Translate this page into:
An international multicenter study on quality of life and family quality of life in children with atopic dermatitis
2 Department of Dermatovenerology, Charles University, Prague, Czech Republic
3 Department of Psychological Medicine, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
4 Department of General Practice, Erasmus MC-University Medical Center, Rotterdam, The Netherlands
5 Department of Women's and Children's Health, State University of Montes Claros, Montes Claros, Brazil
6 Department of Dermatology, State University of Montes Claros, Montes Claros, Brazil
7 Department of Dermatology, College of Medicine, Hallym University, Seoul, Korea
Correspondence Address:
Pavel V Chernyshov
Department of Dermatology and Venereology, National Medical University, 13, Bulvar Shevchenko, 01601, Kiev
Ukraine
| How to cite this article: Chernyshov PV, Jirakova A, Ho RC, Moed H, Caldeira AP, Alvarenga TM, Park CW, Hercogova J. An international multicenter study on quality of life and family quality of life in children with atopic dermatitis. Indian J Dermatol Venereol Leprol 2013;79:52-58 |
Abstract
Background: Atopic dermatitis (AD) has severe impact on the quality of life (QoL) of children suffering from the disease and their families. The infant's dermatitis quality of life index (IDQoL) and the dermatitis family impact questionnaire (DFI) were designed to study this impact. Aims: To compare the impact of AD on children and their families in different countries. Methods: 419 children with AD from six countries representing three continents under the age of 4 years were included into the study. English, Ukrainian, Czech, Portuguese, and Korean versions of the IDQoL and the DFI and Dutch version of the IDQoL questionnaires were used. Results: The highest scored items for the IDQoL and the DFI were rather similar. The IDQoL and the DFI results were well correlated with parental assessment of disease severity and between each other in all countries. Some differences mostly in the IDQoL assessment were found. Conclusion: Despite some reported peculiarities, parents in different counties assessed QoL and family QoL of their AD children in a similar way. The IDQoL and the DFI may be reliable initial measures for international studies. International study on the influence of the same treatment methods on the IDQoL and the DFI assessments is important.Introduction
Atopic dermatitis (AD) is a common chronic inflammatory skin condition that often begins in infancy or early childhood, with 90% of cases appearing in the first 5 years of life. [1],[2] Prevalence of AD in different regions may vary. Thus, reported prevalence of AD in preschool children in UK is 21.0%, meanwhile in China only 3.07%. [3],[4] Severe negative impact of AD on the quality of life (QoL) of children and their families was well documented in previous studies. [5],[6],[7],[8]
Questionnaire is the most common method to measure QoL. In small children, outsider or proxy-ratings (questions posed to persons close to the patient or to a patient′s therapist, if the patient cannot give information by him/herself) can be used. Parent proxy-report should only be the primary outcome measure when the child is too young or ill or otherwise unable to self-report. [9]
The infant′s dermatitis quality of life index (IDQoL) questionnaire was designed 10 years ago for use in children with AD below the age of 4 years. It is self-explanatory and should be completed by the child′s parents or regular carer. The higher the score the more the QoL is impaired. The severity of eczema is scored separately by the child′s parents or regular carer. [10]
Following interviews of families in which one child had AD, the dermatitis family impact (DFI) questionnaire was described covering "secondary" effect of skin disease. [11]
QoL questionnaires are increasingly being used by clinicians and researches as outcome measures for assessing the impact of AD. Moreover, their use in conjunction with clinical measures in clinical trials has been recommended by the National Institute for Health and Clinical Excellence (UK). [12]
The IDQoL and the DFI were translated into different languages and several national versions of these questionnaires are available. [13],[14],[15],[16],[17] However, few authors provided exact numeric data on IDQoL and DFI items assessment in their articles and therefore it is difficult to understand how much the results of different studies vary.
Results of a comparative study on QoL of AD children from Ukraine and Czech Republic showed minimal differences in the IDQoL results. [18]
The aims of our study were first to make a comparison of the assessment of the impact of AD on young children and their families in different countries and continents and second, to investigate the reliability of the IDQoL and the DFI questionnaires as initial measure for international multicenter studies.
Methods
Study population
The authors who published a study on the IDQoL and the DFI assessments in children with AD were found by means of PubMed and contacted to obtain the data set. Data on 419 children with AD from six countries (Ukraine, Czech Republic, Singapore, the Netherlands, Brazil, and South Korea) representing three continents from 0 to 4 years old who had no other manifest diseases were used for the study. The diagnosis of AD was made using Hanifin and Rajka or Williams′ criteria. [19],[20] Patients from South Korea, Brazil, Singapore, and the Netherlands were selected from participants of local studies. [14],[17],[21],[22] Children who had diagnosed AD and were less than 4 years old at the moment of completing the questionnaires by their parents were selected for the study. Part of patients from Ukraine and Czech Republic participated in comparative study on the IDQoL. [18] All patients visited dermatologists except those from the Netherlands who visited the general practitioner. Ethical permission for the study was granted by the local ethic research committees.
QoL assessment
Original (English), Ukrainian, Czech, Portuguese, and Korean versions of the IDQoL and the DFI questionnaires and a Dutch version of the IDQoL questionnaire were used. Permission to use the IDQoL and the DFI questionnaires were granted by its authors and copyright owners, Professor Andrew Y. Finlay and Dr. M.S. Lewis-Jones.
The IDQoL consists of 10 questions scored 0-3. The IDQoL is calculated by summing the score of each question resulting in a maximum of 30 and a minimum of 0. The IDQoL also contains a single initial question on parental assessment of global clinical severity which is scored separately from the QoL, graded 0-4, from none to extremely severe. [10] The DFI also consists of 10 questions scored 0-3 and a maximum score of 30. [11] The higher the score the more the QoL is impaired in both questionnaires.
In most cases, the parent who filled in the questionnaires was mother. However, it was previously shown that gender of parent who should fill in the IDQoL [23],[24] and the DFI [24] cannot significantly influence the results of clinical studies.
Statistical analysis
Values are expressed as mean±standard deviation (SD). Tukey-Kramer Multiple Comparisons Test, Kruskal-Wallis Test (Nonparametric ANOVA), and Spearman nonparametric correlation were used. The results were considered significant if P<0.05.
Demographic and economical parameters
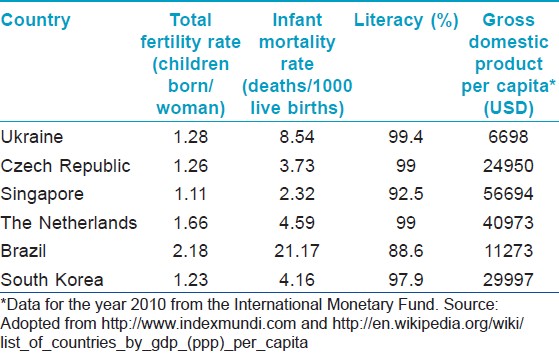
To check demographic and economical inequivalence between countries, total fertility rate, infant mortality rate, literacy rate, and gross domestic product per capita in all participated countries were checked by means of internet resources (http://www.indexmundi.com and data for the year 2010 from the International Monetary Fund; http://en.wikipedia.org/wiki/List_of_countries_by_GDP_(PPP)_per_capita).
Results
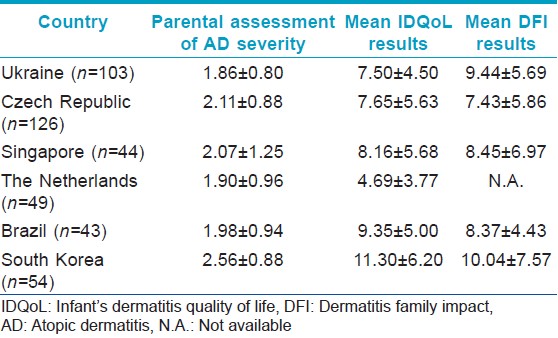
Mean IDQoL, DFI, and parental assessment of disease severity scores are presented in [Table - 1]. Korean parents assessed severity of AD in their children significantly higher than Ukrainian, Dutch, Czech, and Brazilian (P<0.05). Mean IDQoL results in children from Korea were higher than in patients from Ukraine, Czech Republic, and Singapore (P<0.05). In contrast, Dutch children had lower mean IDQoL than Ukrainian, Czech, Singapore, Brazilian, and Korean (P<0.05).
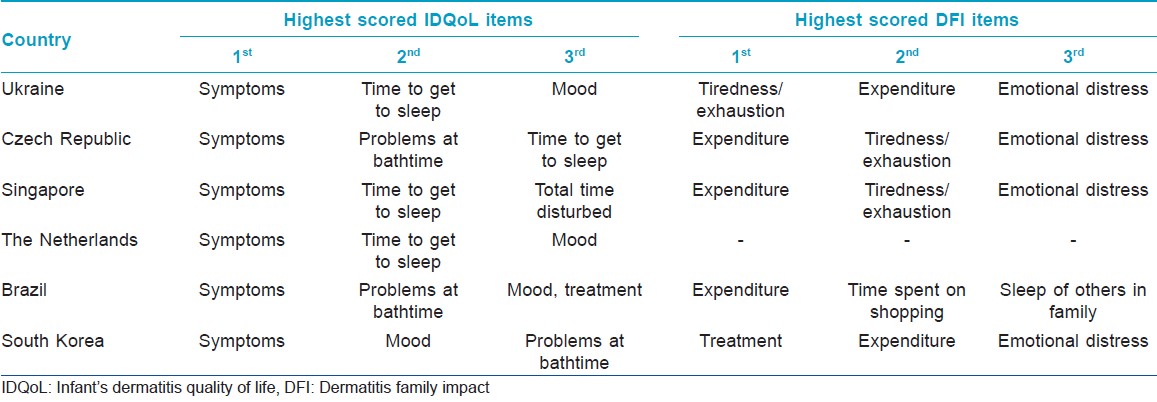
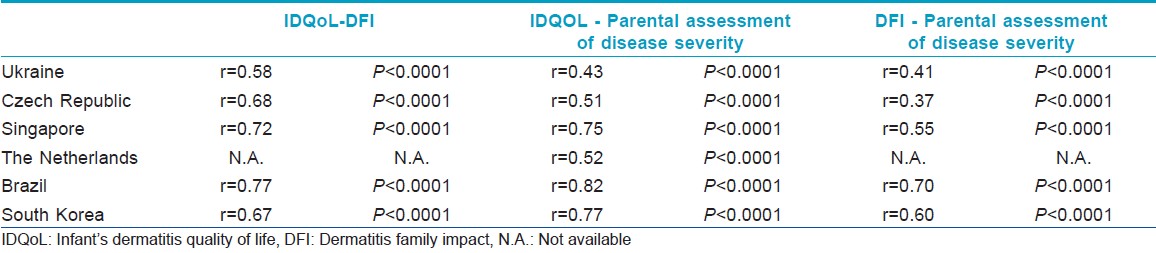
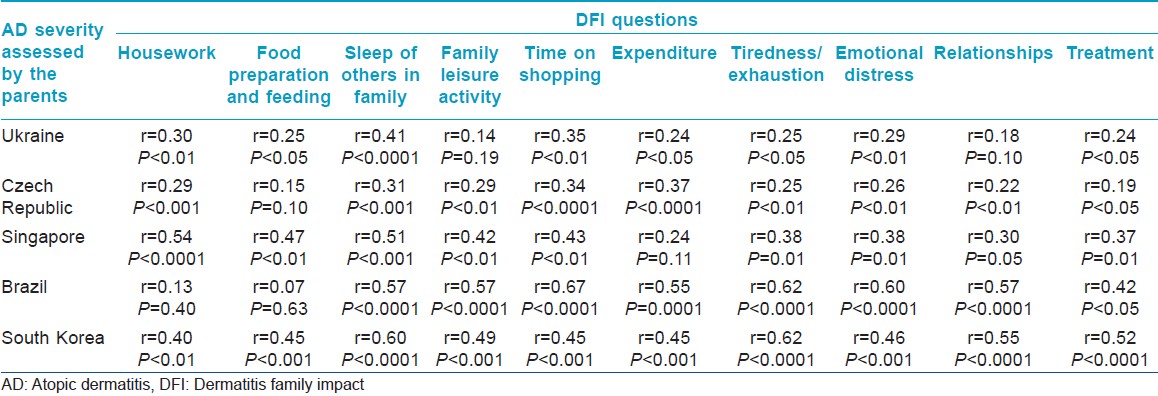
The items with highest score for the IDQoL and the DFI were rather similar for all countries [Table - 2]. The IDQoL and the DFI results were well correlated with parental assessment of disease severity and between each other in all countries [Table - 3]. The DFI results did not correlate with patients′ age. Meanwhile, only in Ukrainians parental assessment of disease severity and the IDQoL negatively correlated with the age of children with AD (r=-0.27, P<0.01 and r=-0.23, P<0.05, respectively).
Some differences in 8 of 10 separate IDQoL items were found. Thus, symptoms were assessed less severe in Ukrainians in comparison with Koreans (1.22±0.78 and 1.67±0.97, P<0.05). Mood changes were higher in Brazilian and Korean children than in Dutch children (0.51±0.65, 1.07±0.70, and 1.02±0.90, respectively, P<0.05). Impact of AD on playing and swimming was less severe for Dutch than for Czech and Brazilians (0.29±0.58, 0.79±0.96, and 0.84±0.65, respectively, P<0.01). Items concerning impact on family activity and mealtimes were also assessed significantly lower by Dutch parents than by Ukrainian, Czech, Brazilian, and Korean parents (0.29±0.58, 1.03±0.88, 0.73±0.88, 0.72±0.70, and 0.55±0.72 for family activity and 0.12±0.33, 0.75±0.77, 0.56±0.81, 0.84±0.65, and 0.74±0.76 for mealtimes, respectively, P<0.05). Brazilian children had significantly higher impact of their treatment on QoL than Ukrainians, Czech, Singapore, and Dutch children (1.07±0.67, 0.64±0.70, 0.38±0.68, 0.39±0.69, and 0.31±0.51, respectively, P<0.01). Problems with dressing had higher impact on Brazilians than on Ukrainians, Singaporeans, and Dutch (1.02±0.80, 0.61±0.75, 0.18±0.39, and 0.39±0.67, respectively, P<0.01). Meanwhile, Singaporeans had less concern on dressing than Ukrainian and Czech children (0.18±0.39, 0.61±0.75, and 0.81±0.93, respectively, P<0.05) and Dutch less concern than Czech (0.39±0.67 and 0.81±0.93, P<0.05). Problems at bathtime had more severe impact on Brazilians than on Ukrainians, Singaporeans, and Dutch (1.02±0.80, 0.63±0.77, 0.45±0.76, and 0.49±0.68, respectively, P<0.01).
Mean DFI results did not differ significantly in patients from different countries. Some differences were found only in four separate DFI items. Ukrainians and Koreans had higher impact on family food preparation and feeding than Czech and Brazilian families (1.09±0.89 and 1.15±0.95 versus 0.71±0.84 and 0.42±0.70, respectively, P<0.05) and higher impact on housework than Czech families (0.85±0.88, 1.02±0.91, and 0.47±0.76, respectively, P<0.01). Brazilians had more time to spend on shopping than Ukrainians, Czech, Singapore, and Koreans (1.23±0.61, 0.62±0.81, 0.46±0.75, 0.55±0.85, and 0.55±0.72, respectively, P<0.01). Meanwhile, Korean parents had more problems with child′s treatment than Ukrainian, Czech, Singaporean, and Brazilian (1.44±0.92, 1.03±0.88, 0.73±0.88, 0.82±0.92, and 0.72±0.70, respectively, P<0.05).
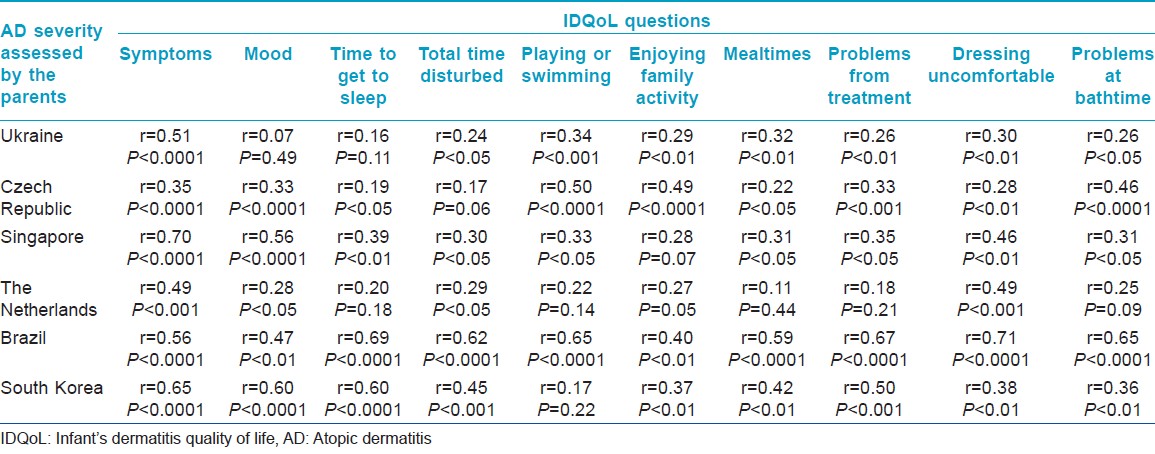
Separate IDQoL and DFI items were well correlated with parental assessment of disease severity in almost all cases [Table - 4] and [Table - 5]. However, only in Ukrainians, four IDQoL items negatively and one item positively correlated with the age of patients ("symptoms" r=-0.21, P<0.05; "mood" r=0.21, P<0.05; "time to get to sleep" r=-0.22, P<0.05; "total time disturbed" r=-0.45, P<0.001; "dressing uncomfortable" r=-0.31, P<0.01) and IDQoL item on symptoms correlated with the age in Czech and Dutch children (r=0.30 and r=0.42, P<0.01, respectively). Only one separate DFI item in Ukrainian parents ("sleep of others in family" r=-0.26, P<0.05) and two DFI items in Korean parents ("food preparation and feeding" r=- 0.30, P<0.05 and "helping with treatment" r=-0.28, P<0.05) significantly correlated with the age of their children with AD.
Discussion
Our results showed common tendencies in the assessment of QoL and family QoL in nonrandomized AD children from different countries. High level of correlation between parental assessment of disease severity with the IDQoL and the DFI confirms common tendencies in the assessment of QoL and family QoL by parents of AD children from different countries despite cultural, climatic, and economic peculiarities. Authors of previously published studies on the IDQoL and the DFI were eager to show only the three highest scored items of the questionnaires. [13],[15],[17] The value of this approach is controversial because the difference between highest scored items and subsequent highly scored items may often be insignificant. However, three highest scored items of the IDQoL and the DFI in counties we studied were quite common. Despite rather low impact of AD on expenditures in UK study, [11] our study demonstrated high impact of this DFI item for all studied countries. We studied economical parameters in participating countries and did not find any difference in the assessment of the economical impact of AD on families from countries with different economical situations. Meanwhile, Camfferman et al.[25] recently reported that low socioeconomic status is associated with a higher frequency of disturbed sleep due to eczema in children. In our study, Brazilian families were from one of the poorest regions of the country and only they reported sleep of others in the family as one of the top scored items.
We also checked total fertility rate, infant mortality rate, and literacy in all participated countries [Table - 6]. It seems that only combination of higher fertility rate with high infant mortality rate may play some role in the attitude of Brazilians parents to their own QoL and QoL of their children. They did not assess emotional distress as top scored DFI item but reported high impact of AD on time spends on shopping, on the mood of their children and high impact of AD treatment on their children.
AD had sufficient impact on child′s mood in all studied countries. According to Ricci et al.,[15] parents perceive their child′s mood with great sensitivity and attention and are able to sense small alterations and changes in his mood and everyday activities. However, feelings of exhaustion and depression in parents can sometimes alter this perception and lead to a slight overrating in their assessment. Meanwhile in our study, Brazilian and Korean parents who reported highest impact of AD on their child′s mood did not assess emotional distress or tiredness and exhaustion higher than others.
Emotional distress was reported as a serious problem for all parents except Brazilian. Moderate to severe childhood eczema should be regarded as a significant illness in which maternal stress is equivalent to that associated with the care of children with severe developmental and physical problems. [26] Despite the fact that parenting distress is associated with severe atopic eczema in early childhood, Daud and colleagues [27] reported that atopic eczema does not lead to insecurity of the mother-child attachment. However, our results indicate the necessity of inclusion of measures focused on a decrease of parental distress caused by AD in their child into all educational activities for this group of patients and their families.
Significant correlation of itch and sleeplessness is well documented in large studies. [28] However, only Brazilians assessed sleeplessness of the parents higher than tiredness and exhaustion or emotional distress. Therefore, it is possible to consider that parental exhaustion and emotional distress are more complicated problems than simple consequences of sleeplessness.
The fact that impact of AD on relation in the family was not a highly assessed item in our study is optimistic because it was previously reported that divorce/separation is associated with a significantly increased incidence of AD in children. [29] Meanwhile, in all countries except Ukraine, impact of AD on relation in the family was higher in children with higher parental assessment of disease severity.
Parent-caregiver′s assessment of severity of AD was previously found to be the single strongest predictor of family impact. [30] In our study, Korean parents assessed disease severity of their children highly. However, Korean parents had more problems with child′s treatment only. Korea has its unique culture and parents of AD children usually depend on other sources of medical care such as oriental medicine or herbal medicine for their children′s treatment. Therefore, they spend extra money for lots of medications which are not evidence based. This tendency may affect parents and increase the impact of AD. Meanwhile, negative correlation of this DFI item with age in Korean parents suggests that this is mostly a problem of initial relapses of AD and deficit of experience in parents.
Lower IDQoL results in Dutch patients may be partially explained by absence of severe cases of AD in this group. Recommendations of the general practitioner that treated Dutch patients contain less limitations and restrictions and may also be the reason of better QoL assessment results.
Patients from Singapore have low impact of AD on their dressing. Singapore is near to equator and there is no winter there. Hence, children wear minimal clothes at home and this may result low assessment of this IDQoL item. Despite the fact that Brazil is also located near equator, Brazilians assessed the impact of AD on their child′s dressing much higher. However, they did not use any special clothes. This peculiarity may be addressed to intercultural differences.
Problems at bathtime and impact of AD treatment in Brazilians may be considered as other intercultural differences. Most of Brazilians reported two baths a day and no problems with water quality or costs. Despite the absence of severe cases of AD in studied patients from Brazil, their parents consider high impact of treatment on children′s QoL. Brazilians spend more time for shopping may be attributed to objective factors.
Another intercultural difference is that Ukrainian parents begin to consider clinical manifestations of their children AD less severe and Czech and Dutch parents more severe with age of children. According to literature data, AD may resolve completely in half of the children by the age of two, but in others persists in a mild form or periodically recurs. [31] Thus, Ukrainian parents assess their child′s symptoms with higher objectivism. Meanwhile, Czech and Dutch parents consider condition more severe in older group of children. The reason for that can be hidden in more serious self-consciousness and stress connected with psychological and physical limitations caused by AD in older children.
We have shown some difference in QoL and family QoL assessments caused by cultural peculiarities in different countries. However, these differences concern few separate items of the DFI and IDQoL questionnaires. Correlations between both questionnaires and parental assessment of disease severity were common in all countries. Thus, our results showed that parents in different countries assessed QoL and family QoL of their children with AD in similar way. It makes possible to recommend the IDQoL and the DFI questionnaires for international studies as reliable initial measure tool to assess impact and efficacy of treatment. The next important step to confirm this statement should be an international study on the influence of same treatment methods on the IDQoL and DFI results.
Acknowledgments
We thank Professor A.Y. Finlay and Dr. M.S. Lewis-Jones for the permission to use the IDQoL and the DFI questionnaires.
| 1. |
Peroni DG, Piacentini GL, Bodini A, Rigotti E, Pigozzi R, Boner AL. Prevalence and risk factors for atopic dermatitis in preschool children. Br J Dermatol 2008;158:539-43.
[Google Scholar]
|
| 2. |
Abramovits W. Atopic dermatitis. J Am Acad Dermatol 2005;53:S86-93.
[Google Scholar]
|
| 3. |
Wadonda-Kabondo N, Sterne JA, Golding J, Kennedy CT, Archer CB, Dunnill MG, et al. A prospective study of the prevalence and incidence of atopic dermatitis in children aged 0-42 months. Br J Dermatol 2003;149:1023-8.
[Google Scholar]
|
| 4. |
Gu H, You LP, Liu YS, Yan Y, Chen K. Survey on the prevalence of childhood atopic dermatitis in ten cities of China. Chin J Dermatol 2004;37:29-31.
[Google Scholar]
|
| 5. |
Beattie PE, Lewis-Jones MS. A comparative study of impairment of quality of life in children with skin disease and children with other chronic childhood diseases. Br J Dermatol 2006;155:145-51.
[Google Scholar]
|
| 6. |
Moore K, David TJ, Murray CS, Child F, Arkwright PD. Effect of childhood eczema and asthma on parental sleep and well-being: a prospective comparative study. Br J Dermatol 2006;154:514-8.
[Google Scholar]
|
| 7. |
Su JC, Kemp AS, Varigos GA, Nolan TM. Atopic eczema: its impact on the family and financial cost. Arch Dis Child 1997;76:159-62.
[Google Scholar]
|
| 8. |
Chamlin SL, Chren MM. Quality-of-life outcomes and measurement in childhood atopic dermatitis. Immunol Allergy Clin North Am 2010;30:281-8.
[Google Scholar]
|
| 9. |
Varni JW, Limbers CA, Burwinkle TM. Parent proxy-report of their children's health-related quality of life: an analysis of 13,878 parents' reliability and validity across age subgroups using the PedsQL 4.0 Generic Core Scales. Health Qual Life Outcomes 2007;5:2.
[Google Scholar]
|
| 10. |
Lewis-Jones MS, Finlay AY, Dykes PJ. The infants' dermatitis quality of life index. Br J Dermatol 2001;144:104-10.
[Google Scholar]
|
| 11. |
Lawson V, Lewis-Jones MS, Finlay AY, Reid P, Owens RG. The family impact of childhood atopic dermatitis: the Dermatitis Family Impact Questionnaire. Br J Dermatol 1998;138:107-13.
[Google Scholar]
|
| 12. |
Beattie PE, Lewis-Jones MS. An audit of the impact of a consultation with a paediatric dermatology team on quality of life in infants with atopic eczema and their families: further validation of the Infants' Dermatitis Quality of Life Index and Dermatitis Family Impact score. Br J Dermatol 2006;155:1249-55.
[Google Scholar]
|
| 13. |
Gånemo A, Svensson A, Lindberg M, Wahlgren CF. Quality of life in Swedish children with eczema. Acta Derm Venereol 2007;87:345-9.
[Google Scholar]
|
| 14. |
Park CK, Park CW, Lee CH. Quality of life and the family impact of atopic dermatitis in children. Korean J Dermatol 2007;45:429-38.
[Google Scholar]
|
| 15. |
Ricci G, Bendandi B, Bellini F, Patrizi A, Masi M. Atopic dermatitis: quality of life of young Italian children and their families and correlation with severity score. Pediatr Allergy Immunol 2007;18:245-9.
[Google Scholar]
|
| 16. |
Chernyshov PV. Creation and cross-cultural adaptation of Ukrainian versions of questionnaires for assessment of quality of life of children with atopic dermatitis and their families. Lik Sprava 2008;1-2:124-8.
[Google Scholar]
|
| 17. |
Alvarenga TM, Caldeira AP. Quality of life in pediatric patients with atopic dermatitis. J Pediatr (Rio J) 2009;85:415-20.
[Google Scholar]
|
| 18. |
Chernyshov PV, Jiráková A, Hercogová J. Comparative study of the quality of life of children with atopic dermatitis from Ukraine and the Czech Republic. J Eur Acad Dermatol Venereol 2011;25:1483-4.
[Google Scholar]
|
| 19. |
Hanifin GM, Rajka G. Diagnostic feature of atopic dermatitis. Acta Derm Venereol 1980;92:44-7.
[Google Scholar]
|
| 20. |
Williams HC, Burney PG, Pembroke AC, Hay RJ. The U.K. Working Party's Diagnostic Criteria for Atopic Dermatitis. III. Independent hospital validation. Br J Dermatol 1994;131:406-16.
[Google Scholar]
|
| 21. |
Ho RC, Giam YC, Ng TP, Mak A, Goh D, Zhang MW, et al. The influence of childhood atopic dermatitis on health of mothers, and its impact on Asian families. Pediatr Allergy Immunol 2010;21:501-7.
[Google Scholar]
|
| 22. |
van Valburg RW, Willemsen MG, Dirven-Meijer PC, Oranje AP, van der Wouden JC, Moed H. Quality of life measurement and its relationship to disease severity in children with atopic dermatitis in general practice. Acta Derm Venereol 2011;91:147-51.
[Google Scholar]
|
| 23. |
Holm EA, Esmann S, Jemec GB. Parent gender and assessment of infant life quality. J Eur Acad Dermatol Venereol 2006;20:274-6.
[Google Scholar]
|
| 24. |
Chernyshov PV. May the gender of a parent influence assessment of health-related quality of life, family impact and severity of atopic dermatitis in children? Pediatr Dermatol 2009;26:99-100.
[Google Scholar]
|
| 25. |
Camfferman D, Kennedy JD, Gold M, Martin AJ, Winwood P, Lushington K. Eczema, sleep, and behavior in children. J Clin Sleep Med 2010;6:581-8.
[Google Scholar]
|
| 26. |
Faught J, Bierl C, Barton B, Kemp A. Stress in mothers of young children with eczema. Arch Dis Child 2007;92:683-6.
[Google Scholar]
|
| 27. |
Daud LR, Garralda ME, David TJ. Psychosocial adjustment in preschool children with atopic eczema. Arch Dis Child 1993;69:670-6.
[Google Scholar]
|
| 28. |
Weisshaar E, Diepgen TL, Bruckner T, Fartasch M, Kupfer J, Lob-Corzilius T, et al. Itch intensity evaluated in the German Atopic Dermatitis Intervention Study (GADIS): correlations with quality of life, coping behaviour and SCORAD severity in 823 children. Acta Derm Venereol 2008;88:234-9.
[Google Scholar]
|
| 29. |
Bockelbrink A, Heinrich J, Schäfer I, Zutavern A, Borte M, Herbarth O, et al. Atopic eczema in children: another harmful sequel of divorce. Allergy 2006;61:1397-402.
[Google Scholar]
|
| 30. |
Balkrishnan R, Housman TS, Carroll C, Feldman SR, Fleischer AB. Disease severity and associated family impact in childhood atopic dermatitis. Arch Dis Child 2003;88:423-7.
[Google Scholar]
|
| 31. |
Meadow R, Newell S. Skin.. In: Meadow R, Newell S, editors. Lecture Notes of Paediatrics. 7 th ed. Oxford: Blackwell-Science; 2002. p. 181-7.
[Google Scholar]
|
Fulltext Views
4,105
PDF downloads
1,945





![[Table - 1]](#tbl_ijdvl_2013_79_1_52_104669_t1.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2013_79_1_52_104669_t2.jpg){kind=link}
![[Table - 3]](#tbl_ijdvl_2013_79_1_52_104669_t3.jpg){kind=link}
![[Table - 4]](#tbl_ijdvl_2013_79_1_52_104669_t4.jpg){kind=link}
![[Table - 5]](#tbl_ijdvl_2013_79_1_52_104669_t5.jpg){kind=link}
![[Table - 6]](#tbl_ijdvl_2013_79_1_52_104669_t6.jpg){kind=link}