Translate this page into:
Angel's kiss in three generations
2 Department of Radiology, Haydarpasa Numune Training and Research Hospital, Istanbul, Turkey
Correspondence Address:
Zafer Turkoglu
Altunizade mah Atifbey sok. Sermiha Konutlari sitesi 63/2 C-16, Acibadem 34662 Uskudar/Istanbul
Turkey
| How to cite this article: Turkoglu Z, Can B, Kavala M, Turkoglu O. Angel's kiss in three generations. Indian J Dermatol Venereol Leprol 2010;76:592 |
Sir,
Vascular stains are the most common capillary malformations (CMs) encountered in newborns. Similar stains called ′′salmon patch,′′ ′′angel′s kiss,′′ ′′stork bite′′ occur in up to 40-50% of newborns but fade progressively during infancy and so termed as ′′fading macular stains.′′ Angel′s kiss (AK) represents a subset of CMs that occupies a midline location of the glabellar region. Some macular stains particularly those on the nape of neck (stork bite) and rarely on the glabellar region (angel′s kiss) persist into adulthood without significant darkening and then called as medial telangiectatic nevus. Despite the high frequency CMs in the general population, only few families that show familial segregation of CMs as an autosomal dominant trait have been reported. [1],[2],[3],[4] We describe three generations including daughter, mother and grandmother with persisting AK located on the glabellar region. A 22-year-old girl (proband) presented with a vascular lesion on her forehead. She reported that she had this red discoloration without any change in color and size since birth. There was 3Χ5 cm reddish butterfly shaped macule on the central part of her forehead and glabella [Figure - 1]a. When questioned, the patient reported that in her family her mother and grandmother also had pinkish discoloration becoming paler with age on their forehead since birth. Her mother and grandmother were later examined. Her mother was 45-year-old and had a V-shaped 2Χ3 cm pinkish macule on her glabella becoming more evident during crying and after emotional reflections [Figure - 1]b. Her grandmother was 70-year-old and had a 1.5Χ3 cm paler pinkish macule on her glabellar area [Figure - 1]c. Physical examination of them were normal and family history was not supportive for other vascular malformations and internal disorders. Radiological examinations including cranial computerized tomography and abdomen ultrasonography for our patient and her mother were normal. Medial telangiectatic nevus (MTN) showed an autosomal dominant mode of transmission in three generations of family [Figure - 2].
 |
| Figure 1 : (a-c) MTN on forehead and glabella of the proband (a), her mother (b) and grandmother (c) |
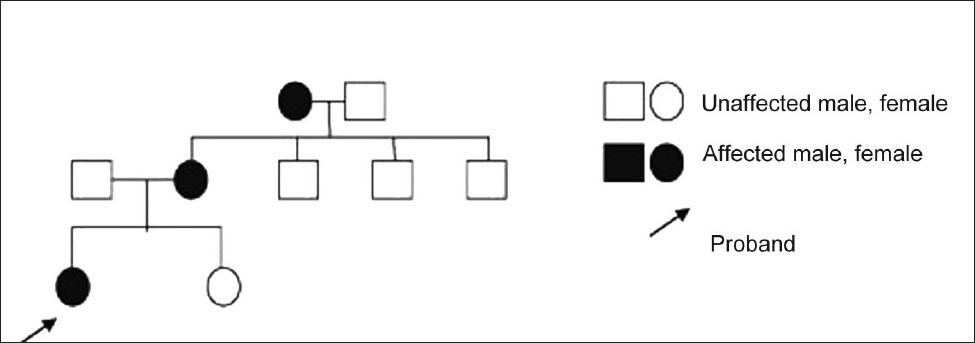 |
| Figure 2 : Pedigree of family (three generations). |
CMs presenting at birth and persisting in adulthood are of two types: (1) MTN, which is the most common form and (2) lateral telangiectatic nevus (LTN), so-called port wine stain or nevus flammeus. CMs of birth appears in 50-74% of all newborn infants as irregular patches ranges salmon pink to red in color that is located primarily on the medial part of glabello-frontal( angel′s kiss), and occipito-nuchal regions of head (stork bite) or lumbosacral areas (salmon patch). [5],[6] They are sometimes termed ′′fading macular stains′′ rather than true CMs because these lesions typically lighten significantly or disappear with in the first few years. If the capillary lesions of AK or the others do not involute during the first 5 years of life, they are called persistent MTN or if the lesions become much lighter and smaller, in time they are called as residual MTN. In the literature MTN is detected in 40-55% of normal adults particularly those on the nape of the neck. [1],[2],[3],[4] Van Baar et al.[7] supposed that 57.5% of stork bite at the nape persist throught life. However the macular stains of AK persisting in adulthood as MTN have been reported rarely in the literature. MTN are associated with other abnormalities such as umbilical hernias and hyperextensions of the joints as well odontodysplasia, multiple hamartomas and intracranial malformations, meningoencephalocele, meningomyelocele, spinal dysraphism, trisomy 13-15, Beckwith-Wiedemann syndrome, Down syndrome, mega cisterna magna, and craniofacial synostosis. [1],[3],[4] There was no clinical sign of these malformations and diseases in our patient and her family.
Histologically CMs are composed of capillary-like vessels that are dilated and/or increased in numbers. They have been suggested to be remnants of unmodified primitive capillary plexus. In contrast, neuronal marking is significantly decreased, suggesting that the lack of innervation may be the dilatation of the cutaneous capillaries. Linkage analysis recently led to the identification of a locus on 5q 13-22. [1],[2],[3],[4]
| 1. |
Pasyk KA, Wlodarczyk SR, Jacobczak MM, Kurek M, Aughton DJ. Familial medial telangiectatic nevus: variant of nevus flammeus-port-wine stain. Plast Reconstr Surg 1993;9:1032-41.
[Google Scholar]
|
| 2. |
Brouillard P, Vikkula M. Vascular malformations: localized defects in vascular morphogenesis. Clin Genet 2003;63:340-351.
[Google Scholar]
|
| 3. |
Cordoro KM, Speetzen LS, Koerper MA, Frieden IJ. Physiologic changes in vascular birthmarks during early infancy: Mechanisms and clinical implications. J Am Acad Dermatol 2009;60:669-75.
[Google Scholar]
|
| 4. |
Garzon MC, Huang JT, Enjolras O, Frieden IJ. Vascular malformations. J Am Acad Dermatol 2007;56:353-70.
[Google Scholar]
|
| 5. |
Pasyk KA. Familial multiple lateral telangiectatic nevi (port-wine stains or nevi flammei). Clin Genet 1992;41:197-201.
[Google Scholar]
|
| 6. |
Happle R. What is a capillary malformation? J Am Acad Dermatol 2008; 59: 1077-9.
[Google Scholar]
|
| 7. |
Van BH, Perret CM, Happle R. Nuchal nevi flammei and alopecia areata. Dermatologica 1989;179:52-3.
[Google Scholar]
|
Fulltext Views
4,583
PDF downloads
1,758





![[Figure - 1]](#fig_ijdvl_2010_76_5_592_69098_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2010_76_5_592_69098_f2.jpg){kind=link}