Translate this page into:
A case of cutaneous focal bilirubin deposition in a man with jaundice
Correspondence Address:
Ji Ping Xia
Department of Dermatology, The First Affiliated Hospital of Nanjing Medical University, 300 Guang Zhou Road, Nanjing 210029
China
| How to cite this article: Bin Jameel AA, Zhou BR, Xia JP. A case of cutaneous focal bilirubin deposition in a man with jaundice. Indian J Dermatol Venereol Leprol 2018;84:320-322 |
Sir,
Spontaneous appearance of a green pigmented cutaneous rash is an unusual clinical finding and it may present in certain medical scenarios such as chloroma, second stage of well's syndrome, copper deposition in the hair and nails and pseudomonas infection.[1] However, such kind of unusual green pigmentation on the palms and soles also happens to be associated with underlying hyperbilirubinemia. In the literature, till now very few cases have been reported.[1],[2],[3],[4],[5],[6],[7],[8]
A 65-year-old male presented with a 10 days history of an asymptomatic progressive skin rash on his bilateral palms and soles. Patient complained of progressive jaundice and flatulence for about 2 months and was recently diagnosed with cholangiocarcinoma. There was no fever, sweating or any other symptoms. Physical examination revealed multiple, discrete, green to black, 1–2 mm pin point macules mainly on the palms and soles, especially on the volar and lateral aspects of the fingers and dorsomedial aspects of the toes [Figure - 1] and [Figure - 2]. The green punctae were distributed along the dermatoglyphic ridges. Patient denied any recent use of topical or oral medications. He also denied any contact with greenish dyes or substances. Histopathological examination of the lesional skin biopsy indicated hyperkeratosis, parakeratosis and deposition of a pink amorphous substance within the stratum corneum [Figure - 3] and [Figure - 4]. The gram stain, potassium hydroxide examination and hall stain (if positive indicates a yellow hue) were negative. Tissue cultures for bacteria and fungus were also negative. Liver function test indicated elevated levels of total serum bilirubin (20.1 mg/dl). Patient underwent an elective pylorus sparing pancreaticoduodenectomy. Two months after the surgery, the total serum bilirubin levels decreased to 0.9 mg/dl and were within the normal range (0.3–1.1 mg/dl). No further recurrence of the skin lesions was observed since then. According to the clinical and laboratory findings, a diagnosis of cutaneous focal bilirubin deposition was made.
 |
| Figure 1: Multiple, discrete, green to black, pin point macular rash on the palms |
 |
| Figure 2: Multiple, green to black pin point macules on the soles |
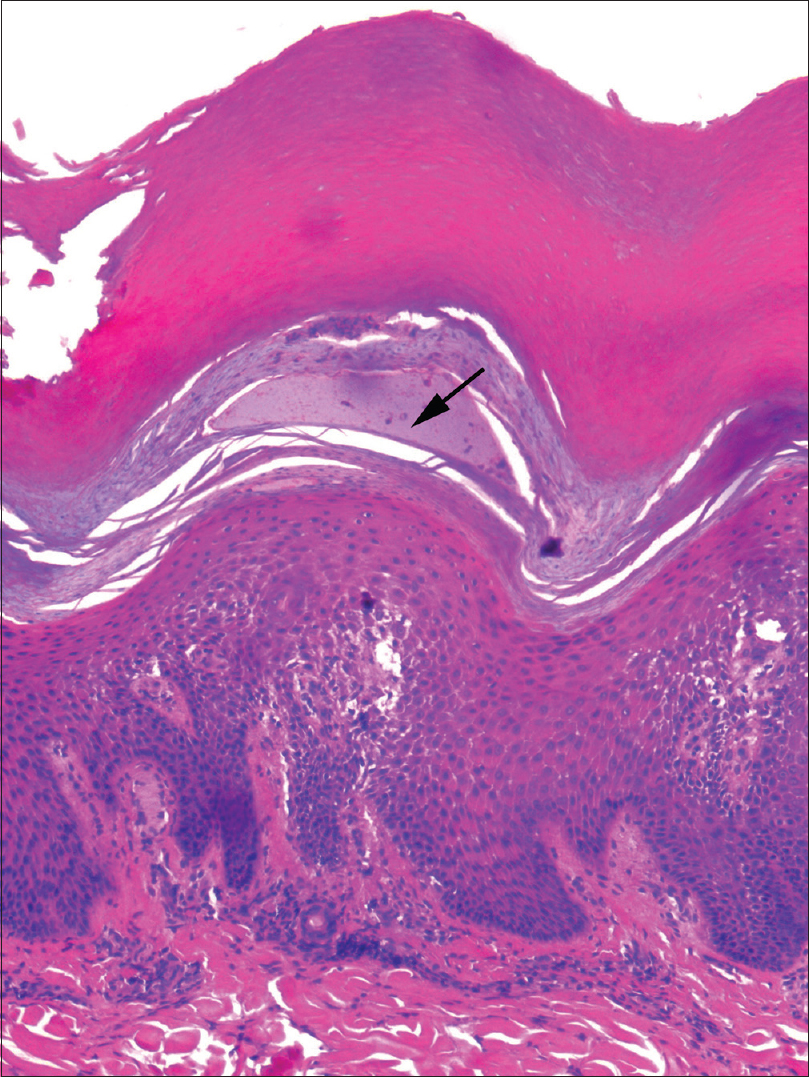 |
| Figure 3: Hyperkeratosis and amorphous pink material in the stratum corneum consistent with bilirubin (arrow) (H and E, ×100) |
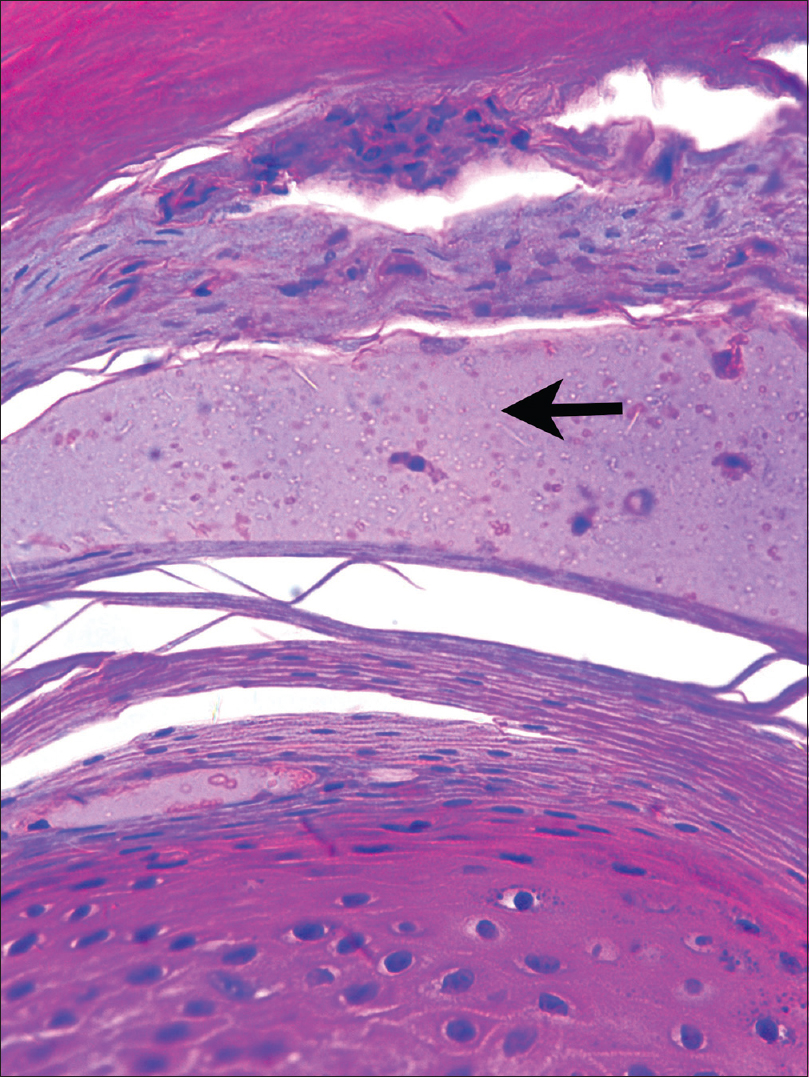 |
| Figure 4: The presence of amorphous pink material in the stratum corneum consistent with bilirubin (arrow) (H and E, ×400) |
Spontaneous appearance of a greenish pigmented rash on the palms and soles in patients with hyperbilirubinemia is a rare entity. Kanzaki and Tsuda were the first to report it in two patients, one with non-A, non-B acute hepatitis and the other recovering from a bypass surgery.[2] Over the years, similar rash has been reported in patients suffering from cholecystitis, choledocholithiasis, cholangiocarcinoma, adenocarcinoma of the gall bladder, biliary atresia, alcoholic liver cirrhosis and invasive duodenal adenocarcinoma.[1],[3],[4],[5],[6],[7],[8] Usually, it is a greenish yellow pigmented rash with black-brown pin-point macules or papules or vesicles usually distributed along the dermatoglyphic ridges where eccrine sweat glands open. Moreover, in all of the reported cases, the rash was located only on the palms and soles, the location where eccrine glands are abundant.[1],[2],[3],[4],[5],[6],[7],[8] Our patient also had strikingly similar features on his palms and soles along with marked hyperbilirubinemia secondary to cholangiocarcinoma. The transient association of a green pigmentation with underlying marked hyperbilirubinemia and its resolution on correction of the serum abnormality supports the deposition of bilirubin and/or metabolites into the skin as the probable mechanism for the clinical presentation.[3] In 1992, Kanzaki and Tsuda regarded this eruption as a variant of eccrine chromhidrosis (a condition characterized by excretion of water soluble pigment from certain dyes or drugs through the eccrine sweat glands). They hypothesized that direct water soluble bilirubin is excreted into the stratum corneum through the eccrine glands eventually where it gets oxidized to biliverdin.[2],[3] Fever and perspiration can also be considered as contributing factors but may not be present in all cases.[1] However, the special staining for bilirubin and/or metabolites did not yield any significant outcome. As reported in the literature, only two cases have shown positive results for bile stain.[1],[4] This may be due to the unavailability of optimal techniques to detect the presence of cutaneous bilirubin metabolites. Apart from the cutaneous deposition, bilirubin metabolites also tend to get deposited in the hard dental tissues secondary to hyperbilirubinemia during dentition. This contributes to the characteristic greenish discoloration of the permanent and deciduous teeth in individuals with congenital biliary atresia.[9]
Cutaneous focal bilirubin deposition is a very rare entity since not all patients with hyperbilirubinemia present with such a phenomenon. Diagnosis is usually based on the classic clinical and histopathological findings. However, certain medical scenarios such as chromhidrosis and pseudochromhidrosis need to be ruled out. We would like to report a case of cutaneous focal bilirubin deposition and would also like to highlight the fact that this condition can be considered as the cutaneous sign of underlying hepatobiliary disease.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Allegue F, Hermo JA, Fachal C, Alfonsín N. Localized green pigmentation in a patient with hyperbilirubinemia. J Am Acad Dermatol 1996;35:108-9.
[Google Scholar]
|
| 2. |
Kanzaki T, Tsuda J. Bile pigment deposition at sweat pores of patients with liver disease. J Am Acad Dermatol 1992;26:655-6.
[Google Scholar]
|
| 3. |
Fung MA, LeBoit PE, Maibach HI. Coalescing green and yellow papules on the feet. Arch Dermatol 2000;136:113, 116.
[Google Scholar]
|
| 4. |
Di Stefani A, Bianchi L, Orlandi A, Chimenti S. Green sweating spots on hands and feet: Unusual expression of hyperbilirubinemia. Ann Intern Med 2006;145:710-1.
[Google Scholar]
|
| 5. |
Triwongwaranat D, Kasemsarn P, Boonchai W. Green pigmentation on the palms and soles. Acral green pigmentation (eccrine chromhidrosis). JAMA Dermatol 2013;149:1339-40.
[Google Scholar]
|
| 6. |
So JK, Romero L. Eccrine chromhidrosis secondary to hyperbilirubinemia. Dermatol Online J 2014;21. pii: 13030/qt6hz8s1mh.
[Google Scholar]
|
| 7. |
Aaron RS, Zacharias I, Mannion S, Gordon FD. Rare cutaneous manifestation of hyperbilirubinemia. Arch Dermatol 2010;146:209-10.
[Google Scholar]
|
| 8. |
Keum DI, Hong H, Lee SH, Ahn SK. Eccrine chromhidrosis resembling clinical features of pompholyx with bile-like greenish pigmentation on the right palm and soles. Ann Dermatol 2015;27:482-3.
[Google Scholar]
|
| 9. |
Rakauskaite A, Juodzbalys G, Pauza DH, Cicciù M. Green pigmentation in human teeth. A stereomicroscopic study. J Clin Pediatr Dent 2014;38:355-61.
[Google Scholar]
|
Fulltext Views
4,259
PDF downloads
4,199





![[Figure - 1]](#fig_ijdvl_2018_84_3_320_228672_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_3_320_228672_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2018_84_3_320_228672_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2018_84_3_320_228672_f4.jpg){kind=link}