Bletry O. Kimura's disease. Orphanet encyclopedia. February 2005. Available from: http://www.orpha.net/data/patho/GB/uk-kimura.pdf. [Last accessed on 2014 Oct 01].
[Google Scholar]
|
| 2. |
Chong WS, Thomas A, Goh CL. Kimura's disease and angiolymphoid hyperplasia with eosinophilia: Two disease entities in the same patient. Case report and review of literature. Int J Dermatol 2006;45:139-45.
[Google Scholar]
|
| 3. |
Liu XK, Ren J, Wang XH, Li XS, Zhang HP, Zeng K. Angiolymphoid hyperplasia with eosinophilia and Kimura's disease coexisting in the same patient: Evidence for a spectrum of disease. Austral J Dermatol 2012;57:47-50.
[Google Scholar]
|
| 4. |
Shahryari J, Dabiri S, Talebi A. Kimura's disease: A case report and review of literatures. Iran J Pathol 2012;7:251-5.
[Google Scholar]
|
Fulltext Views
3,612
PDF downloads
1,563





![[Figure - 1]](#fig_ijdvl_2016_82_5_535_182978_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_5_535_182978_f2.jpg){kind=link}