Translate this page into:
Beard involvement in a man with frontal fibrosing alopecia
2 Department of Dermatology, School of Medicine, Hospital Universitario Virgen Macarena, Seville, Spain
Correspondence Address:
Rafael Salido-Vallejo
M.D. C/Jose Manuel Rodriguez L�pez, No. 7, C�rdoba - 302 14005
Spain
| How to cite this article: Salido-Vallejo R, Garnacho-Saucedo G, Moreno-Gimenez JC, Camacho-Martinez FM. Beard involvement in a man with frontal fibrosing alopecia . Indian J Dermatol Venereol Leprol 2014;80:542-544 |
Sir,
Frontal fibrosing alopecia is a variant of primary lymphocytic cicatricial alopecia, typically observed in postmenopausal women [1] with a few cases reported in men. [2],[3],[4] It is considered a clinical variant of lichen planopilaris producing irregular hair loss from the frontal hairline, preauricular area and eyebrows, with facial papules in the temporal area. Involvement of body hair, mainly affecting axillae, pubis and lower and upper limbs can also occur. [1],[5] We present a case of frontal fibrosing alopecia in a man with acute hair loss from the beard and limbs.
A 52-year-old man presented with a 10-year history of progressive recession of the fronto-parietal hairline in a band and marked decrease in hair on the eyebrows [Figure - 1]a and b. In addition, the patient complained of sudden, relapsing, asymptomatic, patchy hair loss from the beard [Figure - 2] and upper and lower limbs [Figure - 1]c which had started 3 years ago and continued to be active. Axillary and pubic hair were normal. Dermoscopic examination of the scalp, beard and lower limbs revealed loss of orifices, peripilar erythema and white concentric scales around the follicular papules [Figure - 3]c and d. These dermoscopic findings were more pronounced on the scalp and lower limbs than in the beard and eyebrows, where peri-pilar erythema and perifollicular scales were absent.
 |
| Figure 1: (a) Band of frontoparietal hair recession with partial loss of eyebrows. (b) Marked recession of temporal hairline with complete loss of sideburns. (c) Irregular patches devoid of hairs in lower limbs |
 |
| Figure 2: Non-inflammatory bald patches in the beard |
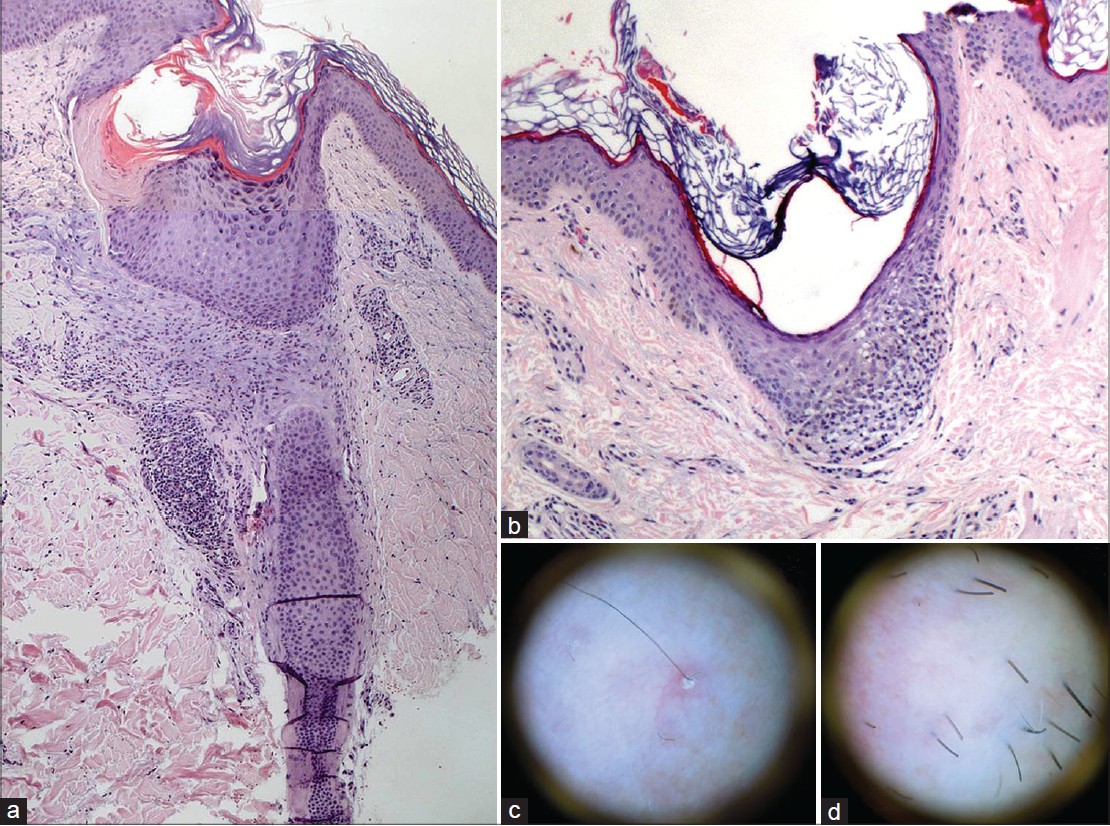 |
| Figure 3: (a) Histopathology of lower limb shows mild follicular hyperkeratosis and perifollicular lymphocytic infiltration involving infundibulum and isthmus portions of single hair follicle. (H and E, ×40) (b) Histopathology of beard (hematoxylin-eosin; original magnification ×10) shows infundibular lichenoid dermatitis with vacuolar interface changes. (H and E, ×100) (c) Dermoscopy of limb: Loss of orifices and peripilar white concentric scales around the emergence of a follicle. (d) Dermoscopy of beard: Loss of orifices with no other specific findings |
Laboratory tests including complete blood count, thyroid screen and antinuclear factor were normal. Histopathological examination of the scalp specimen revealed hair follicles replaced by fibrous tracts and a chronic lymphocytic infiltrate surrounding the follicles. The beard and lower limb biopsies were very similar to the scalp biopsy [Figure - 3]a and b. These findings led us to the diagnosis of frontal fibrosing alopecia with beard and body involvement. Various treatments were used viz. topical and oral corticosteroids, hydroxychloroquine and acitretin, which reduced the signs of inflammation but did not slow the course of the alopecia.
Frontal fibrosing alopecia is extremely unusual in men, with only 9 cases reported in the literature. [2],[3],[6],[7] It is characterized by a symmetric pattern of progressive recession of the fronto-temporal hairline and a marked decrease or complete loss of eyebrows in 73% of cases. [1] Although the "lonely hair" sign can be present in several types of cicatricial alopecia, the appearance in the fronto-parietal hairline or sideburns of single hairs that are not grouped in tufts is very specific to frontal fibrosing alopecia. [8] Acute loss of body hair has been reported in 25% of cases, [1] with no spontaneous regrowth. In men, body and sideburn [6] involvement has been described but with few reports of beard involvement. [4] As reported by Miteva and Tosti for the limbs, [5] frontal fibrosing alopecia of the beard presents as bald patches of sudden onset. Trichoscopy and histopathology are helpful in differentiating this condition from other types of alopecia with body involvement such as alopecia areata and Graham-Little-Piccardi-Lassueur syndrome, with which it may be confused.
In addition to the characteristic fronto-parieto-temporal alopecia of frontal fibrosing alopecia, our patient had large non-inflammatory alopecic plaques on the lower limbs, like those described by Miteva and Tosti, accompanied by similar patches in the beard. Dermoscopic examination revealed lonely hairs with mild asymptomatic follicular papules on the lower limbs. The involvement of the beard was similar to that observed with the eyebrows, with loss of follicular ostia and lonely hairs observed in the center of alopecic patches, but with no evident peri-follicular erythema or scaling. We found no dermoscopic signs of alopecia areata (yellow dots, cadaverised follicles or dystrophic or exclamation mark hairs).
Interestingly, we observed a slight, partial recovery of the alopecic patches on the body and in the beard. Nevertheless, the successive relapses of alopecic patches in the beard and on the limbs led to progressive scarring alopecia with no regrowth. The inflammatory infiltrate observed in the beard and on the body was less intense when compared with that detected on the scalp. This could explain the absence of inflammatory signs and pruritus, as well as the partial regrowth. Repeated episodes of subclinical inflammation would lead to the development of permanent alopecia in these locations, as occurs on the scalp but at a slower rate.
Our findings in this patient are consistent with the diagnosis of frontal fibrosing alopecia occurring as a generalized process that affected the scalp, eyebrows and other parts of the body. Clinicians should be able to recognize this condition so as to differentiate it from alopecia areata and commence appropriate treatment.
| 1. |
MacDonald A, Clark C, Holmes S. Frontal fibrosing alopecia: A review of 60 cases. J Am Acad Dermatol 2012;67:955-61.
[Google Scholar]
|
| 2. |
Kossard S, Shiell RC. Frontal fibrosing alopecia developing after hair transplantation for androgenetic alopecia. Int J Dermatol 2005;44:321-3.
[Google Scholar]
|
| 3. |
Dlova NC, Goh CL. Frontal fibrosing alopecia in an African man. Int J Dermatol 2013. [In Press].
[Google Scholar]
|
| 4. |
Vañó-Galván S, Molina-Ruiz AM, Serrano-Falcón C, Arias-Santiago S, Rodrigues-Barata AR, Garnacho-Saucedo G, et al. Frontal fibrosing alopecia: A multicenter review of 355 patients. J Am Acad Dermatol 2014;70:670-8.
[Google Scholar]
|
| 5. |
Miteva M, Camacho I, Romanelli P, Tosti A. Acute hair loss on the limbs in frontal fibrosing alopecia: A clinicopathological study of two cases. Br J Dermatol 2010;163:426-8.
[Google Scholar]
|
| 6. |
Ramaswamy P, Mendese G, Goldberg LJ. Scarring alopecia of the sideburns: A unique presentation of frontal fibrosing alopecia in men. Arch Dermatol 2012;148:1095-6.
[Google Scholar]
|
| 7. |
Samrao A, Chew AL, Price V. Frontal fibrosing alopecia: A clinical review of 36 patients. Br J Dermatol 2010;163:1296-300.
[Google Scholar]
|
| 8. |
Camacho FM. Lonely hair sign: Not specific for frontal fibrosing alopecia. Arch Dermatol 2012;148:1208-9.
[Google Scholar]
|
Fulltext Views
5,855
PDF downloads
1,673





![[Figure - 1]](#fig_ijdvl_2014_80_6_542_144183_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_6_542_144183_u2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2014_80_6_542_144183_u3.jpg){kind=link}