Translate this page into:
A rare presentation of keratosis follicularis spinulosa decalvans in female twins
Correspondence Address:
Saumya Sankhwar
Department of Dermatology and Venereology, Institute of Medical Sciences, Banaras Hindu University, Varanasi - 221 005, Uttar Pradesh
India
| How to cite this article: Chauhan RK, Sankhwar S, Tripathi R, Pandey S S. A rare presentation of keratosis follicularis spinulosa decalvans in female twins. Indian J Dermatol Venereol Leprol 2018;84:645 |
Sir,
A 9-year-old pair of monozygotic twin sisters, born of spontaneous, full-term normal vaginal delivery, visited the dermatology outpatient department of Sir Sunderlal Hospital, Banaras Hindu University, Varanasi, with the absence of body and scalp hair since birth. There was no history of consanguinity in parents. Parents were using various homemade remedies for the condition, on-and-off, including ayurvedic treatment, since 1 year of age. Some hairs appeared on the scalp one year later and they were persistent [Figure - 1] and [Figure - 2]a. Examination revealed small, discrete, spiny papules with follicular plugging, present on normal looking skin on the body [Figure - 2]b. Oral mucosa, teeth, nails, palms and soles were found to be normal. There was no history of photophobia. Ophthalmic examination revealed no abnormal findings. Routine hematological and other laboratory studies were within normal limits. Hair microscopy was done to rule out hair shaft defects.
 |
| Figure 1: Female twins with follicular papules and some hair on the scalp |
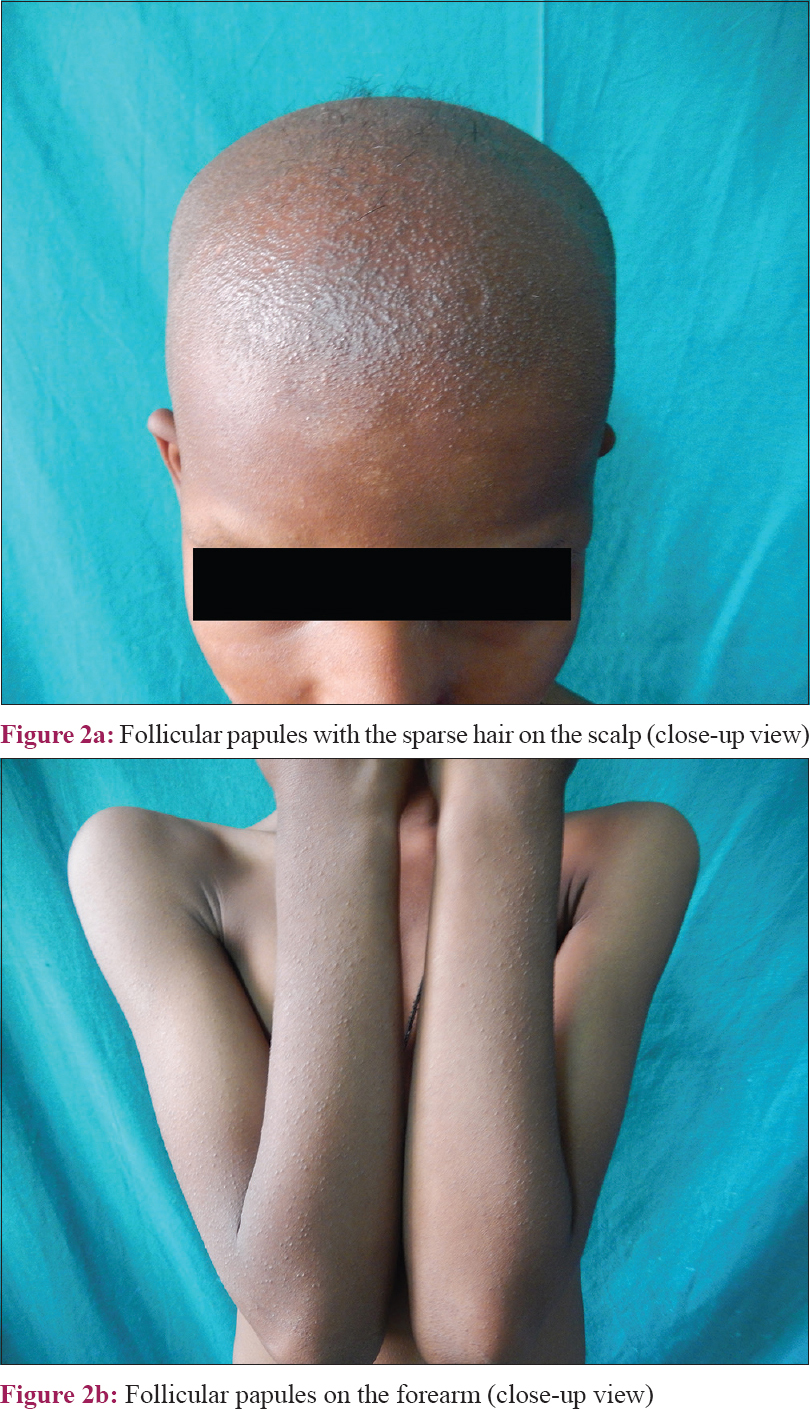 |
| Figure 2 |
Histopathological examination of the hairy areas such as the scalp and extensor aspect of the left forearm showed sparse superficial perivascular and periappendageal lymphocytic infiltrates with no epidermal changes. Some of the follicular infundibula were dilated and plugged with orthokeratotic corneocytes while others showed mild spongiosis. There was dense perifollicular fibroplasia in some follicles and the terminal follicles were reduced in number on the scalp skin [Figure - 3] and [Figure - 4]. Based on these clinical and histopathological findings, these cases were diagnosed as keratosis follicularis spinulosa decalvans.
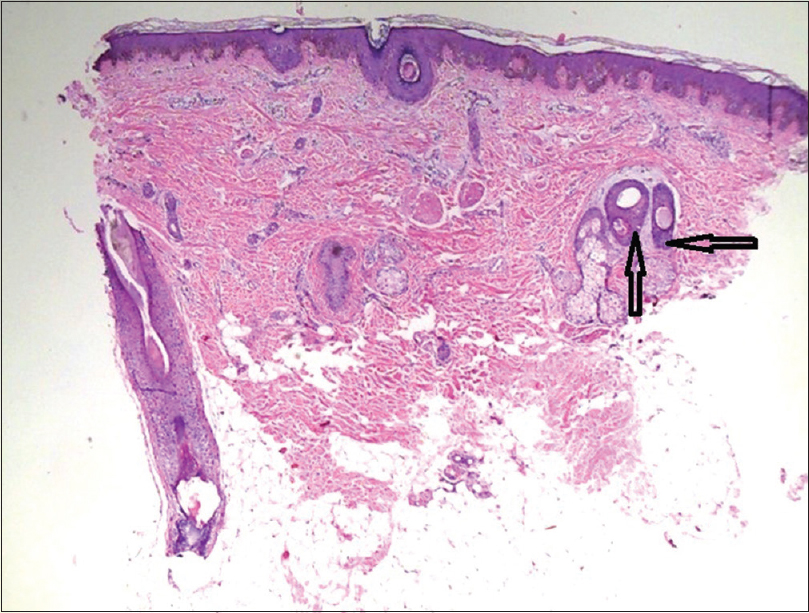 |
| Figure 3: Perifollicular fibroplasia and lymphocytic infiltrate (arrowheads) in other fields on scalp histopathology (H and E, ×100) |
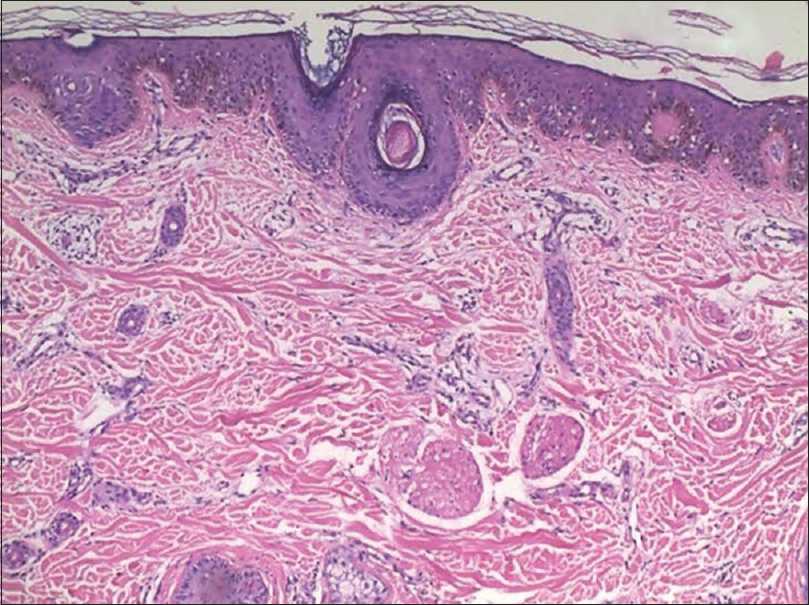 |
| Figure 4: Dilated follicular infundibula plugged with orthokeratotic corneocytes and perivascular, periappendageal lymphocytic infiltrate on scalp histopathology (H and E, ×400) |
Keratosis follicularis spinulosa decalvans is a rare, X-linked, hereditary disorder of keratinization, characterized by the involvement of the skin and eyes. Keratosis follicularis spinulosa decalvans was first described as an X-linked dominant disorder.[1] However, in some cases, an autosomal dominant and sporadic inheritance have also been reported. The term was first used by Siemens in 1926, who described some individuals from a Bavarian family who presented with follicular papules on the face, trunk and extremities with partial loss of hairs; thus, the disease is also known as Siemens syndrome.[1] Genetic studies in Dutch and English families have showed connection with the Xp21.2-p22 gene.[2] When the inheritance pattern is X-linked, males are predominantly affected and females are mostly carriers. Females with severe forms of the disease have also been reported. These cases either had an autosomal dominant pattern of inheritance or some were sporadic in onset. A theory of non-random X-inactivation (process of lyonization) was proposed in cases with sporadic onset.[3] As there is no positive family history and since the disease is rare and present in female twins, our case likely has either an autosomal dominant inheritance or heterogeneous transmission with sporadic inheritance, which is one of the four reported patterns of inheritance in literature.[4] Our patients also had the characteristic cutaneous and histological features of keratosis follicularis spinulosa decalvans. However, there were no other associated abnormalities such as ocular changes, deafness, physical and mental retardation, hypoplastic nails and palmoplantar keratoderma, as described in literature.[3],[4] Moreover, the presence of scarring alopecia on the scalp [Figure - 2]a and the lack of ophthalmological abnormalities differentiate it from ichthyosis follicularis alopecia and photophobia syndrome, where there is nonscarring alopecia and photophobia that presents either at birth, in infancy or in early childhood.[3] Furthermore, in this case, while there was complete alopecia at birth, some hairs appeared on the scalp with time that are still persisting; which helped to differentiate this from the condition- congenital atrichia with papules, where there is permanent and complete alopecia by the first few months of life and no hair regrowth occurs with the passage of time.[5] Clinically, our patients did not have any bony pain or deformities and there was no decreased muscle tone and the levels of alkaline phosphatase, serum calcium and vitamin D were within normal limits, thus ruling out rickets. Other differentials such as lichen spinulosus and lichen planopilaris were excluded on the basis of histopathological findings.
There is no specific treatment for this disorder. However, drugs such as isotretinoin and dapsone have been tried; emollients, topical corticosteroids and keratolytic agents can be used for symptomatic relief.[3] Although it is a rare genodermatosis, keratosis follicularis spinulosa decalvans should always be considered in all cases of hyperkeratosis with alopecia. Genetic counseling is needed in some cases and the treatment should be started as early as possible so as to retard and minimize sequelae such as cicatrization.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the legal guardian has given his/her consent for images and other clinical information to be reported in the journal. The guardian understands that names and initials will not be published and due efforts will be made to conceal patient identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Siemens HW. Keratosis follicularis spinulosa decalvans. Arch Derm Syphilol (Berlin) 1926;151:384.
[Google Scholar]
|
| 2. |
Oosterwijk JC, Nelen M, van Zandvoort PM, van Osch LD, Oranje AP, Wittebol-Post D, et al. Linkage analysis of keratosis follicularis spinulosa decalvans, and regional assignment to human chromosome Xp21.2-p22.2. Am J Hum Genet 1992;50:801-7.
[Google Scholar]
|
| 3. |
Maheswari UG, Chaitra V, Mohan SS. Keratosis follicularis spinulosa decalvans: A rare cause of scarring alopecia in two young Indian girls. Int J Trichology 2013;5:29-31.
[Google Scholar]
|
| 4. |
Castori M, Covaciu C, Paradisi M, Zambruno G. Clinical and genetic heterogeneity in keratosis follicularis spinulosa decalvans. Eur J Med Genet 2009;52:53-8.
[Google Scholar]
|
| 5. |
Yip L, Horev L, Sinclair R, Zlotogorski A. Atrichia with papular lesions: A report of three novel human hairless gene mutations and a revision of diagnostic criteria. Acta Derm Venereol 2008;88:346-9.
[Google Scholar]
|
Fulltext Views
2,562
PDF downloads
1,346





![[Figure - 1]](#fig_ijdvl_2018_84_5_645_213709_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_5_645_213709_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2018_84_5_645_213709_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2018_84_5_645_213709_f4.jpg){kind=link}