
Translate this page into:
An ulcerated plaque on the palm
Corresponding author: Dr. Jingru Sun, Department of Dermatology and Venereology, Peking University First Hospital, Xicheng District, Beijing, China. sjr12315@126.com
-
Received: ,
Accepted: ,
How to cite this article: Wang S, Sun J. An ulcerated plaque on the palm. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_1158_2024
An otherwise healthy Chinese woman in her 60s visited the dermatology department with a painful ulcerated lesion on her left palm. The lesion had started as a papule one year ago, gradually enlarging and ulcerating in the recent months with no response to topical antibiotics. She denied any history of trauma, radiation, burns, or exposure to harmful chemicals in the affected area. She was a white-collar worker. There was no family history of skin cancers, and she had no other similar skin lesions or jaw cysts. Physical examination revealed a 1 cm-sized pink plaque with central crusting and raised edges. [Figure 1a] Dermoscopic examination showed blue ovoid nests with arborising vessels [Figure 1b].

- An ulcerated plaque with central crusting on the palm.

- Dermoscopy showing blue ovoid nests and arborising vessels (DL4, polarising: 20×).
A skin biopsy from the lesion revealed multiple nests of basaloid cells originating from the epidermis and infiltrating into the dermis [Figure 2a]. The basaloid cells displayed a palisading arrangement at the periphery with the presence of stromal mucin and clefts between the cell aggregations [Figure 2b]. Immunohistochemistry confirmed positive BerEp4 staining of the basaloid cells [Figure 2c].
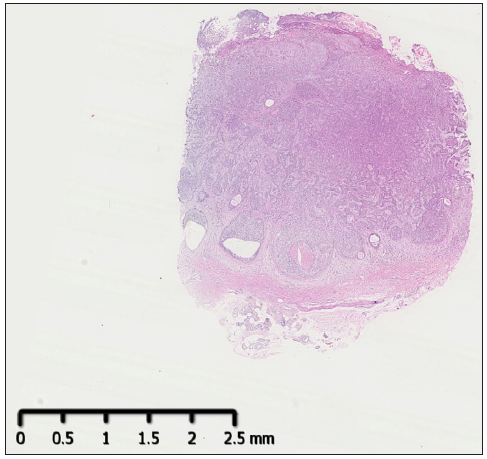
- Multiple nests of basaloid cells originating from the epidermis and infiltrating into the dermis (Haematoxylin and eosin; 10×).
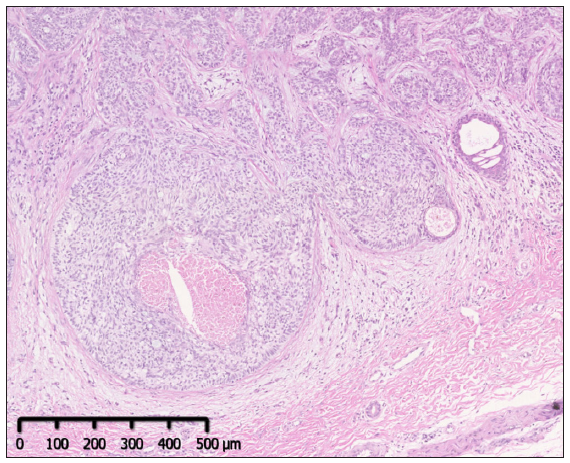
- The basaloid cells at the periphery of aggregations were arranged in a palisade pattern (Haematoxylin and eosin; 50×).
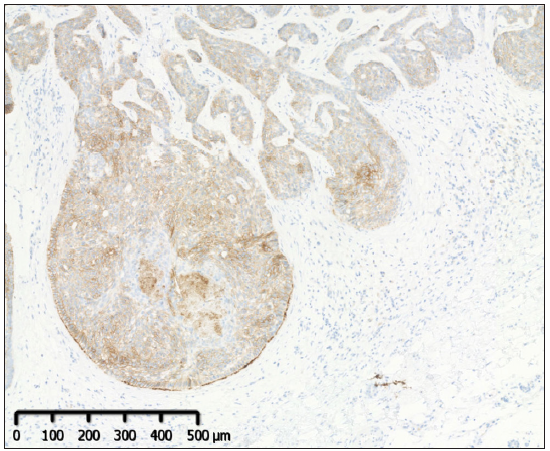
- Positive BerEP4 staining of the tumour (Immunohistochemistry staining; 50×).
The patient underwent Mohs micrographic surgery and has been recurrence free for over a year.
Basal cell carcinoma is among the most prevalent malignancies worldwide. Individuals with fair skin are at a higher risk, with an estimated lifetime risk of approximately 30%, primarily related to prolonged exposure to ultraviolet radiation.1 About 80% of BCCs develop in sun-exposed areas, predominantly on the head and neck, while around 15% are found on the trunk.2 However, BCC occurrences on the palms or soles are extremely rare.
The first documented case of palmar BCC was in the 1960s.2 Since then, less than 20 cases of isolated palmar BCC have been reported.2-4 In some of these cases, there was an association with basal cell naevus syndrome, or trauma, scarring, radiation, or arsenic exposure.2-4 Cases like ours, without identifiable aetiological factors, remain exceptionally rare. Traditionally, BCC is believed to originate from epidermal stem cells in the hair follicle bulge or undifferentiated cells in the outer root sheath, explaining why BCC typically does not appear on the palms or soles, which lack hair follicles. It is proposed that BCC on the hairless skin may originate from interfollicular epidermal stem cells or progenitor cells of the eccrine glands.5
Basal cell carcinoma of the acral skin, such as the palms, typically manifests as slow-growing plaques, sometimes accompanied by ulceration. Important differential diagnoses include squamous cell carcinoma (SCC), pyogenic granuloma, and poroma. Dermoscopy plays a vital role in BCC diagnosis, often revealing distinctive features like ovoid nests, globules, leaf-like areas, and arborising vessels. Histologically, palmar BCC shares similarities with BCCs found in other locations, displaying dermal nests of basaloid keratinocytes, peripheral palisading, and a mucin-rich stroma. Specifically, BCC on the palms or soles shows a thickened stratum corneum and the absence of hair follicles on histology. Immunohistochemical staining with BerEP4 helps distinguish BCC from SCC and poroma in cases of doubt.
Although metastasis is rare, BCC can result in significant local tissue destruction, underscoring the importance of prompt diagnosis and appropriate treatment. Various therapeutic options are available, including surgery, radiotherapy, photodynamic therapy, and systemic sonic Hedgehog inhibitors. However, surgery continues to be the preferred choice for most BCC cases due to its high efficacy and low recurrence rate.1
Our case emphasises the significance of considering the rare condition of acral BCC when examining a solitary ulcerated plaque on the palms or soles.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
This work was supported by the National Natural Science Foundation of China (82002903, J.S.).
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
References
- Update in the management of basal cell carcinoma. Acta Derm Venereol. 2020;100:adv00140.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- A palmar injury that failed to heal. Diagnosis: Basal cell carcinoma of the palm. Clin Exp Dermatol. 2006;31:731-32.
- [CrossRef] [PubMed] [Google Scholar]
- Collision tumor of basal and squamous cell carcinoma of the palm. J Clin Aesthet Dermatol. 2019;12:28-30.
- [PubMed] [Google Scholar]
- Basal cell carcinoma of the palm: An unusual presentation of a common tumour. Australas J Dermatol. 2020;61:69-70.
- [PubMed] [Google Scholar]
- Identification of the cell lineage at the origin of basal cell carcinoma. Nat Cell Biol. 2010;12:299-305.
- [CrossRef] [PubMed] [Google Scholar]




