Translate this page into:
Amelanotic malignant melanoma with multiple secondaries
Correspondence Address:
Manas Chatterjee
(Derm and STD), Military Hospital, Jodhpur 342 006, Rajasthan
India
| How to cite this article: Chatterjee M. Amelanotic malignant melanoma with multiple secondaries. Indian J Dermatol Venereol Leprol 2006;72:252 |
Abstract
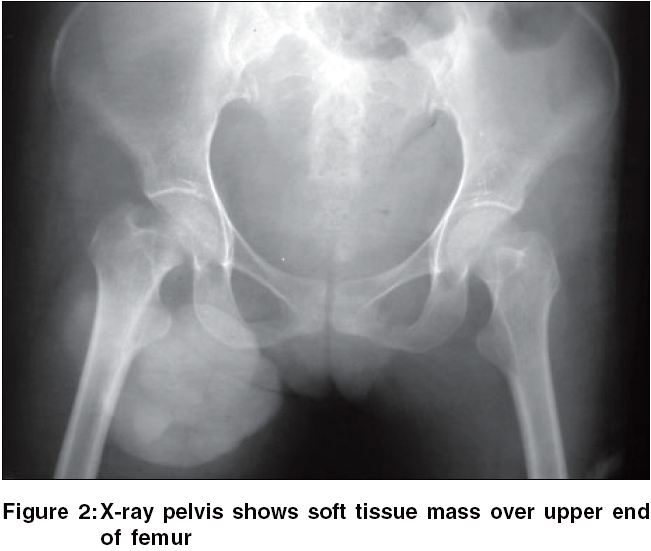
A 37-year-old female presented with a fungating cauliflower-like growth over the right inguinal region with fracture of the right distal femur. Clinical examination revealed an asthenic individual and showed a large fungating protuberant mass over right inguinal region and right knee. Investigations revealed pancytopenia, massive splenomegaly with right iliac lymphadenopathy on ultrasonography of abdomen and a soft tissue mass over upper end of femur and fracture of distal femur on radiological examination. CT scan showed multiple deposits in the lungs with splenomegaly and lymphadenopathy. Fine needle aspiration cytology showed poorly cohesive cellular aspirate with spindle and round cell population with no pigment. Biopsy showed replacement of the dermis by coalescent nests of malignant melanocytes. S-100 antigen was found to be positive. The patient was diagnosed as a case of amelanotic malignant melanoma in Stage III disease and treated with general measures, stabilization of the fracture site followed by oncological management.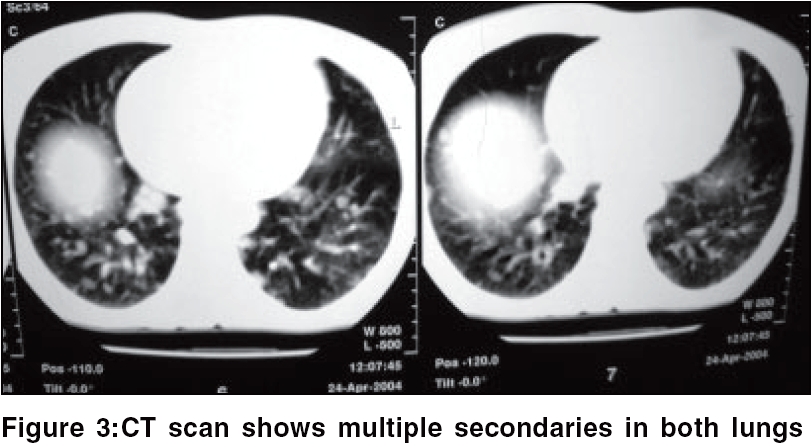 |
|
 |
|
 |
|
Amelanotic malignant melanoma (AMM) is a subtype of cutaneous malignant melanoma that has little or no pigment on visual inspection,[1] as a result of which it may masquerade as a variety of other benign and malignant skin conditions. This unusual variant of malignant melanoma represents 1.8 to 8.1% of all malignant melanomas[2] and leads to potential delays in diagnosis with eventual fatal outcome. Herein we report a case of AMM of the rarely involved inguinal region, who presented with Stage III disease along with distant metastasis.
Case Report
A 37-year-old female presented with a fungating cauliflower-like growth over the right inguinal region of 1-year duration with fracture of the right distal femur of 1-month duration. She also gave history of nonproductive cough along with breathlessness {New York Heart Association (NYHA) Class II}, intermittent low-grade fever and significant progressive loss of weight.
Clinical examination revealed an asthenic individual weighing 40 kg and showed a large fungating protuberant mass measuring 20 x 10 cm over right inguinal region and a 6 x 4 cm mass over right knee. The surface of the lesion showed multiple protuberant hemorrhagic nodules and bloody serosanguinous discharge along with faint speckled pigment at the periphery of the mass [Figure - 1].
Hemogram showed pancytopenia with raised lactate dehydrogenase of 2466 IU/L. Ultrasonography of abdomen showed massive splenomegaly with right iliac lymphadenopathy and radiological examination showed soft tissue mass over upper end of femur [Figure - 2] and fracture of distal femur indicating bone metastasis. CT scan showed multiple deposits in the lungs with splenomegaly and lymphadenopathy [Figure - 3]. Fine needle aspiration cytology from the mass showed poorly cohesive cellular aspirate with spindle and round cell population having abundant indistinct cytoplasm with no pigment and the nuclei were dark, large and eccentric at places.
Biopsy from the tumor showed replacement of the dermis by coalescent nests of malignant melanocytes. The cytoplasm was abundant, granular with no melanin pigment. Nuclei were large, vesicular and eosinophilic, with coarse chromatin. Mitotic figures were frequent, with nuclear grooves and folds in higher magnification. A variable inflammatory infiltrate was present in parts of the tumor along with evidence of junctional activity. S 100 antigen and DOPA reaction were found to be positive. The patient was diagnosed as a case of amelanotic malignant melanoma in Stage III disease. She was treated with general measures, stabilization of the fracture site followed by oncological management.
Discussion
Pizzicheta et al . in a recent review, evaluated the clinical and dermatoscopic features of AMM and tried to evaluate whether dermatoscopy was a useful technique for the diagnosis of AMM.[3] AMM usually occurs in sun-exposed skin of elderly patients with photo damage and appears as erythematous scaly macules or plaques with irregular borders simulating various skin lesions.[4] It may also present as translucent papules, thereby resembling basal cell carcinoma or keratoacanthoma. It may also be seen as an exophytic nodule, often eroded, simulating pyogenic granulomas or hemangiomas or as a skin-colored dermal plaque or nodule, as in our case.[5]
True AMM is rare, as some amount of pigment is often present at the periphery, as seen in our case. The clinical features routinely used to describe melanoma such as peripheral pigmentation, ulceration and asymmetry are not really helpful. Common clinical misdiagnosis of AMM include intradermal nevus, verruca vulgaris, basal cell carcinoma, seborrheic keratosis, dermatitis, actinic keratosis, Bowen′s disease, keratoacanthoma, dermatofibroma, pyogenic granulomas and hemangioma.[6] In AMM, clinical features do not allow the correct clinical diagnosis and therefore, dermoscopy has been found to be a useful noninvasive technique for diagnosing these skin lesions and improve the sensitivity of diagnosing AMM.[7] The dermatoscopic features that are usually noted are irregular pigmentation, dot globules, regression structures and a bluish white veil as well as vascular patterns such as milky red areas, linear irregular vessels or a combination of dotted and linear irregular vessels. These findings are not pathognomic but along with clinical findings, they do play a role in early diagnosis of AMM.[3] Newer imaging techniques like near infrared confocal scanning laser microscopy hold promise in early detection of AMM from normal surrounding skin.[8]
The prognosis of cutaneous AMM is determined by tumor thickness, location, patient age and sex - similar to its pigmented counterpart. Because of its lack of pigmentation, there is usually a delay in diagnoses as it is usually diagnosed at a more advanced stage when it has almost reached Clark stage IV/V with an average delay of about 13 months and a 5-year survival rate of 15% as compared to its pigmented counterpart.[9] The management of the lesions remains the same as malignant melanoma.
Thus, AMM is a rare variant of melanoma, which the physicians should be aware of so that early diagnosis and therapy can be achieved.
| 1. |
Andersen WK, Silvers DN. 'Melanoma? It can't be melanoma!' A subset of melanomas that defies clinical recognition. J Am Med Assoc 1991;266:3463-5.
[Google Scholar]
|
| 2. |
Koch SE, Lange JR. Amelanotic melanoma: the great masquerader. J Am Acad Dermatol 2000;42:731-4.
[Google Scholar]
|
| 3. |
Pizzichetta MA, Talamini R, Stanganelli I, Puddu P, Bono R, Argenziano G, et al . Amelanotic/hypomelanotic melanoma. Clinical and dermoscopic features. Br J Dermatol 2004;150:1117-24.
[Google Scholar]
|
| 4. |
Adler MJ, White CR Jr. Amelanotic malignant melanoma. Semin Cutan Med Surg 1997;16:122-30.
[Google Scholar]
|
| 5. |
Elmets CA, Ceilley RI. Amelanotic melanoma presenting as a pyogenic granulomas. Cutis 1980;25:164-6,168.
[Google Scholar]
|
| 6. |
Holder JE, Colloby PS, Fletcher A, Camp RD. Amelanotic superficial spreading malignant melanoma mimicking Bowen's disease. Br J Dermatol 1996;134:519-21.
[Google Scholar]
|
| 7. |
Bafounta ML, Beauchet A, Aegerter P, Saiag P. Is dermoscopy (epiluminescence microscopy) useful for the diagnoses of melanoma? Results of a meta-analysis using techniques adapted to the evaluation of diagnostic tests. Arch Dermatol 2001;137:1343-50.
[Google Scholar]
|
| 8. |
Busam KJ, Hester K, Charles C, Sachs DL, Antonescu CR, Gonzalez S, et al . Detection of clinically amelanotic malignant melanoma and assessment of its margins by in vivo confocal scanning laser microscopy. Arch Dermatol 2001;137:923-9.
[Google Scholar]
|
| 9. |
Ariel IM. Amelanotic melanomas. An analysis of 77 patients. Curr Surg 1981;38:151-5.
[Google Scholar]
|
Fulltext Views
2,688
PDF downloads
2,800





![[Figure - 1]](#fig_ijdvl_2006_72_3_252_25799_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2006_72_3_252_25799_2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2006_72_3_252_25799_3.jpg){kind=link}