Translate this page into:
Actinic keratosis arising in an epidermal cyst
2 Department of Pathology, Mackay Memorial Hospital, Hsinchu Branch, Hsinchu, Taiwan
3 Department of Dermatology, Mackay Memorial Hospital, Taipei, Taiwan
Correspondence Address:
Yu-Hung Wu
Department of Dermatology, Mackay Memorial Hospital, 92, Sec. 2, Zhongshan North Road, Taipei 10449
Taiwan
| How to cite this article: Loganathan E, Chang KM, Wu YH. Actinic keratosis arising in an epidermal cyst. Indian J Dermatol Venereol Leprol 2020;86:411-413 |
Sir,
Actinic keratosis is a common skin tumor which occurs on sites chronically exposed to sun, such as the face, scalp, neck and forearms. There is an increased incidence of actinic keratosis with age, lighter skin color and chronic sun exposure. Actinic keratosis evolves in stages from individual UV-damaged keratinocytes, subclinical nonvisible lesions, early and late lesions and if untreated, may evolves as an invasive sqamous cell carcinoma. Histopathologically, there is keratinocyte pleomorphism and architectural changes as well as nuclear morphometric alterations at the basal and supra basal areas of the epidermis on a background of photodamage such as atrophy and solar elastosis in the dermis.[1]
An epidermal cyst develops from the infundibular part of the hair follicle; therefore, it is also called as infundibular cyst or epidermal inclusion cyst. Herein, we report an unusual case of an epidermal cyst with focal change of actinic keratosis.
A 78-year old Taiwanese woman of Fitzpatrick 3 skin type, presented with an asymptomatic skin lesion on the left cheek which existed for many years and gradually increased in size. On examination, it was a nodular lesion about 1.5 cm in size with scaling and yellowish crusts [Figure - 1]. The lesion was completely excised and the specimen was sectioned into four pieces. In one piece, there were typical findings of actinic keratosis that showed hyperkeratosis, parakeratosis, irregular acanthosis and proliferation of atypical keratinocytes in the lower epidermis [Figure - 2]a and [Figure - 2]b. The other sections demonstrated a dermal cystic lesion expanding to the subcutis, filled with keratinous material and mainly lined by stratified squamous epithelium with a granular layer which indicated a typical epidermal cyst [Figure - 3]a. The cyst lining in the deep portion, close to subcutis, revealed areas of atypical proliferation of keratinocytes. These keratinocytes had abundant glassy cytoplasm, forming multiple short blunt extensions with nuclear atypia in the lower portion of cyst membrane as seen in actinic keratosis [Figure - 3]b, [Figure - 3]c, [Figure - 3]d, [Figure - 3]e. The proliferating keratinocytes in the basal-suprabasal layers had a mild increase of proliferative index under immunohistochemistry stain for Ki-67 and some of them frankly stained with p16. The overall features suggested an actinic keratotic change of a portion of the epidermal cyst. The surgical margins were free of tumor involvement.
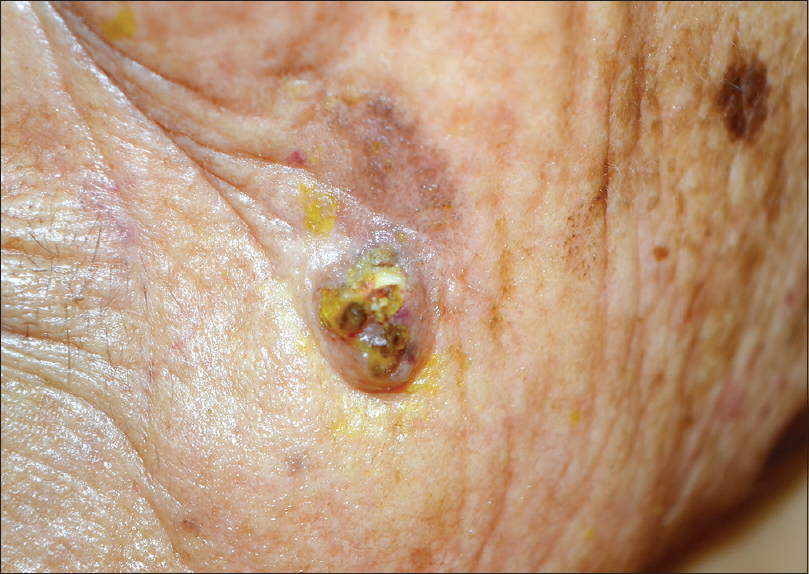 |
| Figure 1: A nodular lesion measuring about 1.5 cm in size with scaling and yellowish crusts on the left che |
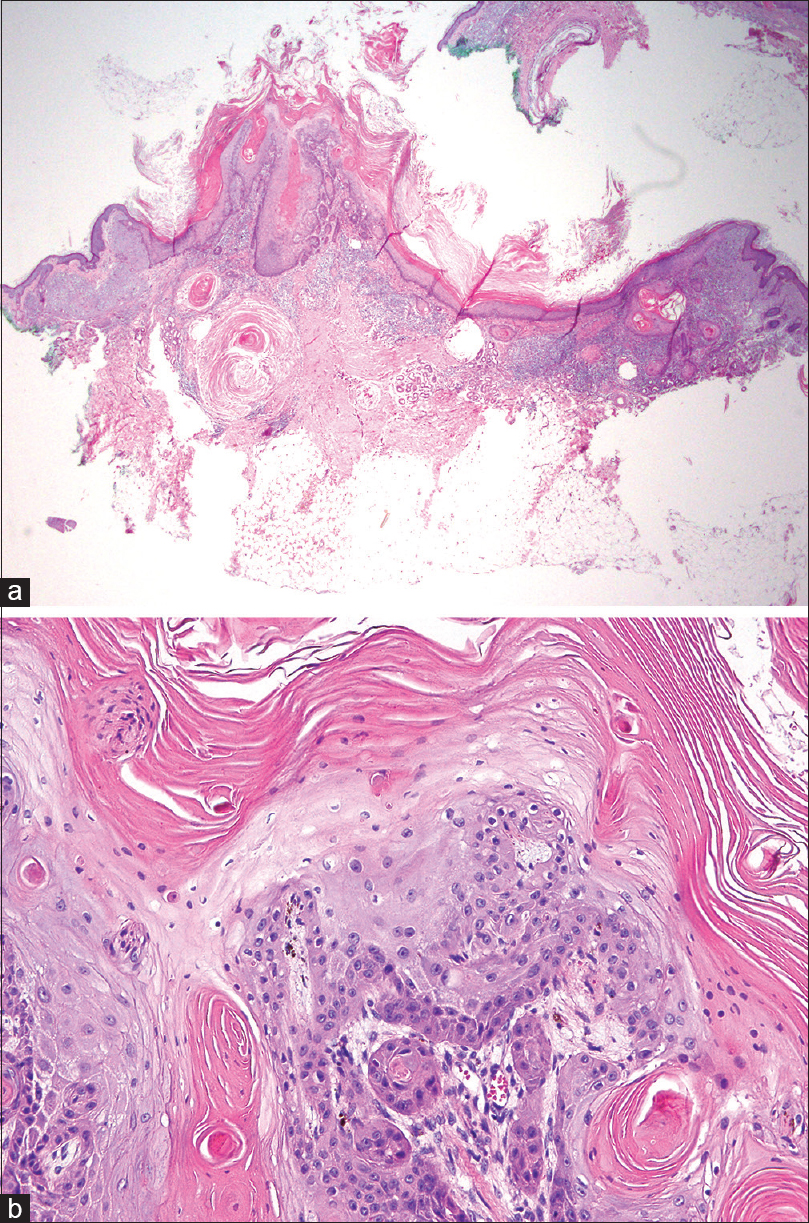 |
| Figure 2: One section showed typical findings of actinic keratosis featured by hyperkeratosis, parakeratosis and irregularly proliferation of atypical keratinocytes in the lower epidermis (a) (H and E, 4×), (b) (H and E, 40×) |
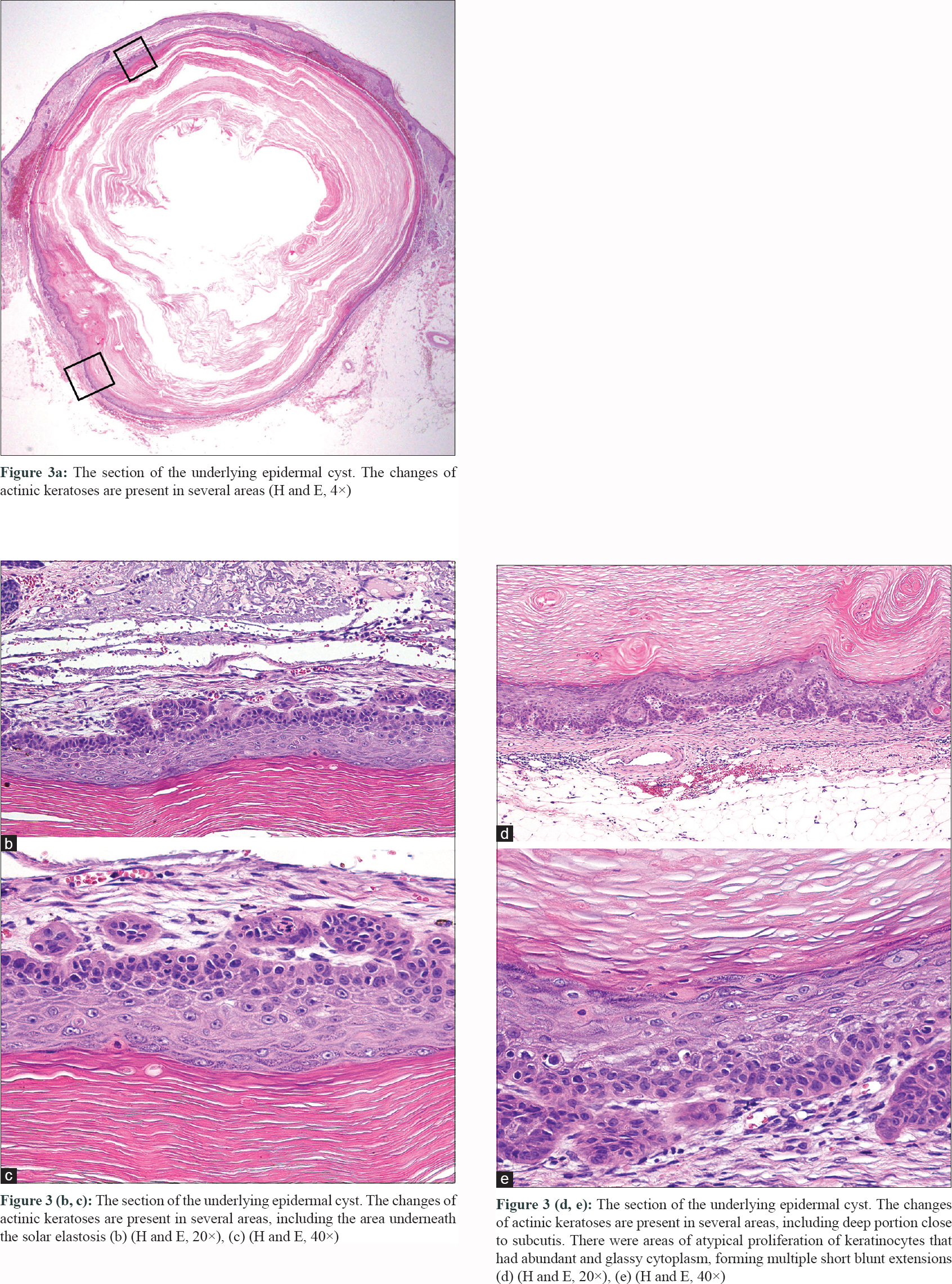 |
| Figure 3: |
Epidermal cysts are very common lesions, but development of actinic keratosis on them is a very rare occurrence. Sometimes, actinic keratosis may show a downward extension into the hair follicle.[2] This finding was also present in our patient [Figure - 2]a. Since there is a possibility of common origin from the infundibular portion of the hair follicle, we can establish a link between the epidermal cysts and malignant changes, like actinic keratosis, in this case. Based on available literature till date, cases of well documented sqamous cell carcinoma arising from epidermal cysts have an incidence ranging from 0.01–0.05%.[3] The proposed mechanism of malignant change seen in epidermal cysts could be chronic inflammation due to direct trauma, recurrent irritation, human papillomavirus, immunosuppression and actinic damage.[4] In our case report, ultraviolet damage could have been the precipitating factor as it was present on a chronically sun damaged skin.
Epidermal cysts presenting with pain, rapid growth or overlying skin changes such as ulceration or persistent drainage should be considered as warning signs and must be completely excised. There are possibilities of missing a malignant change because of simple bisection of the cyst and therefore, thorough sectioning is advised whenever in suspicion.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understand that name and initials will not be published, and due efforts will be made to conceal identity but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Figueras Nart I, Cerio R, Dirschka T, Dréno B, Lear JT, Pellacani G, et al. Defining the actinic keratosis field: A literature review and discussion. J Eur Acad Dermatol Venereol 2018;32:544-63.
[Google Scholar]
|
| 2. |
Fernández-Figueras MT, Saenz-Sardà X, Vargas P, Thompson CT, Carrato C, Puig L, et al. The depth of follicular extension in actinic keratosis correlates with the depth of invasion in squamous cell carcinoma: Implication for clinical treatment. J Eur Acad Dermatol Venereol 2018;32:1657-61.
[Google Scholar]
|
| 3. |
Morgan MB, Stevens GL, Somach S, Tannenbaum M. Carcinoma arising in epidermoid cyst: A case series and aetiological investigation of human papillomavirus. Br J Dermatol 2001;145:505-6.
[Google Scholar]
|
| 4. |
Sze S, Richmond I, Bickers A, Saha A. Squamous cell carcinoma arising from a vulval epidermal cyst. J Obstet Gynaecol Res 2016;42:1623-6.
[Google Scholar]
|
Fulltext Views
4,119
PDF downloads
2,579





![[Figure - 1]](#fig_ijdvl_2020_86_4_411_284949_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2020_86_4_411_284949_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2020_86_4_411_284949_f3.jpg){kind=link}