Translate this page into:
Angioma serpiginosum in a bilateral distribution with acral involvement: An uncommon presentation
2 Department of Pathology, University College of Medical Sciences, GTB Hospital, University of Delhi, New Delhi, India
Correspondence Address:
Deepika Pandhi
Department of Dermatology and STD, University College of Medical Sciences, GTB Hospital, University of Delhi, New Delhi - 110 095
India
| How to cite this article: Jakhar D, Pandhi D, Singal A, Sharma S. Angioma serpiginosum in a bilateral distribution with acral involvement: An uncommon presentation. Indian J Dermatol Venereol Leprol 2018;84:338-341 |
Sir,
Angioma serpiginosum is a vascular nevus of superficial capillaries characterized by minute red to copper-colored macules in clusters or in a serpiginous pattern,[1] resulting from congenital hyperplasia or ectasia of preexisting superficial dermal capillaries. The condition usually arises before 20 years of age and thereafter it reaches a state of relative stability.[2] Herein, we report a case of angioma serpiginosum with characteristic clinical presentation involving both upper limbs, trunk, palms and nails.
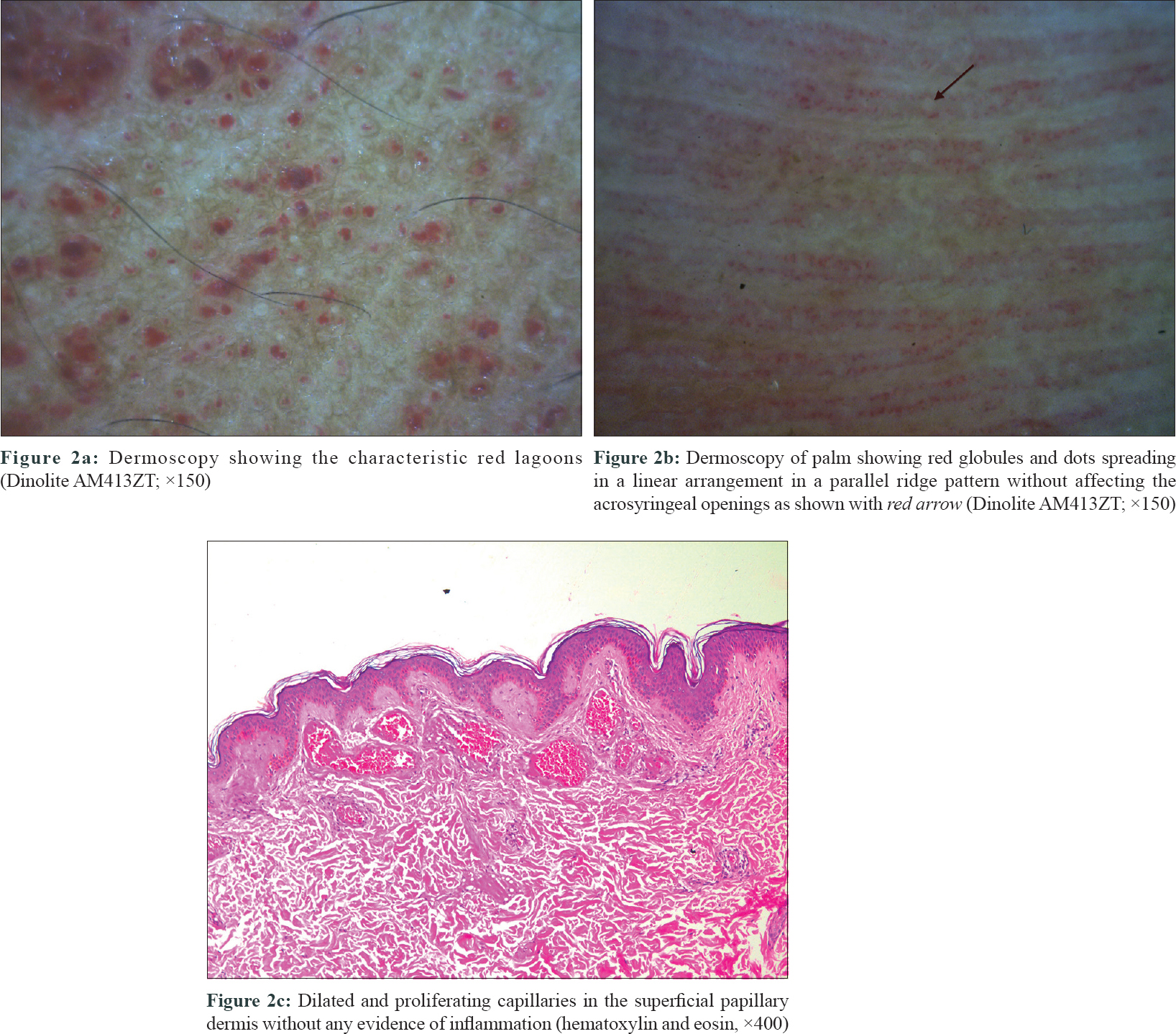
An 18-year-old man, born out of nonconsanguineous parentage, second in order of birth, presented to our outpatient Department (OPD) with red-colored lesions on both upper limbs, chest and upper back for the last 8 years. Initially there was a single lesion on the left arm which subsequently progressed in size and number to involve both the upper limbs and chest. He reported a rapid progression in the last 3 years. There was no history of any systemic complaints. Dermatological examination revealed pin-point to pin-head-sized erythematous discrete to coalescent macules in a serpiginous pattern distributed over both upper limbs, chest[Figure - 1]a, upper trunk and palms [Figure - 1]b, [Figure - 1]c, [Figure - 1]d. Erythema was also noticed on the middle finger nail of left hand [Figure - 1]e. On diascopy, the lesions were nonblanchable. No other part of the body was involved including the lower limbs. Hair and mucosae were spared. Systemic examination was within normal limits. A differential diagnoses of angioma serpiginosum and bilateral nevoid telangiectasia was made. Dermoscopy of the lesions on the arm and chest showed characteristic oval to round red lagoons, consistent with angioma serpiginosum [Figure - 2]a. Dermoscopy of the palmar lesions showed erythematous parallel ridged pattern with red globules and dots arranged linearly without affecting the acrosyringeal openings [Figure - 2]b. Onychoscopy of the left-hand middle fingernail showed a diffuse erythema. Histopathology revealed presence of dilated and proliferating capillaries in the superficial papillary dermis with no evidence of extravasation of erythrocytes [Figure - 2]c. Rest of the hematological, biochemical, radiological and systemic workup was noncontributory. On the basis of clinical, dermoscopic and histopathology features, a final diagnosis of angioma serpiginosum was made.
 |
| Figure 1 |
 |
| Figure 2 |
Angioma serpiginosum is an uncommon cutaneous vascular nevus first reported by Jonathan Hutchinson in 1890, while Frain-Bell distinguished this entity from pigmentary purpura and other disorders in 1957.[1] A female preponderance has been reported and it mainly affects lower extremities and buttocks, although involvement of upper extremities has been reported, as in our case [2],[3] It predominantly has a unilateral distribution and usually involves the trunk, palms and mucosae.[3]
Bilateral nevoid telangiectasia, on the other hand, is an acquired condition usually seen in hyperestrogenic states and liver diseases that presents clinically with 'spider' telangiectasia.[4],[5] Distribution is bilaterally symmetrical and it can be associated with gastrointestinal telangiectasia, presenting as unexplained gastrointestinal bleeding.[4] Association with Hepatitis C infection and cholangiocarcinoma has also been reported.[4]
Histopathology of angioma serpiginosum shows dilated and tortuous capillaries in the papillary dermis without any evidence of inflammation or red cell extravasation, whereas bilateral nevoid telangiectasia demonstrates superficial papillary dermal telangiectasia with minimal chronic inflammation.[3],[5] Dermoscopy of angioma serpiginosum shows characteristic well-demarcated oval red lagoons.[6] Acral variant on dermoscopy demonstrates erythematous parallel ridge pattern with red globules and dots in a linear arrangement.with sparing of the acrosyringeal openings.[7],[8] Dermoscopy of unilateral nevoid telangiectasia, on the other hand, shows thin and tortuous linear vessels with absence of red lagoons.[9]
Both dermoscopic and histopathologic findings in our case were consistent with the diagnosis of angioma serpiginosum.
Etiology of this condition remains obscure. Role of estrogen has been suggested in the etiopathogenesis of both angioma serpiginosum and nevoid telangiectasia.[2],[5] The proliferative effect of estrogen on the vascular endothelial cells support this hypothesis.[2] However, absence of estrogen and progesterone receptors on the involved blood vessels in angioma serpiginosum has contradicted this theory.[10] Other than hormonal theory, abnormal response of capillaries to cold has also been proposed as a possible etiology.[2] This condition remains stable or partially regresses after puberty.
Treatment with pulse dye laser has shown promising results in some reports.[2],[6] Our patient has also been counselled regarding the therapeutic option of pulse dye laser.
Our case presented with an unusual bilateral asymmetrical distribution involving both upper extremities, trunk and palms, whereas this condition is predominantly unilateral. Another unique feature of our case was possible involvement of the nail bed that manifested as nonblanching erythema in contiguity with palmar lesions. Onychoscopy showed diffuse erythema of nail bed. The patient, however, refused nail biopsy. To the best of our knowledge, this unique distribution of angioma serpiginosum has not been reported yet in the literature.
The rarity of our case and the role of noninvasive dermoscopy in differentiating angioma serpiginosum from bilateral nevoid telangiectasia has prompted us to report this case. This distinction is especially pertinent as the latter is more likely to be associated with underlying pathologies.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Barker LP, Sachs PM. Angioma serpiginosum, a comparative study. Arch Dermatol 1965;92:613-20.
[Google Scholar]
|
| 2. |
Bhushan P, Thatte SS, Singh A. Angioma serpiginosum: A case series of 4 patients. Indian J Dermatol Venereol Leprol 2016;82:588.
[Google Scholar]
|
| 3. |
Sancheti K, Das A, Podder I, Gharami RC. Angioma serpiginosum in a patchy and Blaschkoid distribution: A rare condition with an unconventional presentation. Indian J Dermatol 2016;61:570-2.
[Google Scholar]
|
| 4. |
Jee H, Kim TG, Kim DS, Kim DY, Lee MG. Acquired bilateral nevoid telangiectasia: Report of 9 cases. Eur J Dermatol 2013;23:736-7.
[Google Scholar]
|
| 5. |
Tang SJ, Faughnan ME, Marcon NE. Bilateral nevoid telangiectasia syndrome. Gastrointest Endosc 2004;60:468-71.
[Google Scholar]
|
| 6. |
Ilknur T, Fetil E, Akarsu S, Altiner DD, UlukuşC, GüneşAT, et al. Angioma serpiginosum: Dermoscopy for diagnosis, pulsed dye laser for treatment. J Dermatol 2006;33:252-5.
[Google Scholar]
|
| 7. |
Freites-Martinez A, Martinez-Sanchez D, Tardío JC, Huerta-Brogeras M, Borbujo J. Dermoscopy of acral angioma serpiginosum. Dermatol Online J 2014;21. pii: 13030/qt72t147pn.
[Google Scholar]
|
| 8. |
Freites-Martinez A, Moreno-Torres A, Núñez AH, Martinez-Sanchez D, Huerta-Brogeras M, Borbujo J, et al. Angioma serpiginosum: Report of an unusual acral case and review of the literature. An Bras Dermatol 2015;90 3 Suppl 1:26-8.
[Google Scholar]
|
| 9. |
Das D, Nayak CS, Tambe SA. Blaschko-linear angioma serpiginosum. Indian J Dermatol Venereol Leprol 2016;82:335-7.
[Google Scholar]
|
| 10. |
Bayramgurler D, Filinte D, Kiran R. Angioma serpiginosum with sole involvement. Eur J Dermatol 2008;18:708-9.
[Google Scholar]
|
Fulltext Views
3,625
PDF downloads
3,637





![[Figure - 1]](#fig_ijdvl_2018_84_3_338_227616_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_3_338_227616_f2.jpg){kind=link}