Translate this page into:
Actinomycotic mycetoma of the hand: A rare occurrence
Correspondence Address:
Vandana Mehta Rai
Department of Skin and STD, Kasturba Medical College and Hospital, Manipal 576 104, Karnataka
India
| How to cite this article: Rai VM, Balachandran C. Actinomycotic mycetoma of the hand: A rare occurrence. Indian J Dermatol Venereol Leprol 2006;72:178 |
 |
|
 |
|
 |
|
Sir,
Mycetoma is a chronic suppurative granulomatous disorder of subcutaneous tissues and bones characterized by localized swellings with multiple sinus tracts discharging granules that are microcolonies of the causative agent. John Gill in 1842 described its clinical features for the first time and named it ′Madura foot′ after the region of Madurai in India, where it was first identified. It may be caused by either actinomycetes (actinomycotic mycetoma) or true fungi (eumycetoma). The foot is most commonly affected. We report a case of actinomycotic mycetoma of the hand for its rarity.
A 41-year-old male laborer presented with the complaint of a diffuse swelling with multiple discharging nodules on the thenar eminence of the right palm involving the first web space and dorsal aspect of the right hand of 6 years duration [Figure - 1]. At the onset, there was a single papule. It was excised and was followed by the development of multiple discharging nodules at the same site. The patient could not recollect any history of trauma. He was diagnosed as mycetoma outside and had been treated with dapsone 100 mg daily and antibiotics (amoxycillin-clavulanic acid 625 mg BD followed by doxycycline 100 mg BD) for 2 months without any response.
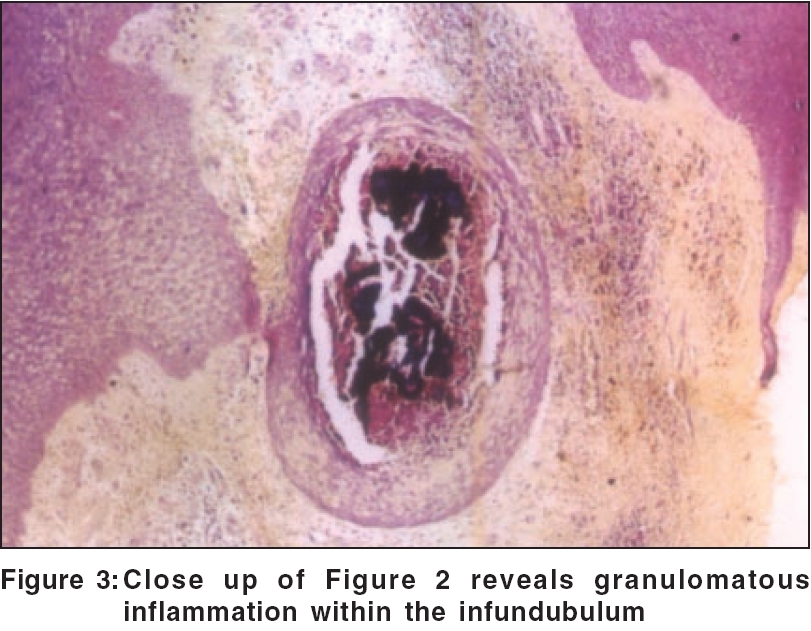
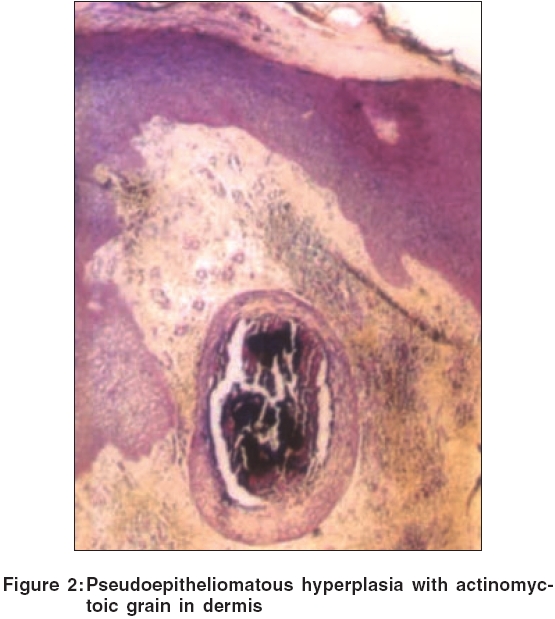
Routine hematological and biochemical investigations were normal. A biopsy showed pseudoepitheliomatous hyperplasia with abscess cavities in the dermis containing sulfur granules that showed a gram-positive reaction [Figure - 2][Figure - 3]. Bacterial culture grew Streptomyces spp. Rontgenogram of right hand showed juxta-articular osteopenia. Our patient was treated with cotrimoxazole 960 mg twice daily for 2 months followed by one tablet for 3 months, amikacin 250 mg intravenous BD for one week and rifampicin 600mg once daily for 4 months with which the lesions on the palm and dorsa of hand flattened. There was neither any further discharge nor any development of new lesions.
Actinomycetomas are caused by aerobic actinomycetes belonging to the genera Nocardia , Streptomyces and Actinomadura . Although reported from all over the world, they are common in tropical and subtropical regions where people walk barefoot. In India, actinomycotic mycetoma is more commonly encountered than eumycotic mycetoma.[1] However, the latter account for most of the cases reported from northern India. Actinomadura pelletieri is rarely seen in northern India and most of the cases reported are from Tamil Nadu. The body part affected most commonly is the foot, with involvement of the dorsal aspect of the forefoot being typical. However, other areas of the body may also be involved.[2],[3],[4] Combination therapy is recommended for treatment because of its synergistic effects and decreased likelihood of the development of resistance. In mycetomas due to streptomyces, streptomycin has been successfully used in combination with dapsone or sulfamethoxazole.[5] Our patient did not respond to dapsone and antibiotics given for 2 months. This combination was later substituted by amikacin, cotrimoxazole[6] and daily rifampicin with which there was flattening of the lesions.
| 1. |
Venugopal TV, Venugopal PV, Paramasivan CN. Mycetomas in Madras. Sabouraudia 1977;15:17-23.
[Google Scholar]
|
| 2. |
Baril L, Boiron P, Manceron V. Refractory craniofacial actinomycetoma due to streptomyces somaliensis that required salvage therapy with amikacin and imipenem. Clin Infect Dis 1999;29:460-1.
[Google Scholar]
|
| 3. |
Tritten JJ, Uffer S. Actinomycetes granuloma of the upper eyelid. Klin Monatsbl Augenheilkd 1997;210:339-40. [PUBMED abstract]
[Google Scholar]
|
| 4. |
Pulikot AM, Bapat SS, Tolat S. Mycetoma of the sole. Ann Trop Paediatr 2002;22:187-90.
[Google Scholar]
|
| 5. |
Mahgoub ES. Medical management of mycetoma. Bulletin of the WHO 1976;54:303-10.
[Google Scholar]
|
| 6. |
Welsch O, Sauceda E, Gonzalez J. Amikacin alone and in combination with Trimethoprim-sulphamethoxazole in the treatment of actinomycotic mycetoma. J Am Acad Dermatol 1987;17:443.
[Google Scholar]
|
Fulltext Views
2,882
PDF downloads
3,005





![[Figure - 1]](#fig_ijdvl_2006_72_2_178_25661_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2006_72_2_178_25661_2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2006_72_2_178_25661_3.jpg){kind=link}