
Translate this page into:
Beyond the blue: A rare case of azure lunula
Corresponding author: Dr. Sudharani Chintagunta, Department of Dermatology, Venereology and Leprology, Gandhi Medical College, Hyderabad, Telangana India. schintagunta@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Koppula A, Srikanth M, Chintagunta S, Netha GNR. Beyond the blue: A rare case of azure lunula. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_307_2024
Dear Editor,
The lunula is the visible part of the distal nail matrix that extends past the proximal nail fold. It is more visible on the thumbnail and great toenail. The white colour of the lunula may be secondary to characteristics of the nail matrix and the nail bed, or the nail plate which may be attributed to thicker lunular epithelium, light diffraction by parakeratotic onychocytes, and thinner nail plate.1 Normally lunular epithelium is thicker hence the capillaries of the adjacent bed are not visible giving it a white colour. The colour of the lunula may range from white, red, green to blue.2 Azure lunula can be caused by systemic drug ingestion, for e.g. silver (argyria), zidovudine, some chemotherapeutic agents like vincristine, and hydroxyurea.
Hydroxyurea, a ribonucleotide reductase inhibitor used as a first-line agent in polycythemia vera can cause hyperpigmentation of nails and rarely bluish discolouration of the lunula. We present a case of hydroxyurea-induced blue lunula in a patient being treated for polycythemia vera.
A 25-year-old man with polycythemia vera complained of bluish discolouration of fingernails for one week. Two weeks ago oral hydroxyurea therapy 500 mg twice daily had been initiated. There was no history of consumption of any drugs of alternative medicine. On examination, the lunula on the fingernails most prominently on thumbnails showed a bluish colour [Figure 1]. Other parts of the nail plate were normal. Hyperpigmentation of the palms and soles was also noted [Figure 2]. Mucosae were normal. Onychoscopy showed a bluish hue over the lunular region of all the nails, predominantly on both the thumbnails [Figure 3]. A routine haematological examination showed haemoglobin to be 19.1 gm%. Other laboratory investigations were within the normal limits. Genetic analysis showed JAK2 positivity. Based on the history and clinical findings, a diagnosis of azure lunula secondary to hydroxyurea was made. The lunular dyschromia cleared in four months of stopping hydroxyurea.
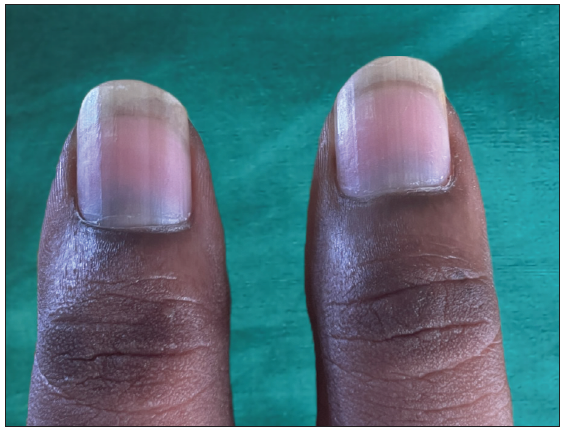
- Bluish discolouration of the lunula noted on both thumbnails.

- Patchy hyperpigmentation on both the palms.
Lunular dyschromia can be confluent or spotted or can be characterised by longitudinal coloured bands that traverse the lunula. Blue or azure lunula can be hereditary or acquired [Table 1]. Among systemic medications, chemotherapeutic agents are the most common cause of azure lunula.
| Causes of azure lunula |
|---|
| INHERITED |
| 1. Wilson disease |
| 2. Haemoglobin M disease |
| 3. Hereditary acrolabial telengectasia |
| ACQUIRED |
| 1. Argyria |
| 2. Hydroxyurea |
| 3. Zidovudine |
| 4. Phenolphthalein |
| 5. Combination chemotherapy : |
| • Cyclophosphamide, vincristine, doxorubicine, dacarbazine. |
| • 5-fluorouracil, doxorubicin, cyclophosphamide. |
| • Vinblastine, dactinomycin, bleomycin. |
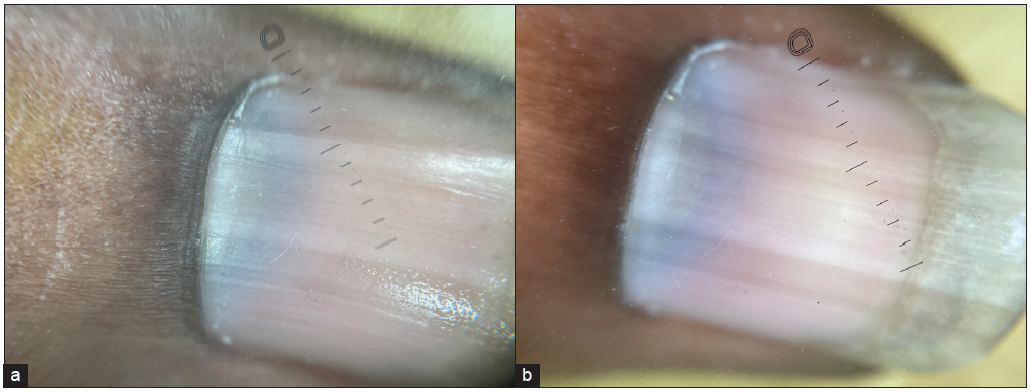
- Bluish hue on the lunula of the thumbnail 10x, dermlite Dl5. (a) Non-polarised mode, (b) Polarised mode.
Hydroxyurea is used as a chemotherapeutic agent in polycythemia vera. Long-term treatment is associated with painful skin ulcers, aphthous ulcers, non-ulcerative toxicity with erythema, and skin infiltration.3 Hydroxyurea-induced nail changes include atrophic, brittle nails, longitudinal bands, transverse bands, and diffuse darkening.4 Hydroxyurea-induced blue lunula is a rare manifestation and it usually occurs months to years after initiation of therapy. The exact pathophysiology of hydroxyurea-induced lunular pigmentation is unclear, but it can be due to the direct toxicity of the drug on the distal nail matrix or focal stimulation of melanocytes leading to the deposition of melanin.2
Hydroxyurea-induced blue lunula usually occurs after several months of therapy. In this case, the bluish discolouration of lunula was noticed two weeks into the therapy similar to the case report by Jeevan et al.2 In addition to azure lunula, which were more conspicuous on the thumbnails, the patient also presented with hyperpigmentation of palms. However, there was no discolouration of the mucosae.
Though blue lunula secondary to hydroxyurea is rare, it should be kept in mind during regular follow-up and management of the patients on hydroxyurea therapy as it is reversible on cessation of the drug and therefore helps us avoid invasive procedures.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Hydroxyurea-induced azure lunula: Case report. Journal of Dermatology and Dermatologic Surgery. 2021;25:44-5.
- [Google Scholar]
- Hydroxyurea toxicity. In: StatPearls. Treasure Island (FL): StatPearls Publishing; August 8, 2023.
- [Google Scholar]




