Translate this page into:
A case of giant sebaceous carcinoma localized in the breast area of a male patient
2 Dermatological Surgery Unit, Department of Dermatology, Morgagni-Pierantoni Hospital, Forl�;Institute of Dermatology, University of Trieste, Trieste, Italy
3 Pathology Unit, Morgagni-Pierantoni Hospital, Forl�, Italy
4 Department of Medical Oncology, Isituto Scientifico Romagnolo per lo Studio e la Cura dei Tumori (I.R.S.T.), Meldola, Italy
5 Dermatological Surgery Unit, Department of Dermatology, Morgagni-Pierantoni Hospital, Forl�, Italy
6 Institute of Dermatology, University of Trieste, Trieste, Italy
Correspondence Address:
Antonio Ascari-Raccagni
Dermatological Surgery Unit, Department of Dermatology, Morgagni-Pierantoni Hospital, via Forlanini 34, 47121 Forli
Italy
| How to cite this article: Ascari-Raccagni A, Dondas A, Padovani F, Milandri C, Righini MG, Trevisan G. A case of giant sebaceous carcinoma localized in the breast area of a male patient. Indian J Dermatol Venereol Leprol 2011;77:403 |
Sir,
Cutaneous sebaceous carcinoma (SC) is a rare, aggressive tumor that originates in the holocrine adnexal epithelium of sebaceous glands. Around 400 cases have been reported to date in the literature, of which 120 were extra-orbital in origin and the remaining periorbital. [1] Extra-ocular SC occurs predominantly in the head and neck area, where the concentration of sebaceous glands is highest. Other uncommon locations include the external genitalia, trunk and limbs. We report a case of a giant sebaceous carcinoma localized in the breast area of a male patient.
A 61-year-old man was seen in our department for a large, painless, ulcerated lesion localized in the left breast area, measuring 12 x 9 cm [Figure - 1]. The lesion had first appeared four years earlier and had slowly grown, gradually including and then totally destroying the homo-lateral nipple. The ulcerated neoformation was well-circumscribed and slightly elevated, with bright red edges. The bottom central part of the lesion was depressed, yellowish and foul-smelling. The patient had never consulted his general physician about it and had never used any kind of topical or systemic therapy in an attempt to resolve the problem.
 |
| Figure 1: Ulcerated lesion with bright red edges localized in the area of the left breast (12 × 9 cm) |
Initial diagnostic hypotheses were made of an invasive cutaneous basal cell carcinoma gradually extending into the breast or a male breast carcinoma involving superficial tissue layers. A large diamond-shaped biopsy was performed, including both edges and central part of the lesion. Histological evaluation was performed with hematoxylin and eosin staining, revealing neoplastic dermal lobular proliferation of epithelial cells with sebocytic differentiation. The tumor cells showed a large, eosinophilic, clear, vacuolated cytoplasm and voluminous nucleus; numerous atypical mitoses were also present [Figure - 2].Neoplastic cell immunoreactivity was observed for epithelial membrane antigen (EMA), with a distinctive pattern of cytoplasmic "bubbliness" [Figure - 3].
Histological examination confirmed a diagnosis of ulcerated, infiltrating sebaceous carcinoma (SC), a rare cutaneous malignancy arising from the holocrine adnexal epithelium of sebaceous glands.
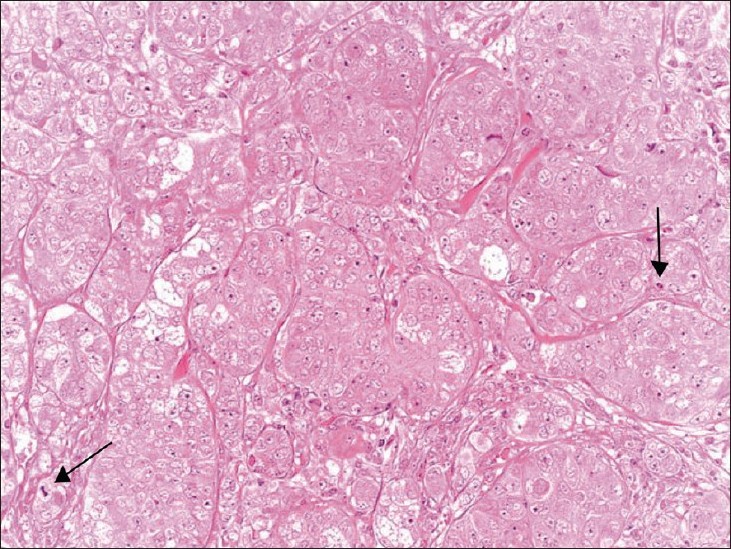 |
| Figure 2: Tumor cells with sebaceous differentiation showing brisk mitotic activity (arrow) (H and E, ×40) |
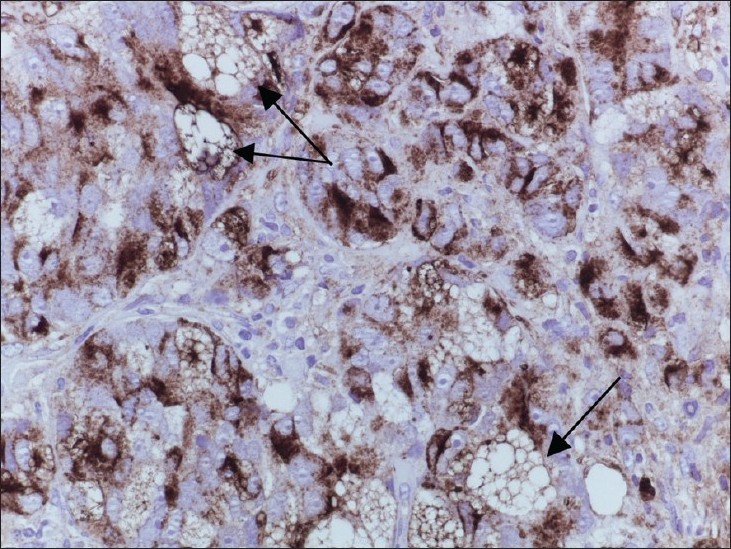 |
| Figure 3: Tumor cells showing a distinctive pattern of cytoplasmic "bubbliness" (arrow) (EMA, ×40) |
The patient reported intense pain in the spinal area, urination and defecation discomfort and modest spastic paraparesis. Contrast-enhanced computed tomography (CT) of the brain, chest and abdomen and magnetic resonance imaging (MRI) of the spine were carried out, highlighting secondary osteolytic processes involving the cervical, chest and lumbar vertebra and the sacrum and rib cage area, with collapse of D10 and D11, in addition to several large left axillary adenopathies. The tumor had spread to the vertebral column at the chest and lumbar level. Gastroenterologic and urologic investigations were performed and were negative, thus excluding the possibility of an association with the Muir-Torre syndrome.
Due to the size of the primary lesion and the extension of the secondary lesions, surgery was not considered as an option. As there were signs of the onset of spinal cord compression, the patient underwent high-dose dexamethasone treatment and radiotherapy on the dorsal spine. Osteotropic therapy with zoledronic acid, systemic chemotherapy with carboplatin and 5-fluorouracil, and opioid analgesic therapy were also initiated. [2] A stiff corset/bust, foam rubber collar and wheelchair were prescribed.
The cutaneous lesion is currently in slow regression and the patient is undergoing regular follow-up.
Sebaceous carcinoma is a rare tumor without a distinctive appearance, it is often mistaken for sebaceous adenoma, basal cell carcinoma with sebaceous differentiation, squamous cell carcinoma, clear cell hidradenocarcinoma, metastatic renal cell carcinoma and metastatic prostate cancer.
SC is classified into two main groups: periocular SC, which arises from the ocular sebaceous glands and an extra-ocular form, threefold less common than the former type.
SC can occur spontaneously or in combination with the Muir-Torre syndrome, a rare autosomal dominant genodermatosis characterized by sebaceous gland tumors and/or keratoacanthoma associated with visceral malignancies, including gastrointestinal and genitourinary cancers. [3],[4]
| 1. |
Dowd MB, Kumar RJ, Sharma R, Murali R. Diagnosis and management of sebaceous carcinoma: an Australian experience. ANZ J Surg 2008;78:158-63.
[Google Scholar]
|
| 2. |
Wu CY. Muir-Torre syndrome: Extraocular sebaceous carcinoma with adenocarcinoma of colon in a 76-year-old man. Clin Exp Dermatol 2009;34:e399-400.
[Google Scholar]
|
| 3. |
Abbas O, Mahalingam M. Cutaneous sebaceous neoplasms as markers of Muir-Torre syndrome: A diagnostic algorithm. J Cutan Pathol 2009;36:613-9.
[Google Scholar]
|
| 4. |
Murthy R, Honavar SG, Burman S, Vemuganti GK, Naik MN, Reddy VA. Neoadjuvant chemotherapy in the management of sebaceous gland carcinoma of the eyelid with regional lymph node metastasis. Ophthal Plast Reconstr Surg 2005;21:307-9.
[Google Scholar]
|
Fulltext Views
2,194
PDF downloads
2,785





![[Figure - 1]](#fig_ijdvl_2011_77_3_403_79745_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_3_403_79745_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2011_77_3_403_79745_f3.jpg){kind=link}