Translate this page into:
A comparison of irradiance at different body sites in whole-body narrowband-ultraviolet B cabins
Correspondence Address:
Furen Zhang
Department of Dermatology, Shandong Provincial Institute of Dermatology and Venereology, 27397 Jingshi Road, Jinan, Shandong Province, 250 022
China
| How to cite this article: Shan X, Wang C, Yang B, Zhang F. A comparison of irradiance at different body sites in whole-body narrowband-ultraviolet B cabins. Indian J Dermatol Venereol Leprol 2012;78:745-746 |
Sir,
Ultraviolet B (UVB) phototherapy is widely used to treat psoriasis, but treatment in whole-body narrowband UVB (NB-UVB) cabins may cause phototoxic reactions, which commonly occur in the trunk, less frequently in the limbs and seldom in the lower limbs. The main reason for this may be the different sensitivity of skin to NB-UVB in different parts of the body. Another reason may be the difference in irradiance at different parts of the body in whole-body NB-UVB cabins.
In this study, we aimed to investigate the irradiance at different parts of the body in a whole-body NB-UVB cabin. Twenty adult volunteers excluding pregnant and lactating women were enrolled in this study, which was conducted from March 2011 to April 2011. Approval was obtained from the Institutional Review Board of Shandong Provincial Hospital of Dermatology, and written informed consent was obtained from each healthy volunteer. The height, body weight, and waist circumference of each volunteer was recorded.
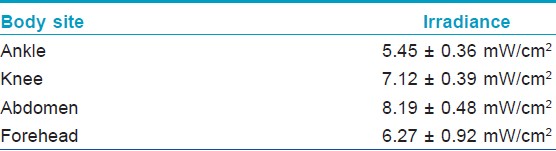
The whole-body NB-UVB cabins (Sigma Co., Shanghai, China) in this study were equipped with 40 Philips TL 100W/01 UVB lamps, lining each wall of the quadrilateral cabin. Lamps were warmed up for 180 seconds, and the irradiance was confirmed to be stable before measurements were taken. Volunteers with standard UV shielding were asked to stand in the center of the cabin. A hand-held radiometer (International Light Radiometer, Model IL1400A, Detector Head Model sel005, Newburyport, MA, USA) was used to measure irradiance at 4 sites of the body: The ankle, knee, abdomen, and forehead. For each site, volunteers obtained 3 sequential measurements of irradiance, of which the mean value was determined.
Data were analyzed with SPSS 11.0 for Windows. The mean values of irradiance detected on different parts of the body were compared using Friedman′s test for k-related samples. The Wilcoxon signed rank test was used to test for significant differences between irradiance at pairs of body sites. P values of less than 0.05 were considered statistically significant.
The mean ± SD height of 20 volunteers was 169 ± 8.42 cm (range 155-185 cm); body weight was 72.15 ± 18.18 kg (range 44-110 kg); waist circumference was 92.6 ± 15.48 cm (range 78-132 cm). [Table - 1] summarizes the irradiance measured at the different body sites. The irradiance on the abdomen was higher than on the ankle, knee, and forehead (P<0.001 respectively) using the Wilcoxon signed rank test.
Waist circumference and body weight correlated with irradiance on the abdomen using the non-parametric Spearman′s rank test (rs = 0.62, P < 0.01) and Pearson′s correlation coefficient (r = 0.67, P < 0.01), respectively, which means a larger waist circumference and a heavier body weight lead to a higher irradiance on the abdomen. There was no detectable correlation between height and irradiance on the abdomen using Pearson′s correlation coefficient.
When adult volunteers are treated in the whole-body NB-UVB cabin, the height of their trunk is at the center of the lamp, while the face and lower legs are located at opposite ends. This results in the lower legs and face receiving less radiation because the radiation is only coming from one side compared the radiation received by the mid area. [1] Furthermore, the distance between the skin and the UV lamps varies for different body parts and for different individuals as the trunk is closer to the lamps than are the lower limbs, especially for adults with central obesity or a large waist circumference. This leads to more irradiation at the trunk according to the inverse- square law for light.
The sensitivity of skin to ultraviolet light on different parts of the body varies, and generally, the trunk is more sensitive than the extremities, [2],[3] so, there appear to be two exacerbating factors in whole-body NB-UVB phototherapy: The trunk is sensitive to ultraviolet light but receives more radiation, yet the lower legs are insensitive but receive less radiation, and accordingly phototoxic reactions occur more commonly in the trunk, and seldom in the lower legs. As for the face, most Chinese patients refuse to receive phototherapy because of hyperpigmentation.
The response of psoriasis lesions to NB-UVB phototherapy is related to the radiation dose, and a high-dose UVB therapy results in fewer treatments with better long-term efficacy. [4],[5] For almost all psoriasis patients who receive treatment in whole body NB-UVB cabins, the trunk lesions resolve faster than those on the extremities, especially those on the lower legs. May be the disproportionate UV intensity is one of the reasons for this. Since the skin on the limbs can tolerate more UV irradiation, it might be useful to give a supplementary radiation dose to the limbs, especially the lower legs after whole-body NB-UVB treatment to facilitate the clearance of psoriasis lesions.
| 1. |
Clarkson DMcG, Franks L. The use of a simulated body shape for determination of patient dosimetry within whole body ultraviolet treatment cabinets. Phys Med Biol 2006;51:51-8.
[Google Scholar]
|
| 2. |
Rhodes LE, Friedmann PS. A comparison of the ultraviolet B-induced erythemal response of back and buttock skin. Photodermatol Photoimmunol Photomed 1992;9:48-51.
[Google Scholar]
|
| 3. |
Leslie KS, Lodge E, Garioch JJ. A comparison of narrowband (TL-01) UVB-induced erythemal response at different body sites. Clin Exp Dermatol 2005;30:337-9.
[Google Scholar]
|
| 4. |
Kleinpenning MM, Smits T, Boezeman J, van de Kerkhof PC, Evers AW, Gerritsen MJ. Narrowband ultraviolet B therapy in psoriasis: randomized double-blind comparison of high-dose and low-dose irradiation regimens. Br J Dermatol 2009;161:1351-6.
[Google Scholar]
|
| 5. |
Dogra S, De D. Narrowband ultraviolet B in the treatment of psoriasis: The journey so far!. Indian J Dermatol Venereol Leprol 2010;76:652-61.
[Google Scholar]
|
Fulltext Views
1,663
PDF downloads
1,632





![[Table - 1]](#tbl_ijdvl_2012_78_6_745_102373_t1.jpg){kind=link}