Translate this page into:
Allergic contact dermatitis due to clotrimazole with cross-reaction to miconazole
Correspondence Address:
Vikram K Mahajan
Department of Dermatology, Venereology and Leprosy, Dr. R. P. Government Medical College, Kangra (Tanda) - 176 001, Himachal Pradesh
India
| How to cite this article: Abhinav C, Mahajan VK, Mehta KS, Chauhan PS. Allergic contact dermatitis due to clotrimazole with cross-reaction to miconazole. Indian J Dermatol Venereol Leprol 2015;81:80-82 |
Sir,
Allergic contact sensitivity from imidazoles is uncommon, when viewed in proportion to their widespread use in various concentrations and preparations (cream, gel, lotion, shampoo, or dusting powder) for topical treatment of dermatophytosis. Miconazole, econazole, tioconazole, and isoconazole have been the most commonly reported causes of contact sensitivity among all the topical imidazoles. Although clotrimazole, miconazole, and ketoconazole are prescribed more frequently than other imidazoles, allergic contact sensitivity due to clotrimazole with cross-reactivity to miconazole is rare.
A 44-year-old male patient suffering from tinea cruris was prescribed oral fluconazole (200 mg/week) and clotrimazole cream (1%) for twice-daily application. A day after topical clotrimazole application, he developed acute dermatitis over the scrotum and both groins. He had used clotrimazole cream on two occasions in the past for tinea cruris. He did have exacerbation of redness and itching on the second occasion; however, he had not reported it then. In the present instance, suspecting acute allergic contact dermatitis from clotrimazole, it was withdrawn and he continued taking oral fluconazole. His dermatitis resolved 1 week after he was started on oral prednisolone (30 mg/day), oral cetirizine (10 mg/day), and plain water compresses. Patch testing was performed after 3 weeks by Finn chamber method with Indian standard series [1] along with the most commonly prescribed and commercially available topical antifungal preparations in an undiluted form [Table - 1]. Among the above, clotrimazole and miconazole elicited 3 + and 2 + positive patch test reactions, respectively [Figure - 1].
 |
| Figure 1: Positive patch test reactions from clotrimazole (3+) and miconazole (2+) at D3 |
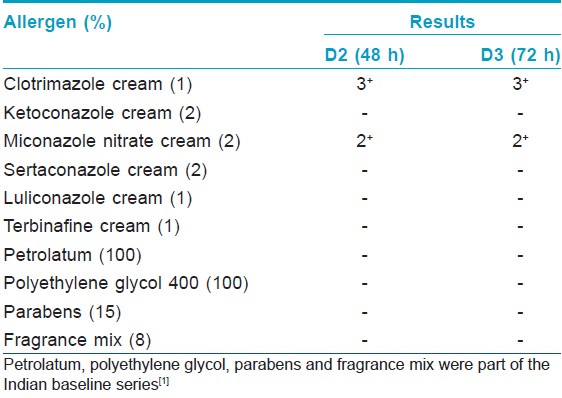
Imidazoles, the most frequently prescribed topical antifungal drugs, comprise two major groups that is, phenethyl imidazoles (ketoconazole, miconazole, tioconazole, isoconazole, enilconazole, econazole, sulconazole, sertaconazole, oxiconazole) and phenmethyl imidazoles (clotrimazole, croconazole, bifonazole). Allergic contact sensitivity from imidazoles is uncommon, and most of the available data are from case reports or a few case series. Miconazole has been the most frequently reported contact sensitizer. [2],[3],[4],[5],[6],[7],[8] Raulin and Frosch [8] noted patch test positivity to miconazole in six of nine patients with imidazole contact allergy, while only three patients each showed positivity to clotrimazole, econazole, and isoconazole. Dooms-Goossens et al. [7] also noted 51 (54%) patch test positive reactions to miconazole in 94 tested cases of suspected imidazole contact sensitivity. Econazole, tioconazole, and isoconazole were other common sensitizers depending upon the local prescribing habits and their availability. However, clotrimazole remains a relatively uncommon contact sensitizer despite its widespread use and over the counter availability. There are a few reports of clotrimazole contact allergy in the English medical literature. [3],[7],[8],[9],[10],[11],[12],[13] Cross-reactions are more common among phenethyl imidazoles than phenmethyl imidazoles and occur frequently between the following groups: (1) sulconazole, miconazole , and econazole, (2) isoconazole and tioconazole , (3) miconazole , econazole, and isoconazole, and (4) ketoconazole and miconazole. [7],[8],[14] Cross-sensitivity is much rarer with clotrimazole and ketoconazole due to their relatively different chemical structure. [10] However, cross sensitivity is common between miconazole, isoconazole and econazole, and between sertaconazole, miconazole and econazole as being nitrates they are similar structurally. [8],[15] Although cross-sensitivity between clotrimazole and other azoles (croconazole, bifonazole, isoconazole, tioconazole) occurs, cross-sensitivity between clotrimazole and miconazole is rare and was observed in only 3 of 105 reviewed cases. [7] This overall low allergenicity of clotrimazole, direct or by cross-sensitization, has been attributed to its non-nitrate molecular structure. [3] Our patient had developed contact dermatitis from topical clotrimazole and showed patch test positivity to both clotrimazole and miconazole. Interestingly, clotrimazole also elicited stronger reaction than miconazole despite the fact that clotrimazole is considered to have lower sensitizing potential than miconazole. The negative patch test results from petrolatum, propylene glycol or parabens, the commonly used vehicles/preservatives in commercial preparations, excluded the possibility of contact sensitivity from the vehicle or other constituents. Although this cross sensitivity between clotrimazole (a phenmethyl azole) and miconazole (a phenethyl azole) appears unlikely in view of their structural dissimilarity, crossover sensitivity to imidazoles from different groups remains a possibility according to previous reports in the literature. [16] Therefore, the possibility of sensitization to miconazole from an over-the-counter preparation used in the past cannot be ruled out entirely.
| 1. |
Sharma VK, Sethuraman G, Garg T, Verma KK, Ramam M. Patch testing with the Indian standard series in New Delhi. Contact Dermatitis 2004;51:319-21.
[Google Scholar]
|
| 2. |
Van Ketel WG. Allergy to miconazole nitrate (Daktarin). Contact Dermatitis Newsletter 1974;16:517.
[Google Scholar]
|
| 3. |
Jelen G, Tennstedt D. Contact dermatitis from topical imidazole antifungals: 15 new cases. Contact Dermatitis 1989;21:6-11.
[Google Scholar]
|
| 4. |
Degreef H, Verhoeve L. Contact dermatitis to miconazole nitrate. Contact Dermatitis 1975;1:269-70.
[Google Scholar]
|
| 5. |
Perret CM, Happle R. Contact allergy to miconazole. Contact Dermatitis 1988;19:75.
[Google Scholar]
|
| 6. |
Foged EK, Hammershøy O. Contact dermatitis due to miconazole nitrate. Contact Dermatitis 1982;8:284.
[Google Scholar]
|
| 7. |
Dooms-Goossens A, Matura M, Drieghe J, Degreef H. Contact allergy to imidazoles used as antimycotic agents. Contact Dermatitis 1995;33:73-7.
[Google Scholar]
|
| 8. |
Raulin C, Frosch PJ. Contact allergy to imidazole antimycotics. Contact Dermatitis 1988;18:76-80.
[Google Scholar]
|
| 9. |
Roller JA. Contact allergy to clotrimazole. Br Med J 1978;2:737.
[Google Scholar]
|
| 10. |
Erdmann S, Hertl M, Merk HF. Contact dermatitis from clotrimazole with positive patch-test reactions also to croconazole and itraconazole. Contact Dermatitis 1999;40:47-8.
[Google Scholar]
|
| 11. |
Valsecchi R, Pansera B, di Landro A, Cainelli T. Connubial contact sensitization to clotrimazole. Contact Dermatitis 1994;30:248.
[Google Scholar]
|
| 12. |
Balato N, Lembo G, Nappa P, Ayala F. Contact dermatitis from clotrimazole. Contact Dermatitis 1985;12:110.
[Google Scholar]
|
| 13. |
Kalb RE, Grossman ME. Contact dermatitis to clotrimazole. Cutis 1985;36:240-2.
[Google Scholar]
|
| 14. |
Imafuku S, Nakayama J. Contact allergy to ketoconazole cross-sensitive to miconazole. Clin Exp Dermatol 2009;34:411-2.
[Google Scholar]
|
| 15. |
Goday JJ, Yanguas I, Aguirre A, Ilardia R, Soloeta R. Allergic contact dermatitis from sertaconazole with cross-sensitivity to miconazole and econazole. Contact Dermatitis 1995;32:370-1.
[Google Scholar]
|
| 16. |
Baes H. Contact sensitivity to miconazole with ortho-chloro cross-sensitivity to other imidazoles. Contact Dermatitis 1991;24:89-93.
[Google Scholar]
|
Fulltext Views
19,551
PDF downloads
3,605





![[Table - 1]](#tbl_ijdvl_2015_81_1_80_148592_t2.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2015_81_1_80_148592_f1.jpg){kind=link}