Translate this page into:
A verrucous plaque on the intergluteal cleft
2 Department of Pathology, Hospital Regional Universitario de Malaga, Malaga, Spain
Correspondence Address:
E G�mez Moyano
Department of Dermatology, Plaza Hospital Civil s/n, 29010 Malaga
Spain
| How to cite this article: Fern�ndez Ballesteros M D, G�mez Moyano E, Ayala Blanca M, Simonsen S. A verrucous plaque on the intergluteal cleft. Indian J Dermatol Venereol Leprol 2018;84:641-642 |
We present a case of a 48-year-old man with no relevant personal or family history, who reported a pruriginous lesion in the gluteal cleft of 14 months duration. Physical examination showed a brownish-pink, verruciform plaque with a raised, hyperkeratotic border, 2 cm in diameter, located in the upper region of the gluteal cleft [Figure - 1].
 |
| Figure 1: Verrucous plaque with a prominent ridge-like border on the natal cleft |
A biopsy was taken with the differential diagnosis of squamous cell carcinoma versus condyloma acuminata. Histological study of the lesion revealed moderate hyperkeratosis associated with verruciform epidermal hyperplasia with significant elongation of the crests [Figure - 2], as well as a column of parakeratosis, the lower vertex of which was situated on a reduced granular layer and dyskeratotic, vacuolated keratinocytes.
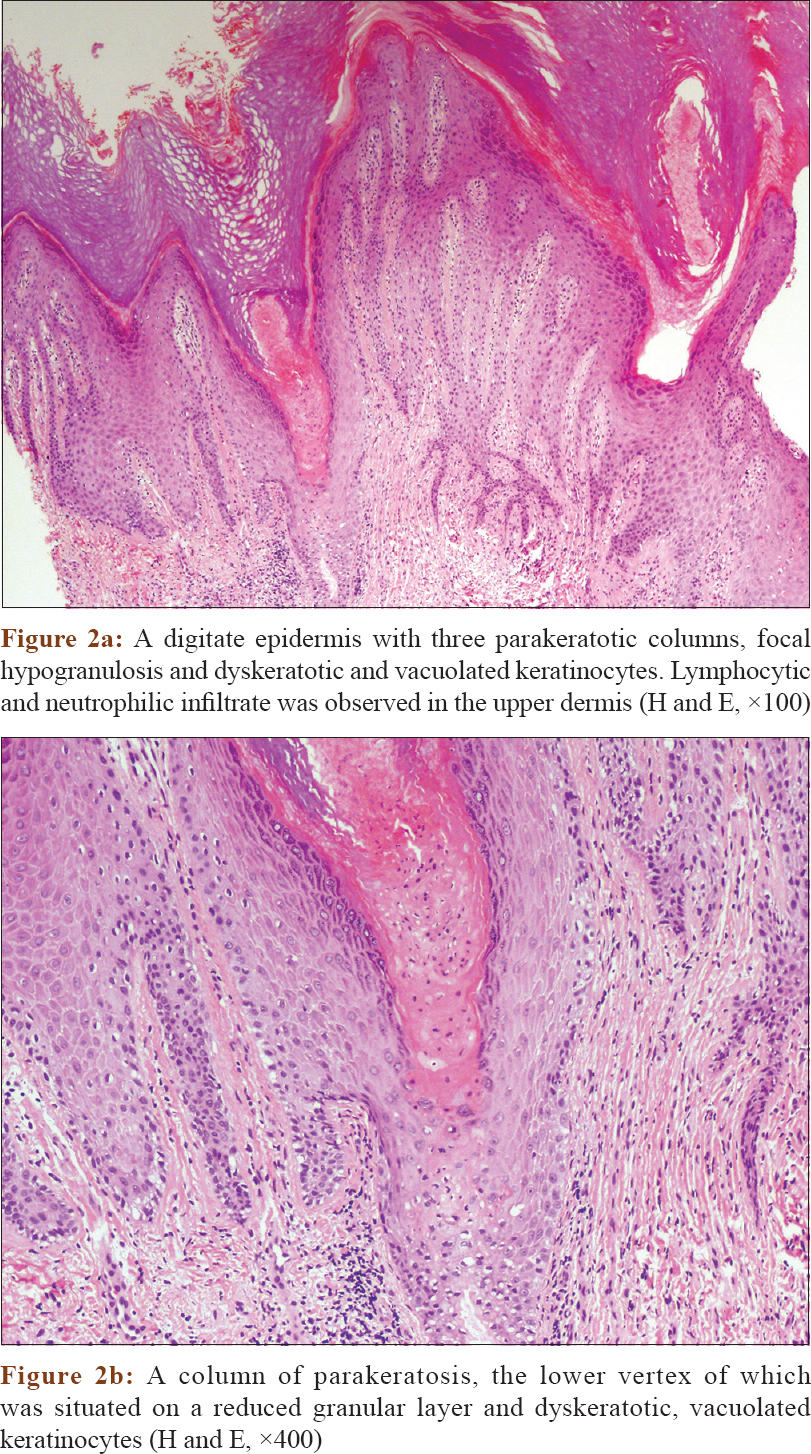 |
| Figure 2 |
No amyloid deposition was observed.
What Is Your Diagnosis?
Answer
Verrucous porokeratosis.
Discussion
Treatment with a retinoid cream at 0.05% daily for 2 months was started without improvement. Cryosurgery was performed, but the lesion remained. Surgical removal is planned.
Porokeratosis is a primary disorder of epidermal keratinization. Classically, there are five variants: punctate porokeratosis, porokeratosis of Mibelli, linear porokeratosis, disseminated superficial actinic porokeratosis and porokeratosis palmaris et plantaris disseminata.[1],[2] However, verrucous porokeratosis of the gluteal cleft is unknown and we can postulate its probable underdiagnosis due to confusion with other entities.[2]
The first reported case was presented by Lucher in 1995, who named it ptychotropic porokeratosis, using two Greek terms, ptythe (cleft) and trope (change or alteration);[3] the next case was published by Stone in 1999.[4] Other descriptions include “hyperkeratotic variant of porokeratosis,” “verrucous porokeratosis of Mibelli on the buttocks,” “follicular porokeratosis of Mibelli on the buttocks,” “hypertrophic perianal porokeratosis” and “genitogluteal porokeratosis.” The unifying term “verrucous porokeratosis” is proposed.[2]
Till now, 35 cases have been described with a clear male predominance (32 men, 3 women).[1],[2],[3],[4],[5] The etiology is unknown, but there appears to be a genetic susceptibility with triggering factors such as repeated trauma to the area.[5]
This variant is characterized by a series of clinical and histological peculiarities. Clinically, it starts as small hyperkeratotic papules with a tendency to join and extend symmetrically on both buttocks, forming a pink verrucous plaque in the shape of butterfly wings with peripheral satellite lesions, accompanied by intense pruritus.[1],[2],[3],[4] Unlike other variants of porokeratosis, malignant transformation has not been described so far, but it cannot be ruled out completely in porokeratosis.[2],[5]
In the histological study, there is typically a marked epidermal hyperplasia and multiple concentric cornoid lamellae.[1],[5] We found only two cases of a hyperkeratotic variant of porokeratosis with dermal amyloid deposits.[5]
The relationship between dermal amyloid deposits and porokeratosis remains unclear, however it seems that the deposits are secondary to the epidermal defect.[5]
This form of porokeratosis may lead to diagnostic doubts with condyloma acuminata, inverted psoriasis, candidiasis of the cleft, lichen sclerosus or tinea corporis.[1],[2]
Different treatments have been attempted, both ablative (surgical removal, cryosurgery and CO2 laser) and nonablative (topical imiquimod, topical and systemic retinoids and 5-fluorouracil), but none has yet shown acceptable effectiveness.[2]
In conclusion, verrucous porokeratosis of the gluteal cleft is a nonvenereal diagnosis to consider when evaluating anogenital lesions in men. Recognition of this rare disease is important due to the prognostic and therapeutic implications associated with a correct diagnosis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Tallon B, Blumental G, Bhawan J. Porokeratosis ptychotropica: A lesser-known variant. Clin Exp Dermatol 2009;34:895-7.
[Google Scholar]
|
| 2. |
Takiguchi R, White K, White C, Simpson E. Verrucous porokeratosis of the gluteal cleft (porokeratosis ptychotropica): A rare disorder easily misdiagnosed. J of Pathol 2010;37:802-7.
[Google Scholar]
|
| 3. |
Lucker GP, Happle R, Steijlen PM. An unusual case of porokeratosis involving the natal cleft: Porokeratosis ptychotropica? Br J Dermatol 1995;132:150.
[Google Scholar]
|
| 4. |
McGuigan K, Shurman D, Campanelli C, Lee J. Porokeratosis ptychotropica: A clinically distinct variant of porokeratosis. J Am Acad Dermatol 2008;60:501-3.
[Google Scholar]
|
| 5. |
Uenishi T, Teramura K, Kitamura M, Fujii N, Nakanishi G, Tanaka T, et al. Hyperkeratotic variant of porokeratosis Mibelli with dermal amyloid deposits. Journal of Dermatology 2010;37:475-9.
[Google Scholar]
|
Fulltext Views
4,301
PDF downloads
2,454





![[Figure - 1]](#fig_ijdvl_2018_84_5_641_215649_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_5_641_215649_f2.jpg){kind=link}