Translate this page into:
Alopecia areata - Vitiligo overlap syndrome: An emerging clinical variant
Correspondence Address:
A S Krishnaram
Professor and Head of the Department, Department of Dermatology, Madurai Medical College, Madurai, Tamil Nadu - 625020
India
| How to cite this article: Krishnaram A S, Saigal A, Adityan B. Alopecia areata - Vitiligo overlap syndrome: An emerging clinical variant. Indian J Dermatol Venereol Leprol 2013;79:535-537 |
Sir,
A 42-year-old male, agricultural labourer by occupation, presented with 2 months history of patchy hair loss over the scalp with associated whitish discoloration of the bald skin. Initially, he noticed two patches of hair loss over his scalp, which was gradually increasing in size and for which he took no treatment. A month later, depigmentation over the same areas of hair loss was noticed. There was no history of hair loss or whitish patches over any other area of the body in the past. The patient did not have any other comorbid condition. No family members were reported to have similar lesions. Skin examination revealed two irregular, well-defined, patchy areas of nonscarring alopecia: One over the frontoparietal area of size 11 × 6 cm [Figure - 1] and the other over the vertex of size 4 × 3 cm [Figure - 2] with associated depigmentation that was seen exactly over the alopecic area. Associated leucotrichia in few uninvolved hairs within the patch was noted. Skin and hair over other areas appeared normal. Clinical diagnosis of coexisting vitiligo and alopecia areata was made. The basic investigations such as complete blood count, blood sugar, renal function tests, liver function tests, and urine routine were all within normal limits. Thyroid function was also normal. Skin biopsy from frontoparietal lesion showed absence of melanin in the basal layer and perifollicular "swarm of bees" appearance in the same section, thereby, substantiating the clinical diagnosis [Figure - 3]. The patient was treated with topical 0.1% mometasone furoate cream, applied twice daily, for 1 month. Periodic examination at the end of 1 st , 3 rd , and 5 th month showed gradual perifollicular pigmentation and regrowth of hair and, finally, complete regrowth and pigmentation of even leucotrichic hairs [Figure - 1] and [Figure - 2].
 |
| Figure 1: (a) Co-localisation of alopecia areata and vitiligo over the frontoparietal area (11 × 6 cm), (b) Repigmentation and regrowth of hair at the end of 1st month, (c) More pigmentation and regrowth of hair at the end of 3rd month, (d) Completion of pigmentation and regrowth of hair at the end of 5th month |
 |
| Figure 2: (a) Co-localisation of alopecia areata and vitiligo over the vertex (4 × 3 cm), (b) Repigmentation and regrowth of hair at the end of 1st month, (c) More pigmentation and regrowth of hair at the end of 3rd month, (d) Completion of pigmentation and regrowth of hair at the end of 5th month |
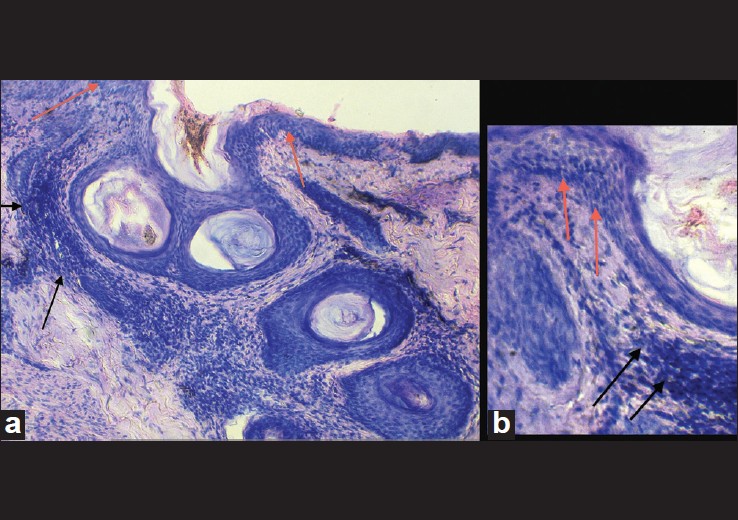 |
| Figure 3: (a) Biopsy showing structure of skin with absence of melanin in the basal layer (red arrow) and perifollicular "swarm of bees" appearance (black arrow) consistent with vitiligo and alopecia areata (H and E × 100), (b) High power (H and E × 400) showing absence of melanin (red arrow) and "swarm of bees" appearance (black arrow) |
Alopecia areata and vitiligo are common skin disorders that are known to coexist in an individual. [1]
However, strict anatomical colocalisation of vitiligo and alopecia areata has been very rarely reported in the literature, mostly in paediatric cases. [2],[3],[4],[5],[6],[7],[8] To the best of our knowledge, this is the first report of such colocalisation in an adult male.
Although the exact antigen is not known, it is widely accepted that alopecia areata and vitiligo are autoimmune diseases with cell-mediated immunity against hair follicle melanocytes, keratinocytes, and dermal papilla cells in case of alopecia areata and epidermal melanocytes in vitiligo. The association with other autoimmune diseases and the presence of circulating autoantibodies further support this hypothesis. This hypothesis also explains the sparing of white hairs in a patch of alopecia areata. [8] Genetic analysis studies have shown that class II human leukocyte antigen (HLA) and various other non-HLA genes are implicated in the pathogenesis of both these diseases. These genes have also been implicated in a number of other autoimmune diseases and are likely to function as general autoimmune susceptibility loci.
Alopecia areata and vitiligo have been found to be associated with various other autoimmune cutaneous disorders such as lichen planus, psoriasis, lupus erythematosus, and Sjogren syndrome, apart from systemic disorders such as pernicious anaemia, autoimmune hepatitis, thyroiditis, Addison′s disease, and inflammatory bowel disease. Thus, it may be proposed that both these disorders share a common autoimmune mechanism and genetic susceptibility. Apart from the colocalisation of alopecia and vitiligo seen in our case, both the conditions showed simultaneous improvement following treatment. It is speculated that this coexistence in a single anatomic area could be due to localized costimulation of an immunological mechanism mediated by helper T cells against both the melanocytes and the hair follicle antigens or by inactivation of non-specific suppressor mechanisms, leading to polyclonal B-cell activation and production of multiple autoantibodies. It has also been proposed that a structural similarity between circulating anti-endothelial antibody targeted against the endothelial cells of hair-bulb capillary plexus and antimelanocytic antibody can play a role. [2],[3],[4] Another interesting observation adding substance to this concept relates with pathogenesis behind the entity perinevoid alopecia, which also showed antibodies against melanocytes. [9]
The prevalence of alopecia areata and vitiligo in general population ranges from 0.1 to 3%, but there is a huge inconsistency regarding the prevalence of autoimmune diseases with alopecia areata. In few studies on vitiligo, a very high association rate of almost 12.5% was noted, whereas other studies reported association rate as low as 0.3%. [5],[6] To our knowledge, only 7 cases of colocalization have been reported so far in the world literature. [2],[3],[4],[5],[6],[7],[8]
Six out of 7 cases mentioned in the literature showed simultaneous onset of both the diseases unlike our case where alopecia appeared first followed by vitiligo 1 month later. This is the first case report showing appearance of vitiligo following alopecia areata.
We propose the entity "alopecia areata-vitiligo overlap syndrome" for this case and also for the cases reported in the past, as the clinical and immunopathological characteristics of both diseases occurred together with histological features of both diseases in the same specimen as in lupus erythematosus-lichen planus overlap syndrome. Although similar cases have been reported in the past, very few details are available regarding the follow-up and treatment aspect, except for two cases. Moreover, this entity may have a benign nature and better prognosis than that of alopecia areata and focal vitiligo occurring separately, because the cases reported by Yadav et al., [4] Ozcan et al., [8] as well as our case showed good response to topical therapy as highlighted by sequential follow-up pictures for 5 months. This entity also highlights the fact that even autoimmune diseases can have a regional presentation. Therefore, we propose that this emerging clinical variant may be included in the classification of either alopecia areata or vitiligo with more similar reports in the future.
| 1. |
Halder RM, Taliaferro SJ. Vitiligo. In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editors. Fitzpatick's Dermatology in general medicine. New York: McGraw Hill Company; 2008. p. 616-22.
[Google Scholar]
|
| 2. |
Dhar S, Kanwar AJ. Colocalization of vitiligo and alopecia areata. Pediatr Dermatol 1994;11:85-6.
[Google Scholar]
|
| 3. |
Adams BB, Lucky AW. Colocalization of alopecia areata and vitiligo. Pediatr Dermatol 1999;16:364-6.
[Google Scholar]
|
| 4. |
Yadav S, Dogra S, Kaur I. An unusual anatomical colocalization of alopecia areata and vitiligo in a child, and improvement during treatment with topical prostaglandin E2. Clin Exp Dermatol 2009;34:e1010-1.
[Google Scholar]
|
| 5. |
Ramot Y, Thomaidou E, Mali A, Zlotogorski A. An extraordinary colocalization of alopecia areata and vitiligo. Int J Trichology 2010;2:108-9.
[Google Scholar]
|
| 6. |
Rodriguez-Martin M, Merino N, Contreras P, Santana GG, Martin BR. Martin-Herrera A, et al. Anatomical colocalization of vitiligo and alopecia areata. Open Autoimmun J 2010;2:193-6.
[Google Scholar]
|
| 7. |
Cho HR, Lee MH. Colocalisation of segmental vitiligo and alopecia areata. Korean J Dermatol 2007;45:1115-7.
[Google Scholar]
|
| 8. |
Ozcan D, Cevlik Aydogan F. Concurrence of alopecia areata and vitiligo at the same anatomical site. Australas J Dermatol 2012;53:e61-3.
[Google Scholar]
|
| 9. |
Yesudian P, Thambiah AS. Perinevoid alopecia. An unusual variety of alopecia areata. Arch Dermatol 1976;112:1432-4.
[Google Scholar]
|
Fulltext Views
10,310
PDF downloads
2,058





![[Figure - 1]](#fig_ijdvl_2013_79_4_535_113100_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2013_79_4_535_113100_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2013_79_4_535_113100_f3.jpg){kind=link}