Translate this page into:
Annular elastolytic giant cell granuloma treated with topical pimecrolimus
2 Department of Laboratory Medicine, Institute of Pathological Anatomy, University Hospital of Santa Maria della Misericordia, Udine, Italy
Correspondence Address:
Giuseppe Stinco
Department of Experimental and Clinical Medicine, Institute of Dermatology, University of Udine, Ospedale "San Michele", Piazza Rodolone 1, 33013 Gemona del Friuli, Udine
Italy
| How to cite this article: Errichetti E, Stinco G, Avellini C, Patrone P. Annular elastolytic giant cell granuloma treated with topical pimecrolimus. Indian J Dermatol Venereol Leprol 2014;80:475-476 |
Sir,
Annular elastolytic giant cell granuloma is a rare granulomatous skin disease characterized by loss of elastic fibers along with elastophagocytosis by multinucleated giant cells. It clinically presents as small papules which evolve into annular and serpiginous plaques that have slightly raised borders. The centre of the plaque may show hypopigmentation or atrophic changes or both. These are found most commonly over the sun-exposed areas but can be seen over sun-protected areas as well. The other clinical variants include a pure papular form with absence of centrifugal annular lesions and those with reticular, brown to livid, partly atrophic skin lesions. [1],[2] The etiopathogenesis of this condition is not clear. It is thought that ultraviolet radiation, heat or other unknown factors transform the antigenicity of the elastic fibers thus inducing a cellular immune response. [3] The condition usually follows a chronic course, although cases of spontaneous remission have been described. The treatment remains a challenge and several therapeutic modalities have been tried. These include topical, intralesional and systemic steroids, clofazimine, cryotherapy, dapsone, cyclosporine A, methotrexate, psoralen plus ultraviolet A therapy, narrowband ultraviolet B therapy, retinoids, fumaric acid esters, antimalarials, topical calcineurin inhibitors and tranilast alone or in combination with pimecrolimus. [1],[2],[3],[4],[5] We report a case of annular elastolytic giant cell granuloma successfully treated with topical pimecrolimus.
A 63-year-old man with complained of two gradually increasing mildly itchy, annular plaques over the right parietal and occipital scalp for 4 months. The lesion over the parietal scalp appeared first and measured 11 cm in diameter while the other appeared a month later and was 4 cm wide. On examination, these annular plaques had slightly raised, brownish, serpiginous borders and a hypopigmented atrophic center [Figure - 1]a and b. There were no other skin or mucosal lesions. Skin biopsy revealed a non-palisading granulomatous infiltrate in the upper dermis with many multinucleated giant cells and signs of elastophagocytosis [Figure - 2]a and b. Van Gieson special staining revealed loss of elastic fibers in the areas of granulomatous infiltrate [Figure - 2]c. On the basis of clinical and histopathological data, a diagnosis of annular elastolytic giant cell granuloma was made. The patient was treated with pimecrolimus 1% cream twice daily. The lesions resolved with residual atrophy after 3 weeks after which we stopped therapy [Figure - 1]c and d. There was no recurrence at follow up two months later.
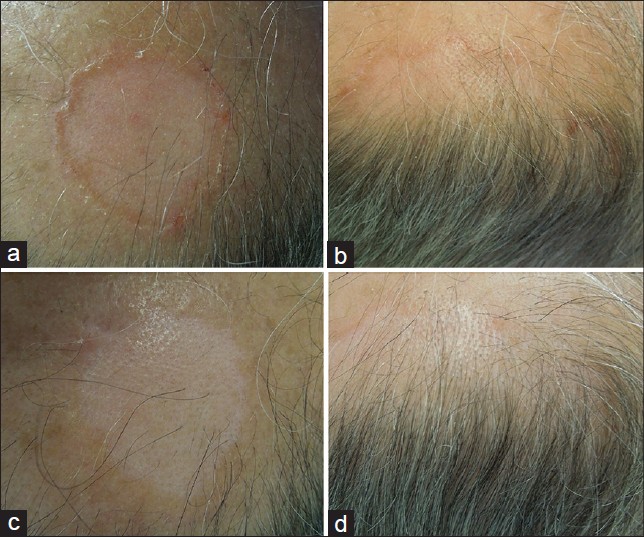 |
| Figure 1: Sharply demarcated annular plaques with slightly raised, brownish, serpiginous borders and hypopigmented, atrophic center localized over the, (a) occipital and, (b) right parietal areas of the scalp at the first visit and, (c and d) after 3 weeks of therapy with topical pimecrolimus |
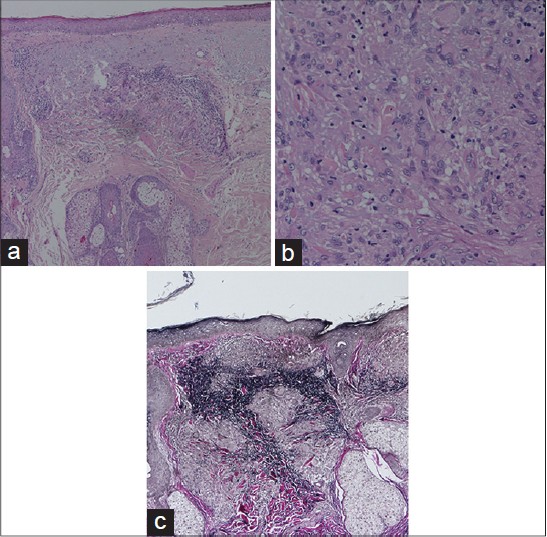 |
| Figure 2: (a) Non palisading granulomatous infi ltrate composed predominantly of multinucleated giant cells located in upper reticular dermis (H and E, ×40), (b) magnified view of multinucleated giant cells with signs of elastophagocytosis (H and E, ×200), (c) loss of elastic fibers in the areas of granulomatous infiltrates (Van Gieson staining, ×40) |
The treatment of annular elastolytic giant cell granuloma is empirical as there is no standard therapy for this chronic disorder. Limited areas of involvement are treated topically, usually with corticosteroids. However prolonged treatment with topical steroids is not always effective and leads to cutaneous atrophy, a finding often already present in this condition. [1] Other topical therapies include the calcineurin inhibitors tacrolimus and pimecrolimus. [1],[3] However, the efficacy of pimecrolimus has been demonstrated only in association with oral tranilast, an anti-allergic drug which may directly affect the activity of cells of the monocyte macrophage line. [3] The mechanism by which calcineurin inhibitors work in this condition is not clear. Several hypotheses have been proposed which include reduction in the number of lesional CD4+ T-cells, decreased production of cytokines such as interleukin-4, interleukin-13, macrophage colony stimulating factor and γ-interferon, and inhibition of the cellular immune reaction inducing granulomas around elastic fibers. [1],[3]
Although we cannot exclude a spontaneous regression of disease, the significant clinical improvement observed in our case shortly after starting topical pimecrolimus suggests the efficacy of this drug and indicates its possible use as monotherapy. Further studies and reports are needed to confirm these assumptions.
| 1. |
Rongioletti F, Baldari M, Burlando M, Parodi A. Papular elastolytic giant cell granuloma: Report of a case associated with monoclonal gammopathy and responsive to topical tacrolimus. Clin Exp Dermatol 2010;35:145-8.
[Google Scholar]
|
| 2. |
Can B, Kavala M, Türkoðlu Z, Zindancý I, Topaloðlu F, Zemheri E. Successful treatment of annular elastolytic giant cell granuloma with hydroxychloroquine. Int J Dermatol 2013;52:509-11.
[Google Scholar]
|
| 3. |
Lee HW, Lee MW, Choi JH, Moon KC, Koh JK. Annular elastolytic giant cell granuloma in an infant: Improvement after treatment with oral tranilast and topical pimecrolimus. J Am Acad Dermatol 2005;535 Suppl 1:S244-6.
[Google Scholar]
|
| 4. |
Espiñeira-Carmona MJ, Arias-Santiago S, Aneiros-Fernández J, Fernández-Pugnaire MA, Naranjo-Sintes R, Aneiros-Cachaza J. Annular erythematous papules in the neckline. Dermatol Online J 2011;17:7.
[Google Scholar]
|
| 5. |
Babuna G, Buyukbabani N, Yazganoglu KD, Baykal C. Effective treatment with hydroxychloroquine in a case of annular elastolytic giant cell granuloma. Indian J Dermatol Venereol Leprol 2011;77:110-1.
[Google Scholar]
|
Fulltext Views
3,500
PDF downloads
1,933





![[Figure - 1]](#fig_ijdvl_2014_80_5_475_140331_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_5_475_140331_u2.jpg){kind=link}