Translate this page into:
A novel scoring system for evaluation of results of autologous transplantation methods in vitiligo
Correspondence Address:
Bhushan Kumar
Department of Dermatology, Venereology and Leprology, Postgraduate Institute of Medical Education & Research, Chandigarh-160 012
India
| How to cite this article: Gupta S, Honda S, Kumar B. A novel scoring system for evaluation of results of autologous transplantation methods in vitiligo. Indian J Dermatol Venereol Leprol 2002;68:33-37 |
Abstract
Autologous transplantation of melanocyte/melanocytes bearing epidermis for vitiligo can be done by mini-punch grafting (MPG), suction blister epidermal grafting (SBEG), thin split -thickness skin grafting (TSTG), transplantation of basal cell layer enriched suspension and cultured epithelial/melanocyte transplantation. To date no comparative study of these transplantation procedures has been published. Comparison of different studies carried out at different centers may be difficult in the absence of uniform evaluation criteria. In most of the published studies, the results were evaluated in terms of extent of pigmentation. Complictions and color match were evaluated separately. This approach, however, may not give a fair idea about the results.We have developed a scoring system with holistic approach considering the extent of pigmentation, color match and the complications of both the donor and the recipient areas, all taken together. In the scoring system, the score for individual criteria was multiplied with a factor, the value of which was decided on the basis of relative importance of each criteria. The use of this scoring system is exemplified in twelve patients who underwent TSTG, SBEG and MPG. In the scoring system the results were judged as excellent and fair in 3 patients each, as good in 4 patients and as poor in 2 patients.
Introduction
Autologous transplantation of melanocytes/melanocyte bearing epidermis for vitiligo can be done by a wide variety of methods.[1] These include mini punch grafting (MPG),[2] suction blister epidermal grafting (SBEG),[3],[4] thin split thickness grafting (TSTG),[5] transplantation of basal cell layer enriched suspension,[6] and cultured epithelial / melanocytes transplantation.[7],[8] To date no single study has been published, which has compared the results of these methods. In the era of evidence based medicine,[9] a question may arise for an operating surgeon, which method gives him/her the best results? However, it may be difficult to compare the results of different studies on different methods in the absence of uniform and acceptable evaluation criteria. In most of the studies published to date, the success in a given patient was rated by the extent of pigmentation (EOP).The complication of donor area (CDA) and the recipient area (CRA) were evaluated separately. The color match (CM) with the surrounding skin was vaguely mentioned or not mentioned at all. There are certain drawbacks in this. For example, in a patient with a patch of vitiligo developing> 90% pigmentation after transplantation (done with the sole purpose of improving color), but also developing at the same time a keloid, hypertrophic or unsightly scar or hyperpigmentation at recipient or donor site may be projected as highly satisfactory during evaluation in terms of the effectiveness of the procedure, though the outcome may be more embarrassing to the patient than the original problem. Thus, there is a need for developing a scientific evaluation system with holistic approach, which includes the extent of pigmentation, color match and complications simultaneously. We have been following such a scoring system for our patients who have undergone various transplantation procedures for vitiligo/other leukodermas.
Materials and Methods
The scoring system and its application
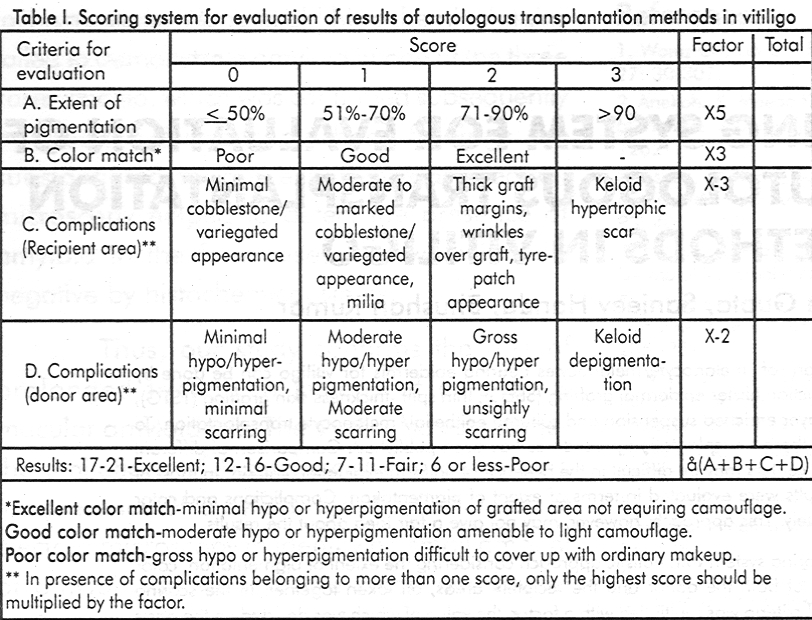
The scoring system is given in [Table - 1]. The evaluation according to this evaluation system is advocated to be done at least one year after the transplantation procedure, which is a sufficient time for the emergence of the final picture of all the surgical procedures.
In the proposed scoring system, a relatively higher rating is given to the pigmentation, as this is the major concern for the patient and the treating physician. In a given patient, if a patch of depigmentation is treated, extent of pigmentation is of prime importance and after this is redeemed, it is the quality of the color match, which becomes important. In some studies, poor color match at the recipient site has been considered as a complication.[10]
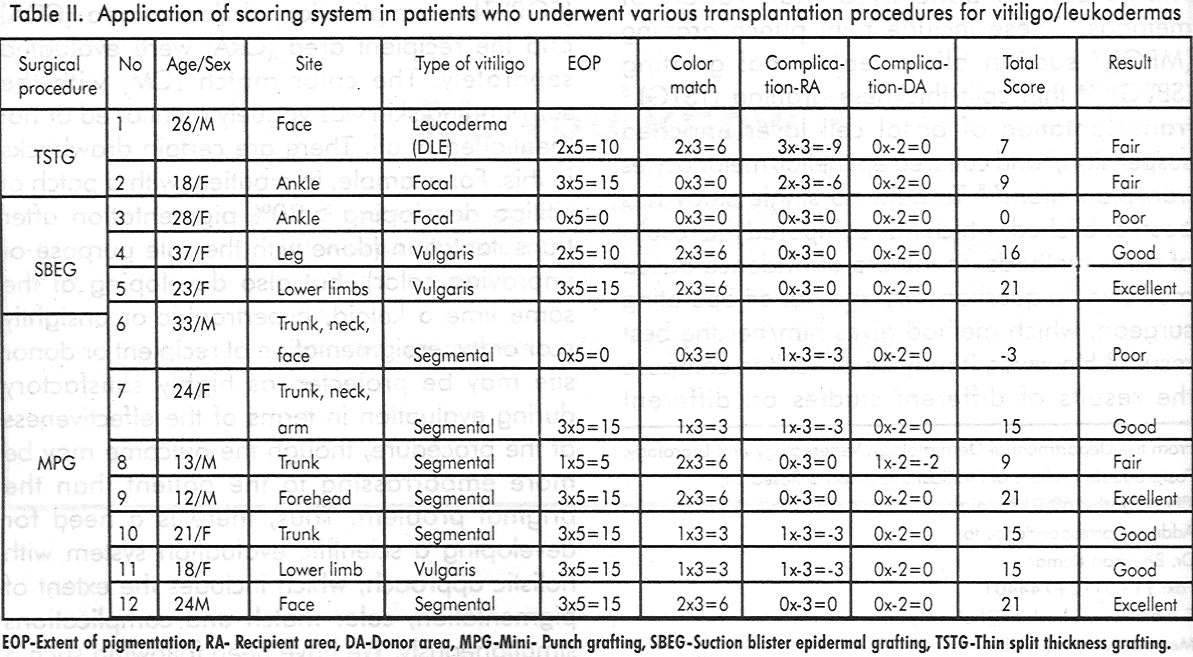
However, we feel that it is a poor outcome of the procedure rather than a complication. Hence, in our scoring system it is evaluated separately. Severe complications, which may nullify the results, merit a high negative score. On the other hand, superficial scarring and/or minimal hypo or hyperpigmentation of donor site are inevitable in grafting procedures and have been considered as negligible complications and thus merit a zero score in the proposed scoring system. An unsightly scar or keloid over the recipient area is considered as a severe complication, while over the donor area it is considered as a moderate complication because generally it is at a hidden/unexposed site. The multiplication factors were decided on the basis of relative importance of each variable. The use of this scoring system is exemplified in the description of the following cases that underwent various transplantation procedures [Table - 2]. The scoring was done on the patients by two independent observers who are regularly involved in the surgical correction of depigmentation disorders. The blinding was not possible, as the outcome of the procedure was obvious to reveal the nature of the procedure done. The final results of the evaluation by both the investigators were identical in all the patients with the exception of patient no.6. They finally came to consensus after discussions.
Procedure: Thin split thickness grafting
Case 1. A 26-year-old male with healed depigmented areas of discoid lupus erythematosus (DLE) was treated with TSTG. Initially he achieved 100% pigmentation. Five months later the disease got reactivated and pigmented area reduced to about 75% from 100% (EOP score 10). The junction of the graft with the surrounding skin was obvious as the graft did not match the surrounding skin texture or thickness resulting in a ′tyre-patch′ appearance (CRA score-6). The color match was excellent (CM score 6). Thus the resultant final score was 10 (10+6-6). The final outcome was considered as fair in our proposed scoring system.
Case 2. An 18-year-old female with focal vitiligo patch on the ankle was treated with TSTG. Though the graft had taken up well and the patch pigmented completely (EOP score 15), the margins of the graft failed to match the surrounding skin color, texture and thickness, giving it a tyre-patch appearance (CM score 0x3=0, CRA score 2x-3=-6, total score 9). The result was judged as fair, though the pigmentation achieved was 100%.
Procedure: Suction blister epidermal grafting
Case 3. A 28-year-old woman with a focal vitiligo patch on the ankle treated with SBEG, developed about 30% pigmentation (EOP score 0) with poor color match (CM score 0) and no complications (score 0). The final outcome was poor (total score=0).
Case 4. A 37-year-old female with residual patches of stable vitiligo vulgaris on leg was treated with SBGE. She developed around 75% pigmentation 12 months after surgery (EOP score 10). The color match was excellent (CM score 6). There were no complications. The total score was 16 and the result was considered as good in our scoring system.
Case 5. A 23-year- old female with residual patches of vitiligo vulgaris on lower limb was treated with SBEG. One year later, about 95% areas were pigmented (EOP score 15). The color match was excellent (CM score 6). There was mild variegated appearance over the patches (CRA score 0). The total score was 21 -an excellent score.
Procedure: Mini-punch grafting
Case 6. A 33-year- old male patient with a large segmental vitiligo involving trunk, neck and face was treated with minigrafting. One year later he developed around 40% pigmentation in the grafted area (EOP score 0). He, however, had gross hyperpigmentation resulting in a poor color match (CM score 0). There was moderate variegated appearance (CRA score-3). Thus he got a total score-3-a poor outcome.
Case 7. A 24-year-old female with a segmental vitiligo on the upper chest, shoulder, neck and upper arm was treated with minigrafting. After one year of follow-up she achieved more than 90% pigmentation with good color match (EOP score 15, CM score 3). However, she had moderate variegated and cobblestone appearance (CRA score-3). The resulting total score was 15-a good result.
Case 8. A 13-year-old boy with segmental vitiligo on the chest was treated with MPG. One year later he developed around 55% pigmentation (EOP score 5) with excellent color match (CM score 6). He had minimal cobblestone appearance (CRA score 0). He also developed moderate scarring over donor area (CDA score-2). The result, in our scoring system was considered as fair (total score 9).
Case 9. A 1 2-year-old boy with segmental vitiligo on forehead with leucotrichia of the eyebrows and the frontal scalp hair was treated with MPG. He achieved more than 95% pigmentation by the end of one year (EOP score 15). His leucotrichia part also improved. Color match was excellent (CM score 6). No complications developed. Result was excellent (total score 21).
Case 10. A 21-year-old woman with a segmental vitiligo patch present on the trunk was treated with MPG. She developed more than 90% pigmentation (EOP score 15) with good color match (CM score 3). There was moderate cobblestone appearance (CRA score-3). The overall score was 15 with good result.
Case 11. An 18-year-old girl with vitiligo vulgaris patches on the lower limb was treated with MPG. She developed about 95% pigmentation after one year (EOP score 15), with good color match (CM score 3). The patches however, pigmented with moderate variegated appearance (CRA score-3). The result was considered as good (total score 15).
Case 12. A 24-year-old man with segmental vitiligo on face was treated with MPG. After one year follow-up he developed more than 95% pigmentation (EOP score 15) with excellent color match (CM score 6) and no complications. The result was excellent.
Discussion
It seems at the first observation that disproportionately high weightage has been given to the criteria for extent of pigmentation. However, in the final evaluation remaining three criteria of the color match and the complications of the recipient and the donor site have a greater impact. In the absence of an excellent/good color match, the outcome in our second patient could not exceed beyond the poor/fair category in spite of achieving significant pigmentation. So to achieve an outcome beyond poor category, one has to have 30% or more of maximum possible scoring. The major bulk of scoring for an essentially successful outcome is the high score given to the EOP, which is the most important goal of therapy (the maximum EOP score being 70% of the maximum possible score). The maximum score in the color match criteria is 6, which is about 30% of the maximum possible total score. The degree of color match is important to achieve a higher score category. Thus the seemingly low score of color match (maximum figure of 6) has a significant impact on the final outcome. Our first, second, seventh, tenth and eleventh cases highlight the importance of complications over recipient area in this system. Eighth case highlights that the complications over donor area may affect the outcome evaluation adversely in this system. Nineth and twelfth cases demonstrate that spread of pigmentation over most of the depigmented area with good to excellent color match, in the absence of moderate to severe complications at both recipient and donor areas, result in an excellent outcome. Our suggestion of evaluation of results at least one year after transplantation procedure is justified by our first case. In this case the disease reactivated and affected the results five months after the surgical procedure. Such adverse events can also occur after a period of more than one year but they are rare enough to be ignored. Any vitiligo patch, stable for one year, is less likely to reactivate later.
For any evaluation system to be useful, the outcome variables must be clearly defined, as objectively as is possible and should have adequate clinical and biological significance.[11] We feel that the proposed scoring system fulfils most of these needs. Presently available means cannot make this evaluation system absolutely objective. However, the use of computerised digital image analysis for measuring the extent of pigmentation and colour match[12] may make the scoring system even more objective and may further improve its accuracy. This can eliminate the inter-observer variation in at least first two criteria of our evaluation system.
An unavoidable limitation of our scoring system is variation in the perception of the patient of his problem of vitiligo and complications resulting from surgery. In some pigmented races where vitiligo is a social taboo,[13] the only concern of most patients is the pigmentation. On the other hand, in the light colored races, aesthetic aspects like color match and overall appearance of the lesions are of at least equal significance in addition to the pigmentation. However, we feel that unaffected by the patient′s perception, a scientific evaluation system should consider all four above-mentioned criteria.
| 1. |
Njoo MD, Westerhof W, Bos JD, et al. A systematic review of autologous transplantation methods in vitiligo. Arch Dermatol 1998;134:1543-1549.
[Google Scholar]
|
| 2. |
Falabella R. Repigmentation of stable Leukoderma by autologous mini-grafting. J Dermatol Surg Oncol 1986;12:172-179.
[Google Scholar]
|
| 3. |
Mutalik S. Transplantation of melanocytes by epidermal grafting: an Indian experience. J Dermatol Surg Oncol 1993;19:231-234.
[Google Scholar]
|
| 4. |
Gupta S, Shroff S, Gupta S. Modified technique of suction blistering of epidermal grafting in vitiligo. Int J Dermatol 1999;38:306-309.
[Google Scholar]
|
| 5. |
Khan AM, Cohen MJ. Repigmentation in vitiligo patients. melancocytes transfer via ultra-thin grafts. Dermatol Surg 1998;24:365-367.
[Google Scholar]
|
| 6. |
Olsson MJ, Juhlin L. Leucoderma treated by transplantation of a basal cell layer enriched suspension. Br J Dermatol 1998;138:644-648.
[Google Scholar]
|
| 7. |
Lerner AB, Halaban R, Klaus SN, et al. Transplantation of human melanocytes. J Invest Dermatol 1987;89:219-224.
[Google Scholar]
|
| 8. |
Platt RT, Brysk MM, Newton RC, et al. A surgical treatment for vitiligo: autologous cultured epithelial grafts. J Dermatol Surg Oncol 1989;15:1161-1166.
[Google Scholar]
|
| 9. |
Ladhoni S.The need for evidence-based management of skin diseases. Int J Dermatol 1997;36:17-22.
[Google Scholar]
|
| 10. |
Hann SK, Im S, Bong HW, et al. Treatment of stable vitiligo with autologous epidermal grafting and PUVA. J Am Acad Dermatol 1995;32:943-948.
[Google Scholar]
|
| 11. |
Bigby M, Gadenne AS. Understanding and evaluating clinical trials. J Am Acad Dermatol 1996;34:555-590.
[Google Scholar]
|
| 12. |
Boersma BR, Westerhof W, Bos JD. Repigmentation in vitiligo by autologous minigrafting: Results in nineteen patients. J Am Acad Dermatol 1995;33:990-995.
[Google Scholar]
|
| 13. |
Mosher DB, Fitzpatrick TB, Hori V, et al. Disorders of pigmentation. In:Fitzpatrick TB, Eisen AZ, Wolff K, et al, eds. Dermatology in General Medicine. 4'ed. New York NY:McGraw Hill Inc; 1993:903.
[Google Scholar]
|





![[Table - 1]](#tbl_ijdvl_2002_68_1_33_12863_1.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2002_68_1_33_12863_2.jpg){kind=link}