
Translate this page into:
Analysis of symmetricity in the three different (sagittal, transverse and frontal) planes in generalized nonsegmental vitiligo
Corresponding author: Prof. Khadiga S. Sayed, 5th Settlement, New Cairo, Egypt. diga1980@kasralainy.edu.eg
-
Received: ,
Accepted: ,
How to cite this article: Anbar T, Abdel Hay RM, Hegazy RA, Esmat S, Diab HM, Amer H, et al. Analysis of symmetricity in the three different (sagittal, transverse and frontal) planes in generalized nonsegmental vitiligo. Indian J Dermatol Venereol Leprol 2021;87:22-8.
Abstract
Background:
Nonsegmental vitiligo is defined as being “often symmetrical”, however, no work has tackled the point as to how valid it is to depend upon the concept of symmetricity in generalized nonsegmental vitiligo.
Aims:
To investigate vitiligo symmetry, taking into account sites of predilection, the clinical characteristics of patients were studied.
Methods:
This multicentric study included 712 nonsegmental vitiligo patients with 2876 examined lesions. Three models were drawn for each patient. Sagittal, transverse and frontal planes were drawn to divide the body into right/left, upper/lower and anterior/posterior halves respectively. Patients were examined by Wood’s light and analyzed for symmetry.
Results:
Bilateral involvement was present in 78% (P < 0.001). Studying the similarity of clinical involvement in the upper and lower body parts revealed that such similarity was present in 38%, with a significant positive association in some areas. Studying clinical similarity in the anteroposterior distribution pattern revealed a significant positive association in 11%.
Limitations:
Relatively low number of patients.
Conclusions:
We found significant bilateral symmetry in the lesions of 78% of vitiligo patients. Our work could aid in drawing the anticipated vitiligo map in patients with active disease, helping in increasing our understanding of the clinical behaviour of this disease.
Keywords
Distribution
predilection
symmetry
vitiligo

Introduction
Vitiligo is a chronic and highly recognizable skin disease that often leads to a decrease in quality of life.1 Even though many efforts have been made to acquire a deeper understanding of the pathophysiology of vitiligo, it remains enigmatic in many aspects. Its precise cause is unknown with multiple theories being proposed: chiefly those based on autoimmune, neural and autocytotoxic phenomena.2
The course and distribution pattern of generalized nonsegmental vitiligo is unpredictable.3 The determination of the anticipated clinical phenotype and evolution pattern of vitiligo in the individual patient is a dream, which if fulfilled, might aid in predicting the site of the next attack. Prophylaxis can be then integrated into the treatment plans for each patient.
Nonsegmental vitiligo has been described to mainly involve the face (periorificial), dorsal surface of the hands, nipples, axillae, umbilicus, sacrum and inguinal/ anogenital regions. On extremities, it has been shown to favor the elbows, knees, digits and flexor wrists.4 Taieb and Picardo,5 described sites of predilection of generalized nonsegmental vitiligo to coincide with areas more prone to the occurrence of the Koebner phenomenon.5 A recent work highlighted the fact that the distribution pattern might depend on several clinical characteristics such as age (age of patient and age of disease onset), gender and duration of disease.6
Furthermore, the Vitiligo European Task Force (VETF) defines nonsegmental vitiligo as being “often symmetrical”; however, no work has tackled the point as to how valid it is to depend upon the concept of symmetricity in generalized nonsegmental vitiligo to draw the individualized map of vitiligo in each patient.7 Therefore, in this study we aimed to investigate this concept of “symmetry” of vitiligo lesions, taking into account previously described sites of predilection. Furthermore, we studied other clinical characteristics of the included generalized nonsegmental vitiligo patients in relation to this concept, in an attempt to de-mystify this intriguing disease.
Methods
This multicentric study was approved by the local Dermatology Research Ethics Committee Office. Generalized nonsegmental vitiligo patients were collected consecutively from the dermatology outpatient clinics of Kasralainy teaching hospitals, Ain Shams University, Hod El Marsoud Hospital, Al Minya University and Al Fayoum University.
All patients were examined by dermatologists and patients were included if they satisfied the definition of generalized nonsegmental vitiligo.7
A detailed history was retrieved from each patient through a questionnaire to document their age and sex, the presence of a positive family history in a first-degree relative, as well as the duration and course of the disease based on the Vitiligo Disease Activity Score.8 Personal and family history of autoimmune diseases (thyroid disease, diabetes mellitus type 1, alopecia areata, psoriasis, pernicious anemia, rheumatoid arthritis and systemic lupus erythematosus and Addison disease) were also assessed.6
Three models were drawn for each patient, in which sagittal, transverse and frontal (coronal) planes were drawn to divide the body into right/left, upper/lower and anterior/posterior halves, respectively. Included patients were thoroughly examined by Wood’s light and the lesions drawn in the three models were analyzed for symmetricity.
Statistical analysis
Data were statistically described in terms of range, mean ± standard deviation, or frequencies (number of cases) and percentages when appropriate. For comparing categorical data, Chi-square (χ2) test was performed. The exact test was used when the expected frequency was less than 5. Correlation between various variables was found using the Spearman rank correlation equation for non-linear relation. P values of less than 0.05 were considered statistically significant. All statistical calculations were done using computer program Statistical Package for the Social Science (SPSS Inc., Chicago, IL, USA) release 15 for Microsoft Windows (2006).
Results
This multicentric study included 712 nonsegmental vitiligo patients in whom 2876 lesions were examined. Their age ranged from 5 to 65 years with mean ± standard deviation 31.54 ± 15.437 years. There were 271 (38%) males and 441 (62%) females. The duration of disease ranged from 0.08 to 12 years with mean ± standard deviation 9.61 ± 19.243 years. The clinical and demographic data of patients is included in Table 1.
| Data | Results |
|---|---|
| Age/years, range (mean±SD) | 5-65 (31.54±15.44) |
| Sex (male/female), n (%) | 271 (38)/441 (62) |
| Disease duration/years, range (mean±SD) | 0.08-12 (9.61±19.24) |
| Course of the disease(VIDA score), n (%) | |
| 0 | 75 (10.6) |
| +1 | 106 (14.8) |
| +2 | 126 (17.7) |
| +3 | 120 (16.9) |
| +4 | 285 (40) |
| Family history of vitiligo, n (%) | |
| Present | 252 (35.4) |
| Absent | 460 (64.6) |
| Associated autoimmune disease, n (%) | |
| Present | 70 (9.8) |
| Absent | 642 (90.2) |
| Family history of autoimmune disease, n (%) | |
| Present | 48 (6.7) |
| Absent | 664 (93.3) |
SD: Standard deviation, VIDA: Vitiligo disease activity
Bilateral distribution across the sagittal plane
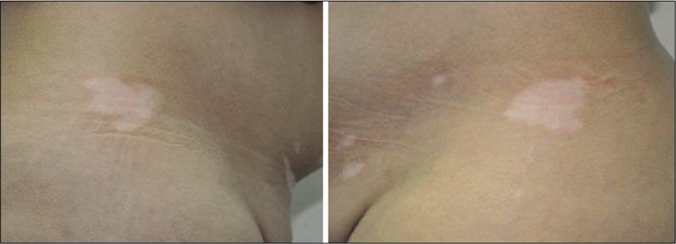
Studying the clinical symmetry of the affected lesions revealed that bilateral involvement was present in 78% (n = 555) of patients. This figure was statistically significant (P < 0.001). All studied areas, apart from the shoulders, revealed the statistically significant positive occurrence of bilateral symmetry [Table 2]. The prevalence of bilateral distribution in different body sites is demonstrated in Table 2 and Figures 1-4.
| Studied association | Positive association, n (%) | Negative association, n (%) | P | |
|---|---|---|---|---|
| Right side forehead | Left side forehead | 93/110 (84.5) | 17/110 (15.5) | <0.001* |
| Right side nose | Left side nose | 36/36 (100) | 0 | <0.001* |
| Right eyelid | Left eyelid | 93/160 (58.1) | 67/160 (41.2) | <0.001* |
| Right periauricular | Left periauricular | 28/28 (100) | 0 | <0.001* |
| Right postauricular | Left postauricular | 21/21 (100) | 0 | <0.001* |
| Right ear | Left ear | 7/7 (100) | 0 | <0.001* |
| Right cheek | Left cheek | 36/36 (100) | 0 | <0.001* |
| Right shoulder | Left shoulder | 7/32 (21.8) | 25/32 (78.2) | <0.002* |
| Right axilla | Left axilla | 156/178 (87.6) | 22/178 (12.3) | <0.001* |
| Right arm | Left arm | 36/53 (67.9) | 17/53 (32.1) | <0.001* |
| Right elbow | Left elbow | 185/197 (94) | 12/197 (6) | <0.001* |
| Right cubital fossa | Left cubital fossa | 7/14 (50) | 7/14 (50) | 1 |
| Right forearm/wrist | Left forearm/wrist | 150/170 (88) | 20/170 (12) | <0.001* |
| Right dorsum of hand | Left dorsum of hand | 142/177 (80) | 35/177 (20) | <0.001* |
| Right fingers | Left fingers | 142/154 (92) | 12/154 (8) | <0.001* |
| Right periungual area | Left periungual areas | 89/98 (90.8) | 9/98 (9.2) | <0.001* |
| Right palm | Left palm | 28/28 (100) | 0 | <0.001* |
| Right nipple | Left nipple | 14/14 (100) | 0 | <0.001* |
| Right areola | Left areola | 14/25 (56) | 11/25 (44) | <0.001* |
| Right breast | Left breast | 71/71 (100) | 0 | <0.001* |
| Right half of the chest | Left half of the chest | 57/69 (82.6) | 12/69 (17.4) | <0.001* |
| Right half of the abdomen | Left half of the abdomen | 28/28 (100) | 0 | <0.001* |
| Right half of the back | Left half of the back | 50/50 (100) | 0 | <0.001* |
| Right buttock | Left buttock | 36/36 (100) | 0 | <0.001* |
| Right thigh | Left thigh | 71/82 (86.6) | 11/82 (13.4) | <0.001* |
| Right knee | Left knee | 157/180 (87) | 23/180 (13) | <0.001* |
| Right popliteal fossa | Left popliteal fossa | 43/57 (75.4%) | 14/57 (24.6) | <0.001* |
| Right leg | Left leg | 178/190 (94) | 12/190 (6) | <0.001* |
| Right malleolus | Left malleolus | 164/173 (95) | 9/173 (5) | <0.001* |
| Right dorsum of foot | Left dorsum of foot | 150/178 (84) | 28/178 (16) | <0.001* |
| Right toes | Left toes | 50/62 (80.6) | 12/63 (19.4) | <0.001* |
| Right periungual areas (toes) | Left periungual areas (toes) | 100/120 (83.3) | 20/120 (16.7) | <0.001* |
| Right side of scrotum | Left side of scrotum | 21/21 (100) | 0 | <0.001* |
| Right side of labia minora | Left side of labia minora | 14/14 (100) | 0 | <0.001* |
| Right side of vulva | Left side of vulva | 7/7 (100) | 0 | <0.001* |

- Clinical photo of (patient number 7) showing clinical similarity in vitiligo distribution comparing right and left sides of the body

- Clinical photo of (patient number 13) showing clinical similarity in vitiligo distribution comparing right and left sides of the body
- Clinical photo of (patient number 20) showing clinical similarity in vitiligo distribution comparing right and left sides of the body

- Clinical photo of (patient number 25) showing clinical similarity in vitiligo distribution comparing right and left sides of the body
Bilateral clinical involvement (n = 555/712) showed no statistically significant difference (P = 0.396). in males (n = 204/271, 75%) versus females (n = 351/441, 79%).
Upper versus lower part distribution across the transverse plane
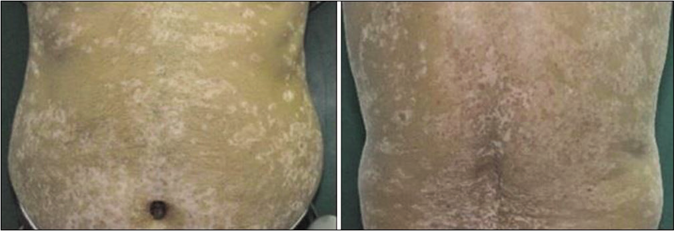
Involvement of both upper and lower parts of the body was present in 38% (n = 270) of patients [Table 3 and Figure 5].
| Studied association | Positive association, n (%) | Negative association, n (%) | P | |
|---|---|---|---|---|
| Right arm | Right thigh | 11/61 (18) | 50/61 (82) | 0.273 |
| Left arm | Left thigh | 11/53 (20.8) | 42/53 (79.2) | 0.138 |
| Right forearm | Right leg | 52/169 (30.8) | 117/169 (69.2) | 0.322 |
| Left forearm | Left leg | 32/151 (21.2) | 119/151 (78.8) | 0.462 |
| Right elbow | Right knee | 109/193 (56.5) | 84/193 (43.5) | <0.001* |
| Left elbow | Left knee | 109/204 (53.4) | 95/204 (46.6) | <0.001* |
| Right cubital fossa | Right popliteal fossa | 0 | 18/18 (100) | 0.453 |
| Left cubital fossa | Left popliteal fossa | 0 | 9/9 (100) | 0.552 |
| Right dorsum of hand | Right dorsum of foot | 64/180 (35.5) | 116/180 (64.5) | 0.103 |
| Left dorsum of hand | Left dorsum of foot | 71/157 (45.2) | 86/157 (54.8) | <0.001* |
| Right fingers | Right toes | 22/144 (15.3) | 122/144 (84.7) | 0.016* |
| Left fingers | Left toes | 22/156 (14.1) | 134/156 (85.9) | 0.003* |

- Clinical photo of (patient number 27) showing clinical similarity in vitiligo distribution in both upper and lower parts of the body
In addition, studying the clinical similarity in vitiligo distribution comparing upper and lower parts of body affection revealed a statistically significant positive association only between some areas e.g., upper and lower lips, upper and lower lip mucosa, nasal tip and chin, chin and neck [Table 4].
| Studied association | Positive association, n (%) | Negative association, n (%) | P | |
|---|---|---|---|---|
| Upper lip | Lower lip | 79/90 (87.8) | 11/90 (12.2) | <0.001* |
| Upper lip mucosa | Lower lip mucosa | 11/11 (100) | 0 | <0.001* |
| Right arm | Right forearm | 9/63 (14.3) | 54/63 (85.7) | 0.206 |
| Left arm | Left forearm | 9/54 (16.7) | 45/54 (83.3) | 0.575 |
| Right thigh | Right leg | 41/82 (50) | 41/82 (50) | 1 |
| Left thigh | Left leg | 30/83 (36.1) | 53/83 (63.9) | 0.091 |
Involvement of both upper and lower body parts (n = 270/712) was not significantly different (P = 0.241). in males (n = 109/271, 40%) versus females (n = 161/441, 37%).
Anteroposterior distribution across the frontal plane
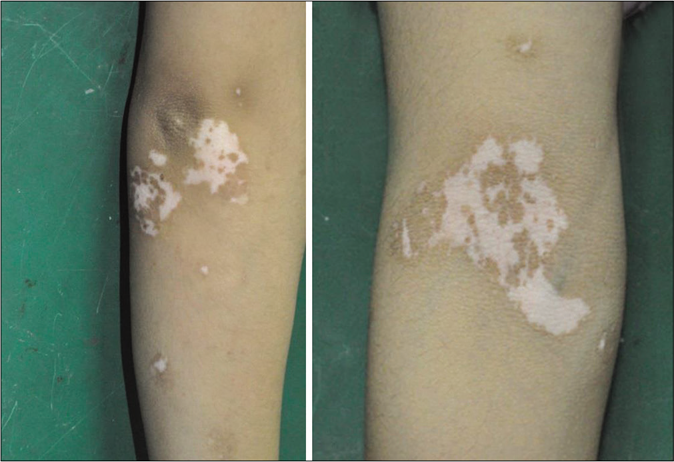
The anteroposterior distribution pattern among vitiligo patients revealed a significant positive association in 11% (n = 80/712). This was detected between the periauricular and postauricular areas (n = 40), and also between the abdomen and the back (n = 40) [Table 5 and Figures 6, 7].
| Studied association | Positive association, n (%) | Negative association, n (%) | P | |
|---|---|---|---|---|
| Right periauricular | Right postauricular | 20/31 (64.5) | 11/31 (35.5) | <0.001* |
| Left periauricular | Left postauricular | 20/31 (64.5) | 11/31 (35.5) | <0.001* |
| Right elbow | Right cubital fossa | 9/191 (4.7) | 182/191 (95.3) | 0.001 |
| Left elbow | Left cubital fossa | 0 | 205/205 (100) | <0.001* |
| Right dorsum of hand | Right palm | 20/186 (11.8) | 166/186 (88.2) | <0.001* |
| Left dorsum of hand | Left palm | 20/157 (12.7) | 137/157 (87.3) | <0.001* |
| Right side of chest | Right side of back | 22/64 (34.4) | 42/64 (65.6) | <0.001* |
| Left side of chest | Left side of back | 22/53 (41.5) | 31/53 (58.5) | <0.001* |
| Right side of abdomen | Right side of back | 20/20 (100) | 0 | <0.001* |
| Left side of abdomen | Left side of back | 20/20 (100) | 0 | <0.001* |
| Right knee | Right popliteal fossa | 11/172 (6.4) | 161/172 (93.6) | <0.001* |
| Left knee | Left popliteal fossa | 34/166 (20.5) | 132/166 (79.5) | <0.001* |
- Clinical photo of (patient number 35) showing clinical similarity in the antero-posterior distribution pattern among vitiligo patients
- Clinical photo of (patient number 40) showing clinical similarity in the antero-posterior distribution pattern among vitiligo patients
Anteroposterior clinical was not significantly different (P = 0.387) involvement (n = 80/712) in males (n = 35/271, 12.9%) versus females (n = 45/441, 10.2%).
A significant positive correlation was detected between longer disease duration and symmetry in all the 3 studied planes (P = 0.001, 0.035, 0.047, respectively). No other significant associations were detected with any clinical or demographic variable.
Discussion
Pattern recognition is at the heart of clinical dermatology,9 and several studies have been conducted in recent years to understand the patterns of lesion evolution in vitiligo.6,10,11 We believe that this study takes us a step closer to understanding the pattern of this unpredictable disease.
Symmetricity is traditionally thought of in terms of the right/ left relationship. However, literally it means the quality of being similar in parts facing each other or around an axis,. Accordingly, in our body, we can have horizontal, vertical and anteroposterior symmetry.12 In this study, 2876 lesions in 712 nonsegmental vitiligo patients were clinically studied for symmetry along those three planes, in an attempt to draw a clearer map for vitiligo.
Bilateral symmetry was the most significant, as it was documented in 78% (n = 555) of patients, followed by upper and lower symmetriy in 53% (n = 376), and anteroposterior symmetry in 11% (n = 80).
Focusing attention on the bilateral symmetry, all examined sites apart from the shoulders exhibited a significant positive bilateral symmetry. All sites exhibited at least 50% positive bilateral symmetry, that reached up to 100% in certain areas (nose, ear with the pre- and postauricular areas, eyelids, cheeks, palms, breasts with nipple, abdomen, back, buttocks, genitalia (scrotum, labia and vulva).
Furthermore, we noticed that areas of predilection previously described, are also the most prone to exhibit bilateral symmetry.4 For example, among the 15 sites that exhibited 100% bilateral symmetry, ten belonged to the previously categorized areas of predilection.4 Furthermore, areas prone to koebnerization demonstrated high rates of bilateral symmetry, such as the malleolus which is highly prone to trauma owing to the praying and sitting habits in our country (95%), as well as the palms (100%). The high rates of bilateral symmetry exceeding 50%, support the previous notion of “often” symmetrical, but our study revealed some areas to be more prone than others.4
Analyzing the vertical symmetricity pattern (upper/lower) around the transverse plane, most sites did not show such a pattern. We did not observe lesions occurring on lips or neck and genitalia in any patient. The vertical symmetry rate ranged from 15% (fingers and toes) around 55% (elbows and knees). Even here, positive vertical symmetry was mainly noted in the areas previously described to be sites of predilection (elbows, knees, digits, dorsum of hands/feet).
We also studied vertical symmetry among different anatomical areas. We found some interesting data; 90-100% symmetry was detected between the upper and lower lip and its mucosa respectively, drawing attention to the importance of protecting the lips once a lesion starts to appear on one.
Lower rates of symmetry were noted in the extremities, with around 15% positive association between arm and forearm, and 36-50% between thigh and leg. Nevertheless, the existence of such associations highlights the importance of taking into account both horizontal and vertical symmetries once lesions emerge on the extremities.
The anteroposterior aspect added further to the vitiligo map. 100% of the cases showed a positive association between the back and abdomen and around 40% between back and chest. Moreover, a positive association between pre- and postauricular areas was detected in around 65% of the cases. The rest of the sites showed strongly negative association (80%-100%). We cannot fully explain this finding. However, several hypotheses can be suggested including different developmental patterns and unlikely exposure to kobnerization in the anteroposterior direction of the body.
It is essential to highlight that negative associations should be considered as important as the positive ones, with both together helping us in drawing the individual map of each case of vitiligo, helping in identifying the areas likely to get affected.
The significant association between the positive symmetry in all studied areas and the duration of the disease is a point of crucial importance. It clarifies the image that vitiligo in each patient follows a preset map, rather than being haphazard. It just takes time to fulfill the picture. It could help us to draw a map for the patient in the first visit itself, so that we can build our therapeutic plan paying attention to areas at higher risk.
Another point of importance is the significance of this symmetry in vitiligo. Still little is known about the biological basis of why any disease has a pattern, despite efforts to categorize pattern inducers.9 In recent work, cutaneous mosaicism was suggested to be involved in the pattern of segmental vitiligo.13,14 In general, a pattern formation is claimed to represent the crossroad between three basic elements; genetics, developmental biology and clinical dermatology, a rule that can be applied to nonsegmental vitiligo.9
Conclusion
The current work studied the symmetricity along the three different (sagittal, transverse and frontal) planes in generalized nonsegmental vitiligo and found significant bilateral symmetry (78%) was found to be positively correlated with the disease duration. Furthermore, the study sheds light on the positive and negative associations between different body parts which might aid in drawing the anticipated map of vitiligo that in turn could aid treatment and prophylaxis. Still, further work is needed to establish the reliability of this work, and whether it is the same among different ethnic groups. In addition, proper therapeutic plans, based on the prevention concept, need to be established and evaluated regarding long-term outcomes. A relatively small number of participants is a limitation of this study.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Vitiligo: Symptoms, pathogenesis and treatment. Int J Immunopathol Pharmacol. 2014;27:485-9.
- [CrossRef] [PubMed] [Google Scholar]
- Vitiligo: A comprehensive overview Part I. Introduction, epidemiology, quality of life, diagnosis, differential diagnosis, associations, histopathology, etiology, and work-up. J Am Acad Dermatol. 2011;65:473-91.
- [CrossRef] [PubMed] [Google Scholar]
- Distribution patterns in generalized vitiligo. J Eur Acad Dermatol Venereol. 2014;28:755-62.
- [CrossRef] [PubMed] [Google Scholar]
- The definition and assessment of vitiligo: A consensus report of the Vitiligo European Task Force. Pigment Cell Res. 2007;20:27-35.
- [CrossRef] [PubMed] [Google Scholar]
- Association of the Köbner phenomenon with disease activity and therapeutic responsiveness in vitiligo vulgaris. Arch Dermatol. 1999;135:407-13.
- [CrossRef] [Google Scholar]
- What is the biological basis of pattern formation of skin lesions? Exp Dermatol. 2006;15:547-64.
- [CrossRef] [PubMed] [Google Scholar]
- Depigmentation patterns of nonsegmental vitiligo: A prospective study of macromorphologic changes in lesions. Am J Clin Dermatol. 2013;14:55-9.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical patterns of vitiligo and its associated co morbidities: A prospective controlled cross-sectional study in South India. Indian Dermatol Online J. 2012;3:114-8.
- [CrossRef] [PubMed] [Google Scholar]
- Simple Definition of Symmetry. Available from: http://www.merriam-webster.com/dictionary/symmetry [Last accessed on 2016 May 28]
- [Google Scholar]
- The distribution pattern of segmental vitiligo: Clues for somatic mosaicism. Br J Dermatol. 2013;168:56-64.
- [CrossRef] [PubMed] [Google Scholar]
- Genetic Susceptibility to Vitiligo: GWAS Approaches for Identifying Vitiligo Susceptibility Genes and Loci. Front Genet. 2016;7:3.
- [CrossRef] [PubMed] [Google Scholar]




