Translate this page into:
Acral syringomas associated with hematological neoplasm
Correspondence Address:
Eduardo Varas-Meis
Department of Dermatology, Complejo Asistencial Universitario de León, Altos de Nava, s/n, León 24080
Spain
| How to cite this article: Varas-Meis E, Prada-García C, Samaniego-González E, Rodríguez-Prieto M&. Acral syringomas associated with hematological neoplasm. Indian J Dermatol Venereol Leprol 2017;83:136 |
Sir,
Syringomas are benign acrosyringeal tumors that typically manifest in adolescent and middle-aged women as asymptomatic, flat or dome-shaped, yellowish-brown papules located on the lower eyelids. Their underlying etiology is unknown. Acral syringomas are rare in the medical literature. Unlike typical clinical syringomas, they have been described in older patients with no gender predominance and are associated with tumor pathology.
A 62-year-old woman with a history of invasive breast cancer, diagnosed 17 years ago, was treated with surgery, radiation therapy and tamoxifen and had suffered no relapses. She was also diagnosed with promyelocytic leukemia 2 years ago and was treated with oral methotrexate, mercaptopurine and tretinoin, but has been in complete remission. She did not have any dermatological disorders till then.
She sought a dermatology consultation when she developed multiple, asymptomatic brownish, non-follicular, confluent and symmetrical papules on the anterior side of both forearms and periocular area over the course of 2 years [Figure - 1]. The lesions began shortly after the hematological diagnosis and before the initiation of anti-neoplastic treatment.
 |
| Figure 1a: Normal coloured to brownish papular, flat and smooth, confluent lesions of symmetrical distribution on anterior side of both wrists |
 |
| Figure 1b: Normal coloured to brownish papular, flat and smooth, confluent lesions of symmetrical distribution on both lower eyelids |
 |
| Figure 1c: Normal coloured to brownish papular, flat and smooth, confluent lesions of symmetrical distribution on detailed lesions on forearm |
The histopathological examination showed glandular structures in the superficial dermis composed of double-cell layer tubular structures with no atypia or mitosis within an eosinophilic stroma [Figure - 2]. Congo red staining was negative. Immunohistochemistry was negative for estrogen receptors, slightly positive for epithelial membrane antigen in the periphery and positive for carcinoembryonic antigen and p63 [Figure - 3]. The findings were compatible with syringoma.
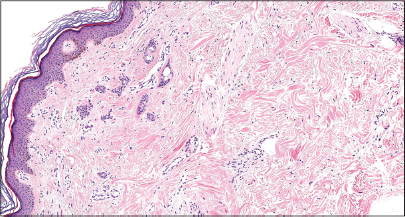 |
| Figure 2: Glandular infiltration into the superficial dermis (H and E, ×40) |
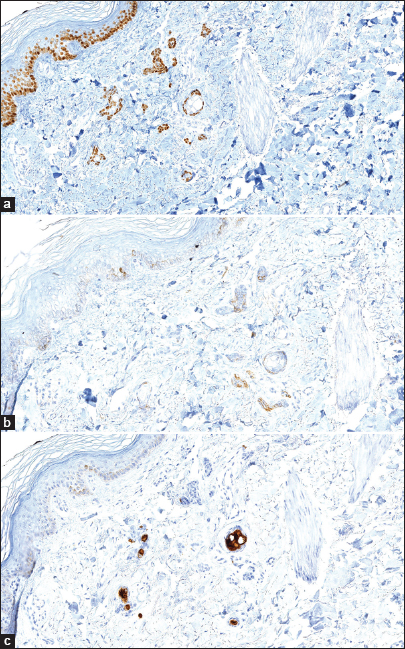 |
| Figure 3: (a) Immunohistochemistry with p63 positive (×40). (b) Immunohistochemistry with slightly EMA positive (×40). (c) Immunohistochemistry with tubular lumen CEA positive result (×40) |
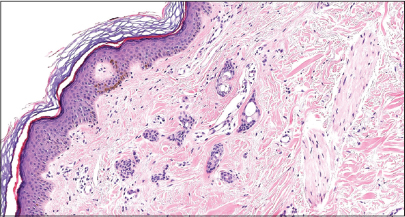 |
| Figure 3d: Detailed tubular infiltration (H and E, ×40) |
In the 2-year follow-up period, no recurrence of the hematological neoplasm was noted, but cutaneous lesions remain unchanged.
Syringomas are benign tumors of the acrosyringium. Clinically, they usually appear as flat or dome-shaped, yellowish-brown papules, located in the lower palpebral area of young to middle-aged women. The etiology is unknown. Friedman and Butler have classified them into four variants based on the clinical picture: localized, associated with Down's syndrome, generalized eruptive syringomas and an autosomal dominant familial form.[1] Syringomas have also been described in multiple atypical sites such as the trunk, upper and lower extremities, buttocks and genitals.[2],[3],[4],[5],[6]
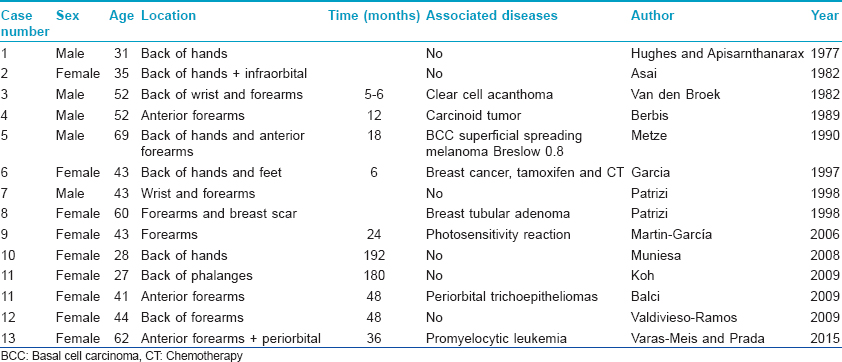
Syringomas of acral location, affecting the distal end of the extremities, are rare in the medical literature. There have only been 13 cases published to date [Table - 1]. They differ from typical palpebral syringomas because they appear in older patients, affect both sexes equally and are frequently associated with tumor pathology.[7] Cases of acral syringomas associated with syringomas of typical bilateral infraorbital location have also been described.
Histologically, they appear as glandular cords and ducts in the superficial dermis, composed of a double cell layer with no atypia, in a collagenous and homogeneous stroma. Some cells may show eccentric prolongations, when they are typically compared to 'comma' or 'tadpole tail-shaped' structures.
The clinical differential diagnosis includes lichenoid eruptions, mastocytosis, sarcoidosis, granuloma annulare and other granulomatous processes.
The lesions do not require treatment except for esthetic or symptomatic reasons. Surgical excision, cryotherapy, electrocoagulation, topical atropine, tretinoin and CO2, erbium-yttrium aluminum garnet, argon, or pulsed dye lasers have been used with inconsistent results.[3],[7],[13]
We were unable to find any previous reports of syringomas associated with hematological neoplasms which may be a triggering factor in the appearance of these lesions but are independent of evolution. However, this could only be a coincidental association.
The mechanisms leading to the development of these lesions remain unclear. The immunosuppression and the hyperproliferative state associated with the hematological neoplasm could contribute to this atypical presentation of the syringomas. Although the association of acral syringoma and breast cancer has been reported, the 17-year difference in the presentation of our case prompted us to consider it as a coincidental finding.[11]
In conclusion, we believe, like other authors, that acral syringomas should constitute an independent class within the original classification of Friedman and Butler due to their unique clinical characteristics.[4],[7],[12]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Friedman SJ, Butler DF. Syringoma presenting as milia. J Am Acad Dermatol 1987;16(2 Pt 1):310-4.
[Google Scholar]
|
| 2. |
Balci DD, Atik E, Altintas S. Coexistence of acral syringomas and multiple trichoepitheliomas on the face. J Cutan Med Surg 2009;13:169-71.
[Google Scholar]
|
| 3. |
Koh MJ. Multiple acral syringomas involving the hands. Clin Exp Dermatol 2009;34:e438.
[Google Scholar]
|
| 4. |
Martín-García RF, Muñoz CM. Acral syringomas presenting as a photosensitive papular eruption. Cutis 2006;77:33-6.
[Google Scholar]
|
| 5. |
Metze D, Jurecka W, Gebhart W. Disseminated syringomas of the upper extremities. Case history and immunohistochemical and ultrastructural study. Dermatologica 1990;180:228-35.
[Google Scholar]
|
| 6. |
van den Broek H, Lundquist CD. Syringomas of the upper extremities with onset in the sixth decade. J Am Acad Dermatol 1982;6 (4 Pt 1):534-6.
[Google Scholar]
|
| 7. |
Valdivielso-Ramos M, de la Cueva P, Gimeno M, Hernanz JM. Acral syringomas. Actas Dermosifiliogr 2010;101:458-60.
[Google Scholar]
|
| 8. |
Asai Y, Ishii M, Hamada T. Acral syringoma: Electron microscopic studies on its origin. Acta Derm Venereol 1982;62:64-8.
[Google Scholar]
|
| 9. |
Hughes PS, Apisarnthanarax P. Acral syringoma. Arch Dermatol 1977;113:1435-6.
[Google Scholar]
|
| 10. |
Berbis P, Fabre JF, Jancovici E, Privat Y, Benderitter T. Late-onset syringomas of the pper extremities associated with a carcinoid tumor. Arch Dermatol 1989;125:848-9.
[Google Scholar]
|
| 11. |
Garcia C, Krunic AL, Grichnik J, Viehman G, Clark RE. Multiple acral syringomata with uniform involvement of the hands and feet. Cutis 1997;59:213-4, 216.
[Google Scholar]
|
| 12. |
Patrizi A, Neri I, Marzaduri S, Varotti E, Passarini B. Syringoma: A review of twenty-nine cases. Acta Derm Venereol 1998;78:460-2.
[Google Scholar]
|
| 13. |
Muniesa C, Fortuño Y, Moreno A, González J. Papules on the dorsum of the fingers. Actas Dermosifiliogr 2008;99:812-3.
[Google Scholar]
|
Fulltext Views
3,199
PDF downloads
2,754





![[Figure - 1]](#fig_ijdvl_2017_83_1_136_192961_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2017_83_1_136_192961_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2017_83_1_136_192961_f3.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2017_83_1_136_192961_t7.jpg){kind=link}