Translate this page into:
Dermoscopic features of a case of solitary reticulohistiocytoma
2 Department of Dermatology, Venereology and Leprolog, JIPMER, Puducherry, India
3 North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, Meghalaya, India
4 Department of Pathology, JIPMER, Puducherry, India
Correspondence Address:
Rashmi Kumari
Department of Dermatology, Venereology and Leprology, JIPMER, Puducherry - 605 006
India
| How to cite this article: Behera B, Kumari R, Thappa DM, Gochhait D. Dermoscopic features of a case of solitary reticulohistiocytoma. Indian J Dermatol Venereol Leprol 2020;86:435-438 |
Sir,
A 44-year-old man presented with a 6-month history of a gradually enlarging, solitary, asymptomatic swelling on the right side of the upper lip. He had accidentally excoriated the surface of the lesion. He denied any history of associated joint pain or swelling or any other systemic complaints. Cutaneous examination revealed a solitary, well-circumscribed, dome-shaped, firm, erythematous, non-tender nodule measuring 0.5 cm × 0.5 cm, with surface erosion on the right side of the upper lip [Figure - 1]. Other cutaneous and systemic examinations were within normal limits. A differential diagnosis of nodular hidradenoma, solitary reticulohistiocytoma and pedunculated encapsulated neuroma was considered. A complete hemogram, liver function test, renal function test, fasting lipid profile and sugar profiles were within normal limits. Dermoscopic examination under non-polarized contact dermoscopy (HEINE DELTA20® Dermatoscope, 10 × magnification) revealed a central crater-like area with overlying blood spots, shiny pink-white areas, different shades of yellow homogenous areas which were out of focus and the presence of crown vessels [Figure - 2]. Interestingly, in the area of surface erosion, the yellow homogenous area was more prominent and in focus. The lesion was completely excised, and histopathological examination revealed orthohyperkeratosis, normal to thinned out stratum spinosum, pan-dermal infiltration of epithelioid histiocytes with a large vesicular nucleus and eosinophilic ground glass cytoplasm, admixed with multinucleated giant cells, lymphocytes and few eosinophils [Figure - 3]. On immunohistochemistry, the histiocytes were positive for leukocyte common antigen, CD68 [Figure - 4] and negative for S100 and CD1a. A diagnosis of solitary reticulohistiocytoma was made, and the patient was followed up for 1 year without any sign of recurrence.
 |
| Figure 1: Solitary, well-circumscribed, dome-shaped erythematous nodule with surface erosion on the right side of the upper lip |
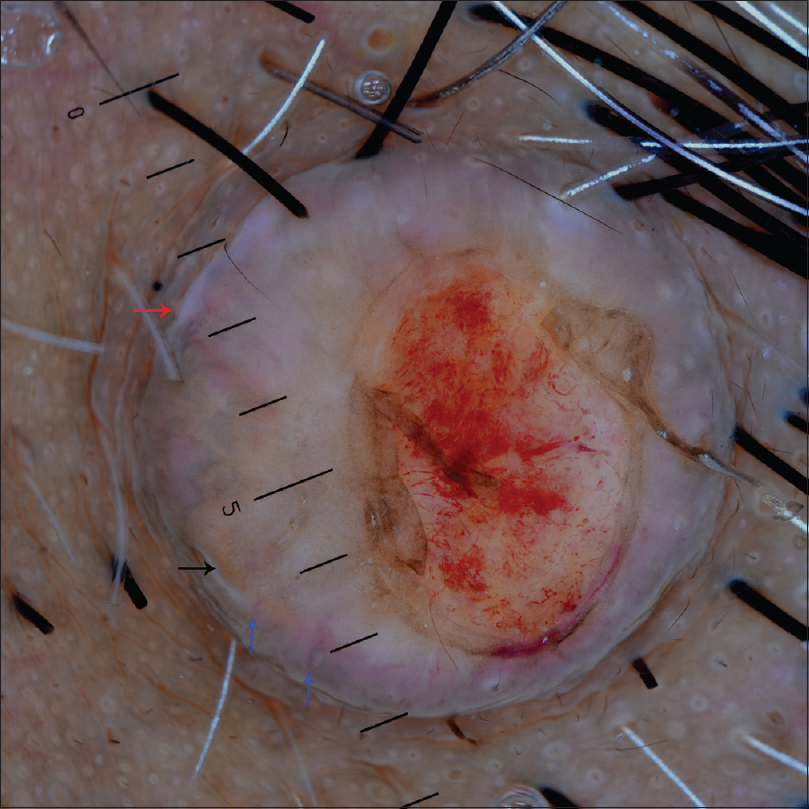 |
| Figure 2: Dermoscopic examination under non-polarized contact dermoscopy (HEINE DELTA20® Dermatoscope, 10×), showing a central crater-like area with overlying blood spots, shiny pink-white areas (red arrow), different shades of out of focus yellow homogenous areas, and crown vessels (blue arrows). The yellow homogenous area is in focus and more prominent in the eroded area |
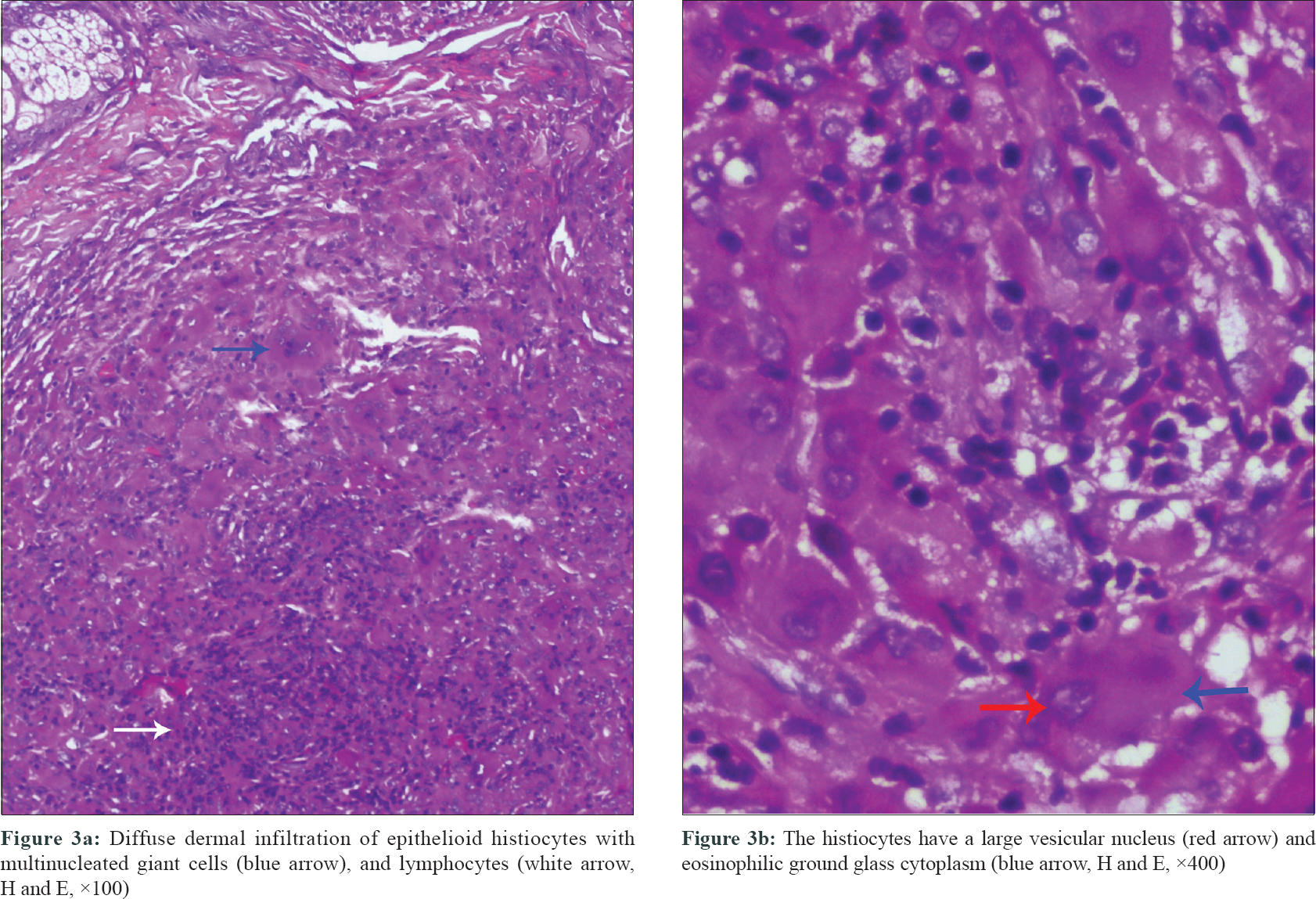 |
| Figure 3: |
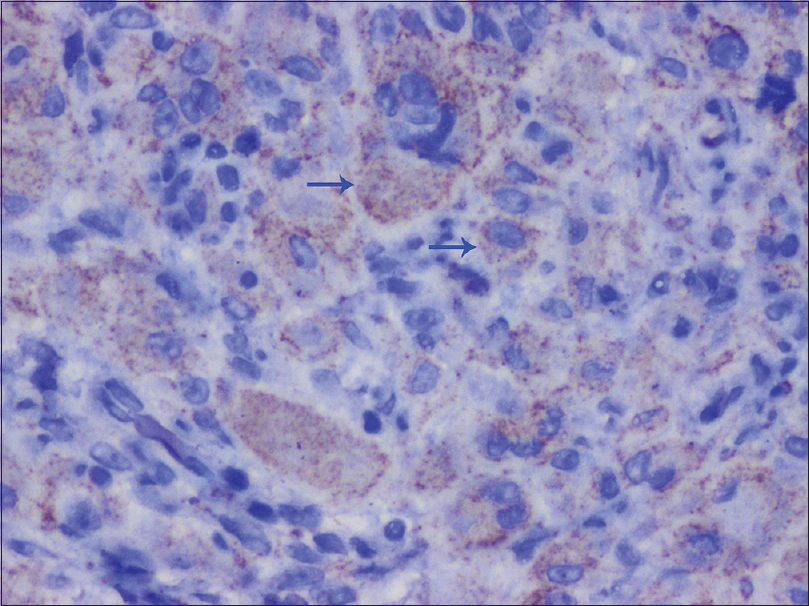 |
| Figure 4: The histiocytes staining positive for CD68 (arrows, immunohistochemistry, ×400) |
Solitary reticulohistiocytoma is a type of non-Langerhans cell histiocytosis that usually presents as a solitary, asymptomatic, firm, smooth-surfaced reddish-brown to yellow papule or nodule of size less than 1 cm. It commonly occurs in young adult males. Trunk and extremities are the favored sites.[1] Clinical diagnosis of solitary reticulohistiocytoma is quite challenging, as it can mimic other solitary cutaneous lesions like nodular hidradenoma, solitary trichoepithelioma, solitary neurofibroma, pedunculated encapsulated neuroma, basal cell carcinoma, etc.
Dermoscopy is increasingly used in clinical practice to aid in the diagnosis of various dermatosis. It reflects the histopathological findings of the epidermis and upper dermis of a cutaneous lesion. Dermoscopy has been successfully used in the diagnosis of solitary reticulohistiocytoma as it is clinically difficult to distinguish it from other solitary cutaneous nodules. A characteristic “setting sun” appearance defined as a central orange-yellow area and a peripheral erythematous ring has been described as a dermoscopic sign for solitary reticulohistiocytoma.[1] A yellow-pink background with crown and arborizing vessels has also been reported.[1],[2] Paolino et al. described a central yellowish area admixed with coiled vessels surrounded by an erythematous background.[2] In all the above reports, the yellow homogenous area was a constant dermoscopic feature of reticulohistiocytoma, which reflects the xanthomized dermal histiocytes. In our case, the yellow homogenous areas were out of focus and were overshadowed by the shiny pink-white areas. Due to the surface erosion, the yellow homogenous area was more prominent and in focus, thus pointing to the xanthomatous nature of the lesion. Three dermoscopic patterns were described in a patient of cutaneous reticulohistiocytosis having 29 lesions; different shades of the yellow homogenous area alone, with a brown reticular structure or with central white scar-like patches and streaks.[1] Dermoscopic features described for solitary reticulohistiocytoma without having yellow homogenous area are a central white-grayish area and peripheral white-pinkish streaks and a homogenous pink coloration with superficial white scales.[1],[3]
Dermoscopic differential diagnosis of our case were adult xanthogranuloma (yellowish-orange hue with arborizing vessels), xanthomatous dermatofibroma (yellow homogeneous area), sebaceous adenoma/sebaceoma (homogenous yellowish hue and crown vessels), sebaceous carcinoma (yellow homogenous area, polymorphous vascular pattern and rarely ulceration) and keratoacanthoma (keratin, white circles, blood spots and white structureless zones).[4],[5] The central crater-like area with overlying red blood spots corresponds to the traumatic erosion and hemorrhage, the yellow area to the xanthomized histiocytes, the white areas to the hyperkeratosis and the crown vessels to the peripheral dilated blood vessels. The presence of large epithelioid histiocytes with eosinophilic glassy cytoplasm thought to be very characteristic of solitary reticulohistiocytoma, helps in differentiating it from other clinical mimics. Cells are CD68 and CD163 positive and negative for CD1a and S100. The treatment of choice is surgical excision.
In conclusion, we are reporting the dermoscopic features of a case of solitary reticulohistiocytoma and discussing how an accidental surface erosion helped in unfolding the dermal dermoscopic features.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal the identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Behera B, Chandrashekar L, Gochhait D, Gupta D, Thappa DM. Crown vessels and follicular white dot: New dermoscopic findings in a case of solitary reticulohistiocytoma. J Am Acad Dermatol 2018;78:e57-9.
[Google Scholar]
|
| 2. |
Paolino G, Cota C, Giona F, Donati P, Lora V, Moliterni E, et al. The different dermoscopic features of the yellow background in Langerhans and non-Langerhans cells histiocytosis. Clin Exp Dermatol 2017;42:679-82.
[Google Scholar]
|
| 3. |
Kieselova K, Santiago F, Amado C, Henrique M. Case for diagnosis. Solitary violaceous nodule on the toe. An Bras Dermatol 2018;93:595-7.
[Google Scholar]
|
| 4. |
Bañuls J, Arribas P, Berbegal L, DeLeón FJ, Francés L, Zaballos P. Yellow and orange in cutaneous lesions: Clinical and dermoscopic data. J Eur Acad Dermatol Venereol 2015;29:2317-25.
[Google Scholar]
|
| 5. |
Rosendahl C, Cameron A, Argenziano G, Zalaudek I, Tschandl P, Kittler H. Dermoscopy of squamous cell carcinoma and keratoacanthoma. Arch Dermatol 2012;148:1386-92.
[Google Scholar]
|
Fulltext Views
3,055
PDF downloads
2,055





![[Figure - 1]](#fig_ijdvl_2020_86_4_435_284713_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2020_86_4_435_284713_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2020_86_4_435_284713_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2020_86_4_435_284713_f4.jpg){kind=link}