Translate this page into:
Bazex-Dupré-Christol syndrome: First report in an Indian family
2 Department of Pathology, Venereology and Leprology, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India
Correspondence Address:
Payal Chauhan
Department of Dermatology, Venereology and Leprology, All India Institute of Medical Sciences, Rishikesh, Uttarakhand
India
| How to cite this article: Chauhan P, Meena D, Dhanta A, Kansal NK, Durgapal P. Bazex-Dupré-Christol syndrome: First report in an Indian family. Indian J Dermatol Venereol Leprol 2018;84:451-456 |
Sir,
Bazex-Dupré-Christol syndrome is a rare X-linked dominant syndrome, characterized by the triad of congenital hypotrichosis, follicular atrophoderma and the development of basal cell carcinoma. Other reported features of the syndrome include multiple milia over the face, hypohidrosis, characteristic facies, atopic diathesis with comedones and hyperpigmentation of the forehead.[1] We were unable to find a case report of this syndrome in an Indian family on detailed literature search. Herein, we report an Indian family with this syndrome, spanning multiple generations with three afflicted patients examined by us, personally.
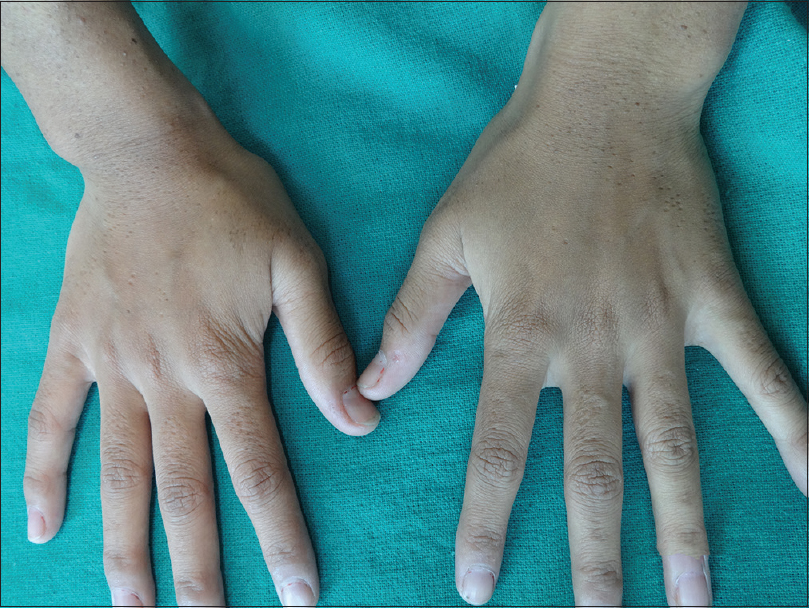
A 60-year-old male [individual III-3, [Figure - 1] presented with multiple raised, hyperpigmented lesions over his face, originating 20 years back. These lesions were increasing in number, ever since. He also complained of multiple pin point depressions over his face, arms and dorsal aspect of hands since childhood. Complaints of sparse hair and decreased sweating since childhood were also elicited. Presence of similar lesions in his daughter and granddaughter prompted him to seek medical advice. He also gave history of similar complaints in his mother, brother and grandmother. On examination, the index case had multiple, well defined hyperpigmented papules and plaques over the face [Figure - 2]. Few lesions had arolling border with central ulceration [Figure - 3]. He also had multiple ice pick depressions over the face, arms and dorsal aspect of hands [Figure - 2],[Figure - 4] and [Figure - 5]. The scalp hair was noted to be sparse and coarse [Figure - 6]. The same was noted over the eyebrows, but the eyelashes were normal in this regard [Figure - 2]. On examination of the 31-year-old daughter of the index case [individual IV-2 in [Figure - 1], there were multiple ice pick depressions over the face and dorsal aspect of hands, along with multiple milia and comedones over the face [Figure - 7], [Figure - 8], [Figure - 9]. The scalp hair was coarse and sparse. The patient had camouflaged the sparseness of the eyebrows with a black pencil [Figure - 7]. There was a single 0.5 cm × 0.5 cm hyperpigmented papule below her left eye, [Figure - 7] which had appeared 5 years back. Examination of the 10-year-old granddaughter of the index case [individual V-1 in [Figure - 1]] revealed multiple milia and comedones over her face [Figure - 10]. The scalp and eyebrow hair were found to be sparse, resembling those of her mother and grandfather. She also had multiple ice pick depressions over the dorsal aspect of hands [Figure - 11]. All three cases had long thin noses, with prominent columella and hypoplastic nasal alae. There was no evidence of acral erythema or palmoplantar pits in any of the patients. Skeletal abnormalities were ruled out with normal skiagrams. Odontogenic cysts were ruled on dental consultation. The son of the index case who accompanied the family showed no abnormality on mucocutaneous examination. Hair microscopy of all the cases was unremarkable. Considering the history and clinical examination of the family members, a provisional diagnosis of Bazex-Dupré-Christol syndrome was made. Dermoscopy of the ulcerated plaque over right cheek showed blue-gray ovoid nests, blue-gray globules, multiple telangiectasias and erosions [Figure - 12]. Dermoscopic examination of the hyperpigmented facial papule of the daughter revealed maple leaf-like areas, spoke wheel areas and arborizing vessels [Figure - 13]. Given the predilection for development of basal cell carcinoma in the syndrome, histopathological examination of the hyperpigmented papule of both the index case and his daughter was performed with other differentials, viz., seborrheic keratosis, actinic keratosis and melanocytic nevi. The histopathology in both the cases showed a tumor arising from the basal layer, comprising irregular nests and sheets of tumour cells with peripheral palisading and retraction artifacts. The tumor cells had high nucleo-cytoplasmic ratio, nuclear hyperchromasia and scant cytoplasm [Figure - 14] and [Figure - 15]. The histopathological diagnosis was consistent with basal cell carcinoma. The overall history, clinical and histopathological examination of the family confirmed the diagnosis of Bazex-Dupré-Christol syndrome. The index case was referred to the plastic surgery department for excision of the basal cell carcinomas. Counselling was done regarding the genetic inheritance of the syndrome, along with emphasis upon regular follow up for early detection of basal cell carcinomas, if required.
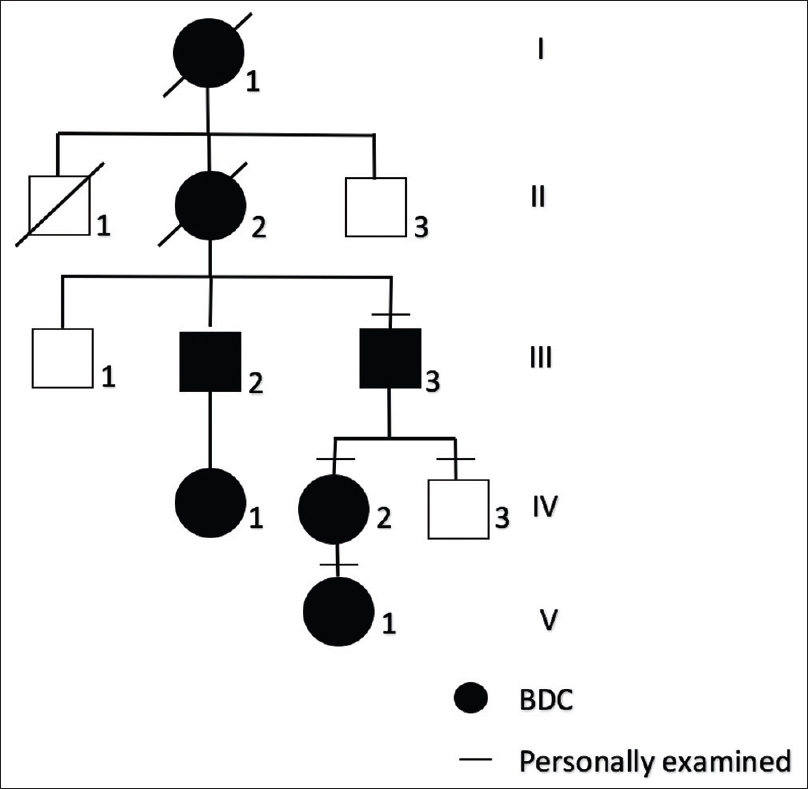 |
| Figure 1: Pedigree chart of the Indian family. The index patient is indicated by an arrow. The horizontal bars indicate patients who were seen by the authors |
 |
| Figure 2: Multiple well-defined hyperpigmented papules, ice pick scars over face along with long thin nose with prominent columella in the index case. Eyebrows found to be sparse |
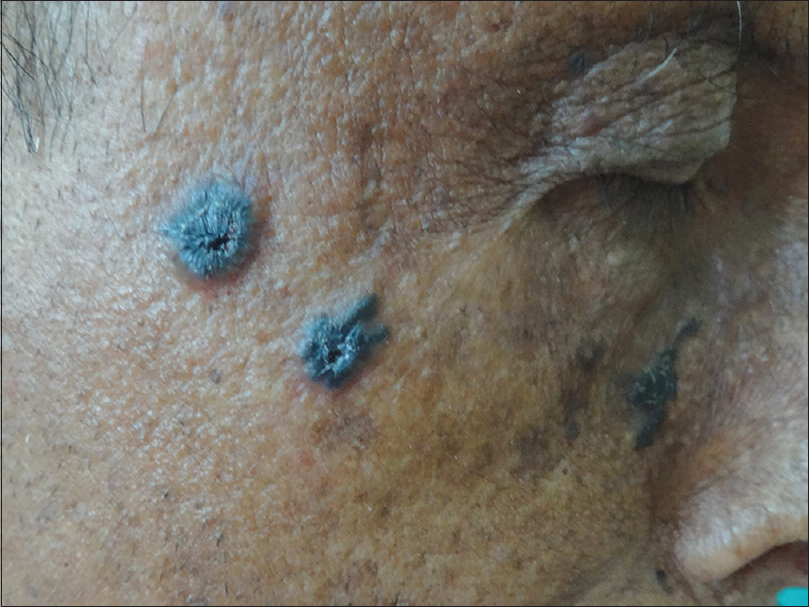 |
| Figure 3: Closer view of the hyperpigmented papules showing rolling border and central ulceration |
 |
| Figure 4: Ice pick depressions over arms of index case |
 |
| Figure 5: Ice pick depressions over dorsal aspect of hands |
 |
| Figure 6: Sparse and coarse scalp hair noted |
 |
| Figure 7: Multiple facial milia, characteristic appearance of nose and sparse eyebrows in the daughter of index case. Single hyperpigmented papule present below the left eye |
 |
| Figure 8: Follicular atrophoderma over dorsal aspect of hands of right hand of daughter of the index case |
 |
| Figure 9: Follicular atrophoderma over dorsal aspect of hands of left hand of daughter of the index case |
 |
| Figure 10: Multiple milia, comedones, sparseness of eyebrows and long nose with prominent columella seen in granddaughter of the index case |
 |
| Figure 11: Ice pick depressions over dorsal aspect of both hands of granddaughter of the index case |
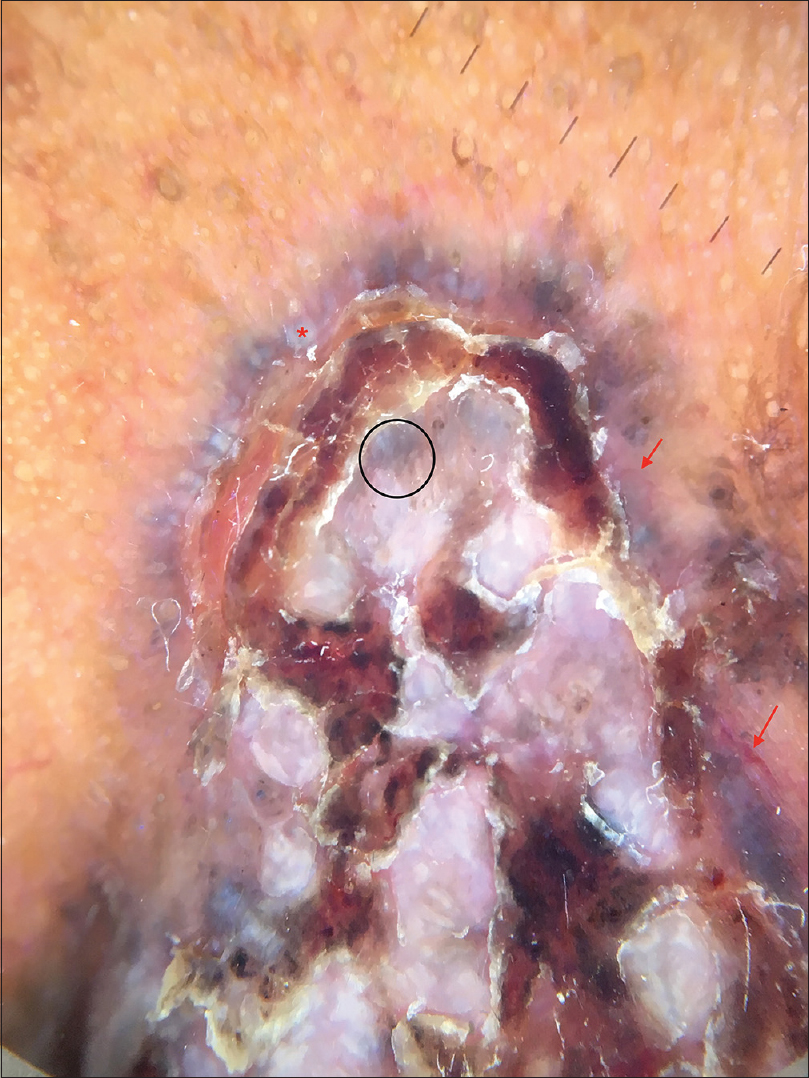 |
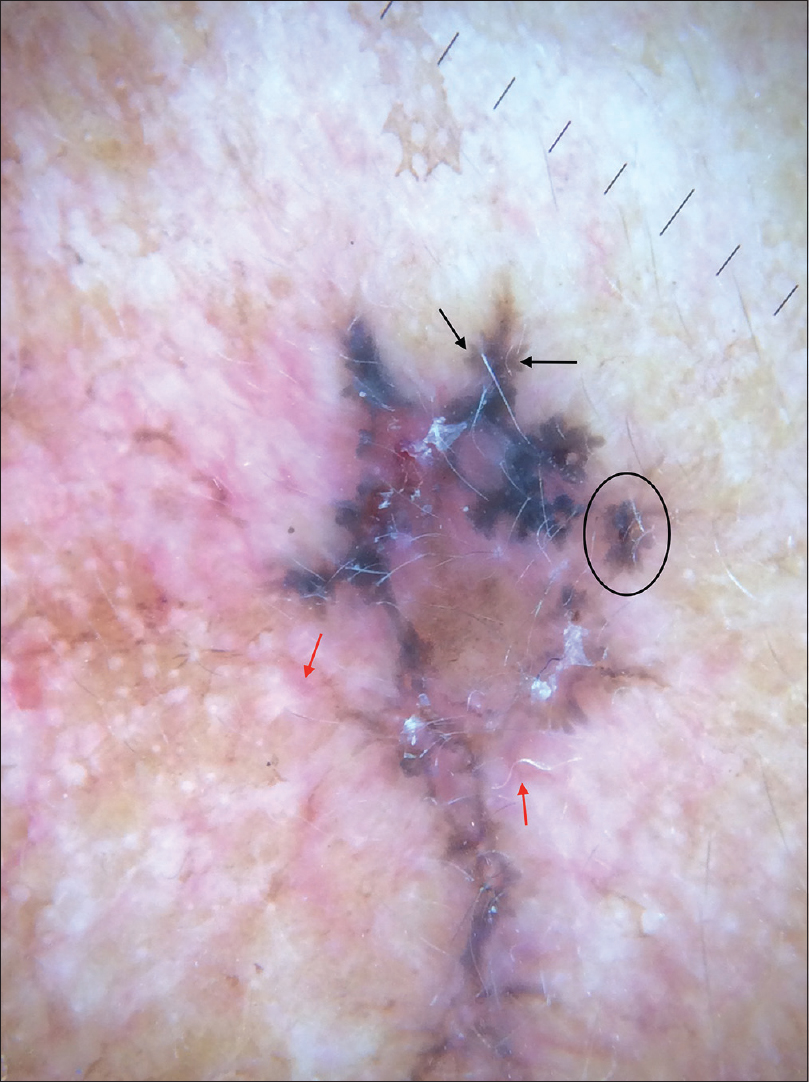
| Figure 12: Dermoscopy of the ulcerated plaque over right cheek showed blue–gray ovoid nests (black circle), blue–gray globules (red star), multiple telangiectasias (red arrow) and erosions |
 |
| Figure 13: Dermoscopic examination of hyper pigmented papule of the daughter revealed maple leaf- like areas (black arrow), spoke wheel areas (black circle) and arborizing vessels (red arrow) |
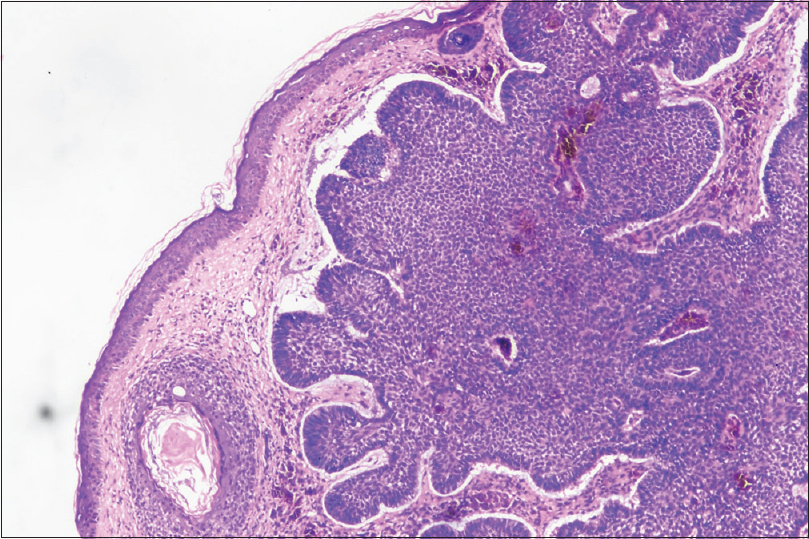 |
| Figure 14: Tumour arising from the basal layer comprising of irregular nests and sheets of tumour cells with peripheral palisading, retraction spaces around the tumour and pigment deposition [hematoxylin and eosin (H and E), ×100)] |
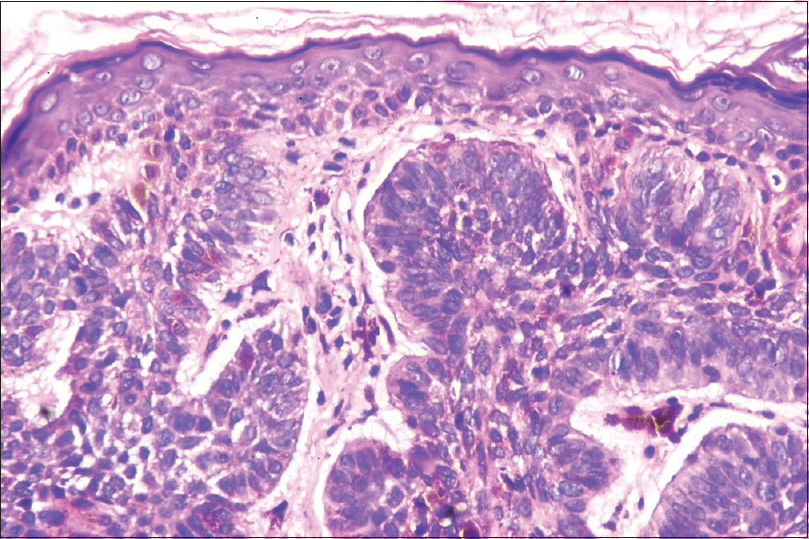 |
| Figure 15: Index case showing high nucleo-cytoplasmic ratio, nuclear hyperchromasia and scant cytoplasm seen in the tumour cells (H and E, ×400) |
Bazex-Dupré-Christol syndrome (OMIM 301845) was first described in 1964 by Bazex et al., involving hair follicle structures.[2] Though the exact genetic defect is not yet known, inheritance of the syndrome is thought to be transmitted in an X-linked dominant pattern with genetic defect localizing to Xq.[1],[3] This mode of inheritance explains the absence of male-to-male transmission of the disease, as seen in the present family. In the original case report, Bazex-Dupré-Christol syndrome was described as a triad of follicular atrophoderma, hypotrichosis and basal cell carcinomas.[2] Milia, hypohidrosis, pinched nose with hypoplastic nasal alae and prominent columella, atopic diathesis with comedones, keratosis pilaris, joint hypermobility and hyperpigmentation of the face, epidermal cysts and trichoepitheliomas are the other reported clinical signs which reflect the intra- and inter-familial phenotypic variations of the syndrome.[1],[3],[4] Till date, around 20 sporadic and familial cases have been reported worldwide.[1] We were unable to find a case report of Bazex-Dupré-Christol syndrome from India, on a detailed literature search. Tharini et al., reported a 10-month-old male with congenital hypotrichosis of scalp, absence of eyebrows and eyelashes, multiple milia over face and extremities with a diagnosis of unclassified ectodermal dysplasia.[5] The patient had palmoplantar pits, which were absent in our patients. Follicular atrophoderma, which was seen in all our patients, was not seen in their case. In previous reports, follicular atrophoderma and hypotrichosis were reported in 85% of patients, hypohidrosis in 54%, milia in 65% and development of basal cell carcinoma in 40–50% of patients.[6],[7] All the above-mentioned findings were present in the reported family. Hypotrichosis can be appreciated shortly after birth, either confined to the scalp or affecting eyebrows as well. Though absent our patients, hair shaft anomalies have also been reported, namely pili torti and trichorrhexis nodosa.[4],[7] Follicular atrophoderma manifesting during early childhood usually affects the dorsal side of the hands and feet, the extensor surfaces of the elbows and knees. BCCs commonly develop in the second decade of life, and beyond, with the face being the most frequent site of affliction. Basal cell carcinomas may show aggressive behaviour with a tendency to relapse. Basal cell nevi and trichoepithelioma are the other basaloid proliferations described in patients with Bazex-Dupré-Christol syndrome.[4],[7]
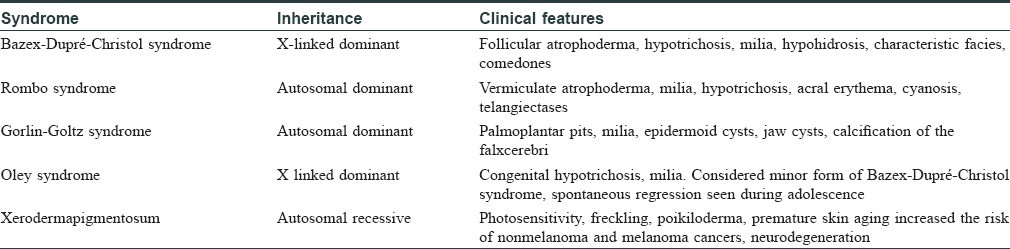
When faced with familial occurrence of basal cell carcinoma as in our report, the differentials to be kept in mind include Rombo syndrome, Gorlin syndrome, Oley syndrome and xeroderma pigmentosum.[4] These differential diagnoses have been discussed in [Table - 1]. Chondrodysplasia punctata is another X-linked dominant disorder that can present with follicular atrophoderma. Presence of ichthyotic lesions, cicatricial alopecia, cataracts, and skeletal abnormalities (short stature, asymmetric shortening of the limbs, epiphyseal stippling) help in differentiating it from Bazex-Dupré-Christol syndrome.[8]
The lack of knowledge of the causative gene precludes preventive measures such as predictive genetic testing in Bazex-Dupré-Christol syndrome. In a study by Pujol et al., prophylactic 13 cis-retinoid, topical retinoid acid and etretinate were used for tumor prevention, without much success.[9] Counselling regarding strict solar photoprotection, along with application of high factor (SPF 30+) sunscreens is paramount, and goes a long way in prevention of malignancy. Surgical excision remains the first line of management in a clinically and histopathologically confirmed cases of basal cell carcinoma.[4] Cryotherapy and imiquimod comprise other therapeutic options, especially in early basal cell carcinoma.[7] As mentioned earlier, the index case was referred to Plastic Surgery Department of the hospital for excision. We were unable to find any report of Bazex-Dupré-Christol syndrome from the Indian subcontinent, on detailed literature search. This case is being reported with the intention to increase awareness regarding this syndrome, so that a thorough clinical examination is undertaken, even in cases of trivial conditions such as milia, when these are extensive, or associated with hypotrichosis or follicular atrophoderma, to rule out basal cell carcinomas.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Yung A, Newton-Bishop JA. A case of Bazex-Dupré-Christol syndrome associated with multiple genital trichoepitheliomas. Br J Dermatol 2005;153:682-84.
[Google Scholar]
|
| 2. |
Bazex A, Dupre A, Christol B. Genodermatosis complex of indeterminate type associating a hypotrichosis, a generalized atrophodermal state and multiple cutaneous degenerations (epitheliomas-basocellular). Bull Soc Fr. Syphilol 1964;71:206.
[Google Scholar]
|
| 3. |
Parren LJ, Frank J. Hereditary tumour syndromes featuring basal cell carcinomas. Br J Dermatol 2011;165:30-4.
[Google Scholar]
|
| 4. |
Abuzahra F, Parren LJMT, Frank J. Multiple familial and pigmented basal cell carcinomas in childhood – Bazex–Dupre'–Christol syndrome. J Eur Acad Dermatol Venereol 2012;26,117-21.
[Google Scholar]
|
| 5. |
Tharini G K, Subashini M, Roshan S A, Prabhavathy D, Jayakumar S. Congenital hypotrichosis, eruptive milia, and palmoplantar pits: A case report with review of literature. Int J Trichol 2012;4:32-5.
[Google Scholar]
|
| 6. |
Glaessl A, Hohenlautner U, Landthaler M, Vogt T. Sporadic Bazex-Dupré-Christol-like syndrome: Early onset basal cell carcinoma, hypohidrosis, hypotrichosis, and prominent milia. Dermatol Surg 2000; 26:152-54.
[Google Scholar]
|
| 7. |
Ghafoor R, Anwar MI, Tahir M. Bazex-Duppré-Christol syndrome: A case report. Iran J Dermatol 2015;18:29-32.
[Google Scholar]
|
| 8. |
Ozyurt K, Subasioglu A, Ozturk P, Inci R, Ozkan F, Bueno E, et al. Emopamil binding protein mutation in Conradi-Hünermann-Happle syndrome representing plaque-type psoriasis. Indian J Dermatol 2015;60:216.
[Google Scholar]
|
| 9. |
Pujol RM, Nadal C, Matias-Guiu X, Peyrí J, Ferrándiz C, Palou J, et al. Multiple follicular hamartomas with sweat gland and sebaceous differentiation, vermiculate atrophoderma, milia, hypotrichosis, and late development of multiple basal cell carcinomas. J Am Acad Dermatol 1998;39:853-7.
[Google Scholar]
|
Fulltext Views
8,890
PDF downloads
2,503





![[Figure - 1]](#fig_ijdvl_2018_84_4_451_233658_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_4_451_233658_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2018_84_4_451_233658_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2018_84_4_451_233658_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2018_84_4_451_233658_f5.jpg){kind=link}
![[Figure - 6]](#fig_ijdvl_2018_84_4_451_233658_f6.jpg){kind=link}
![[Figure - 7]](#fig_ijdvl_2018_84_4_451_233658_f7.jpg){kind=link}
![[Figure - 8]](#fig_ijdvl_2018_84_4_451_233658_f8.jpg){kind=link}
![[Figure - 9]](#fig_ijdvl_2018_84_4_451_233658_f9.jpg){kind=link}
![[Figure - 10]](#fig_ijdvl_2018_84_4_451_233658_f10.jpg){kind=link}
![[Figure - 11]](#fig_ijdvl_2018_84_4_451_233658_f11.jpg){kind=link}
![[Figure - 12]](#fig_ijdvl_2018_84_4_451_233658_f12.jpg){kind=link}
![[Figure - 13]](#fig_ijdvl_2018_84_4_451_233658_f13.jpg){kind=link}
![[Figure - 14]](#fig_ijdvl_2018_84_4_451_233658_f14.jpg){kind=link}
![[Figure - 15]](#fig_ijdvl_2018_84_4_451_233658_f15.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2018_84_4_451_233658_t16.jpg){kind=link}